



Dry eye and ocular surface disease are two of the greatest areas of interest in modern eyecare. Due to this attention, we now have more diagnostic and treatment options to manage dry eye disease (DED) and ocular surface disease (OSD) than ever before.
From meibomian gland imaging studies with meibography to treatments using intense pulsed light (IPL), the ability to diagnose and treat DED and OSD has reached new heights.
Getting started with a dry eye and OSD workup
That being said, this progress may have brought with it some unforeseen consequences. One thing I am hearing more and more from eyecare providers (ECPs) is that—considering all these advancements—they feel ill-equipped to manage DED if they don’t have the latest and greatest diagnostic and treatment devices. This is an unfortunate concern, but thankfully, one that can easily be alleviated.
Although advanced testing and in-office treatment procedures are helpful in managing dry eye, they are by no means a prerequisite to initiating dry eye treatment for the majority of patients. Even in our dedicated dry eye and ocular surface disease clinic, some of the most effective diagnostic testing and treatment options I routinely use are available to ECPs in nearly any setting.
This guide discusses a simple but effective dry eye and ocular surface disease workup that is accessible to all ECPs, whether they practice in an advanced dry eye center or a primary eyecare office.
It all starts with the patient
One of the most powerful diagnostic tools we have at our disposal requires no equipment at all. The late Dr. Art Epstein was fond of saying, “Our patient is the most sensitive instrument we have.” And from my early years in practice working alongside Dr. Epstein to today, I have found this statement to hold true time and time again.
Treating DED and OSD all starts with a thorough patient history:
If you listen closely to a patient’s specific signs and symptoms, they will often lead you directly to the underlying cause of their DED.
I recommend starting by asking open-ended and broad questions such as, “How are your eyes feeling in terms of comfort? Do your eyes ever feel dry, scratchy, or irritated?” Based on their initial response, my questions become more targeted to allow me to hone in on specific conditions such as meibomian gland dysfunction (MGD) or nocturnal lagophthalmos.
Additionally, dry eye questionnaires are readily available tools that also allow you to quantify a patient’s dry eye symptoms, providing objective testing data that requires no additional testing equipment.
Considerations for the exam
Diagnosis and assessment of DED and OSD can be easily carried out with equipment and items commonly found in any practice, including a slit lamp, vital dyes, a transilluminator, and a cotton-tipped applicator. After a patient provides their history, a careful slit lamp exam is largely all that is required to diagnose the vast majority of OSD.
When assessing a patient’s ocular surface health, I recommend taking a consistent, systematic approach to evaluating the ocular surface by looking specifically at each constitutive element.
1. The lids and lashes
Although they do not traditionally receive as much attention as the cornea and conjunctiva, the eyelids and lashes play a significant role in ocular surface homeostasis. It is recommended to assess both their structure and function.
Slit lamp exam findings
Evaluating the eyelids and lashes while having the patient look straight ahead and then down will allow for the detection of numerous OSDs. When the patient looks down, lash collarettes, which are waxy, cylindrical buildups found at the base of the lashes (as seen in Figure 1), serve as the hallmark sign of Demodex blepharitis and can easily be detected.1-4
The presence of spidery telangiectatic blood vessels, also seen in Figure 1, can be suggestive of ocular rosacea.5,6 Notching, keratinization, thickening of the lid margin, or lash loss can be indicative of chronic inflammation, and the presence of saponification or foamy/frothy tears can signal the presence of bacterial blepharitis.7
Further, having the patient blink while behind the slit lamp can aid in the assessment of lid function and blinking mechanics. As the patient blinks, pay close attention to partial or incomplete blinks since they can be potential contributing factors to a patient’s dryness, as incomplete blinks are associated with DED.8 Additionally, lid position can easily be evaluated and reveal ectropion, entropion, lower lid laxity, inferior scleral show, or trichiasis.
I also highly recommend gently lifting the upper lid while the patient is looking down, as this can reveal floppy eyelid syndrome (FES) if there is excessive laxity, effortless lid eversion, or the lid easily pulls away from the globe.9
Figure 1 highlights a patient with lash collarettes and spidery telangiectatic blood vessels, potentially indicative of Demodex blepharitis and ocular rosacea.

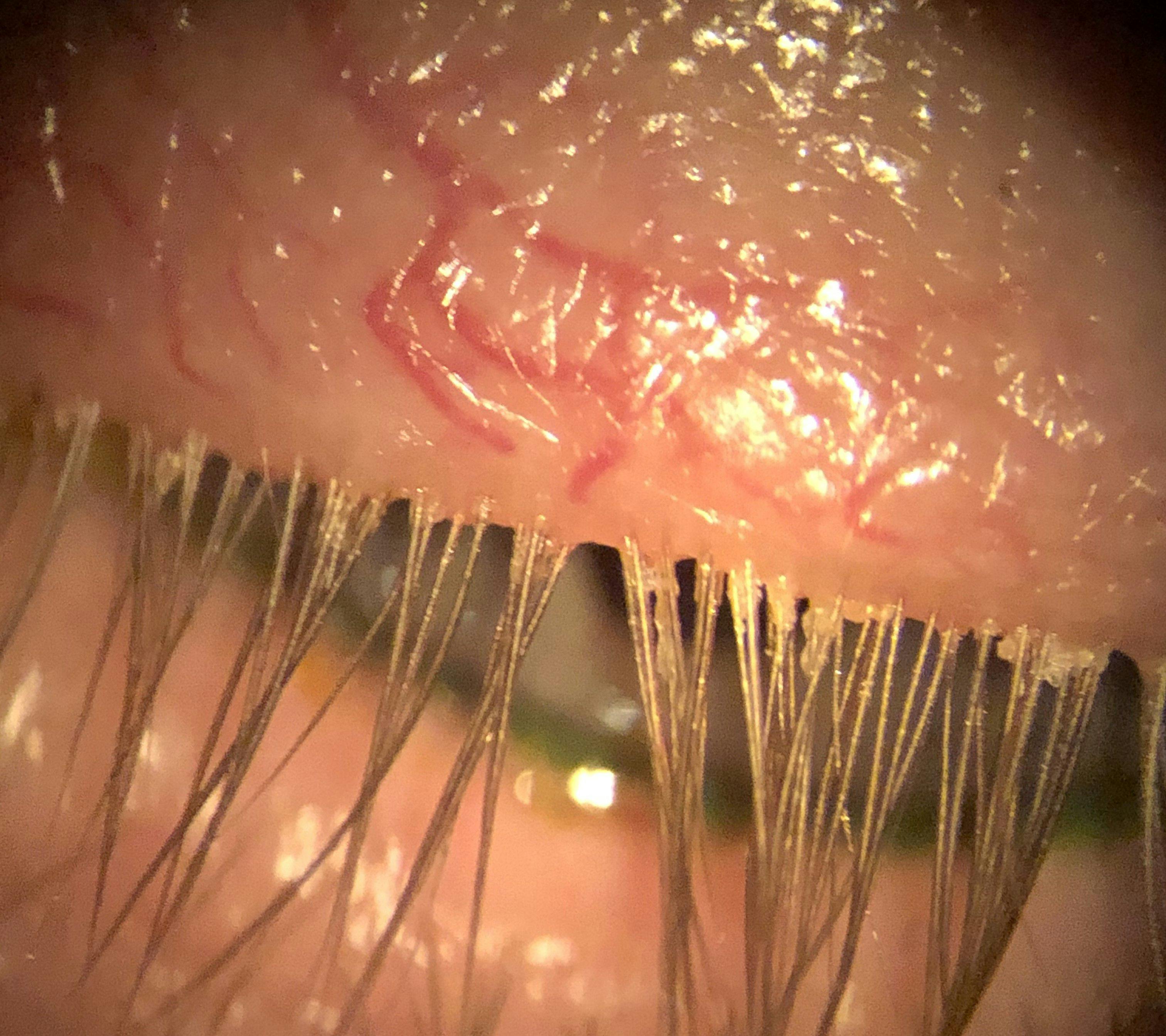
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO.
Transilluminator exam findings
Beyond a slit lamp evaluation, the use of a transilluminator to assess lid closure is a simple but incredibly valuable diagnostic test. To check for lagophthalmos, have the patient tilt their head back and gently close their eyes while shining the light of the transilluminator where the lids meet. If you see the white of the sclera, like in Figure 2, or a glint of light reflected back, this indicates incomplete lid closure.10,11
Additionally, the Korb-Blackie light test can be performed by dimming the lights, having the patient close their eyes, and then placing the transilluminator directly on the upper lid. If you see light shining through the interpalpebral area, this is evidence of a poor lid seal.12
Both of these findings can be significant contributors to DED, as they can lead to nocturnal exposure, discomfort upon waking, and recurrent corneal erosions (RCEs). These patients will often complain of nighttime and morning dryness while typically exhibiting inferior corneal staining in the exposed area.
Figure 2 features a patient with incomplete lid closure, as shown by an exam with a transilluminator.


Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO.
2. The meibomian glands
Meibomian gland structure and function can be easily evaluated through slit lamp examination and the use of a transilluminator. Gland capping or an inflamed appearance of the glands, like that present in Figure 3, can be indicative of MGD.
The quality of the meibum can be assessed by applying gentle, sustained pressure to the eyelid with either a finger or cotton-tipped applicator. If the glands produce a cloudy, turbid, or thick, toothpaste-like secretion, this may be suggestive of MGD, as meibum will ideally have a clear, olive oil-like consistency. If there is no secretion at all, this may indicate the non-producing gland has atrophied.13
A simplistic way to assess meibomian gland structure in more detail is to evert the eyelid and then transilluminate the lid by placing a transilluminator against the external portion of the lid. This will allow visualization of the entire gland structure and reveal any potential structural disruptions such as tortuosity or dropout.13-15
Figure 3 demonstrates a patient with inflamed meibomian glands, likely caused by MGD.

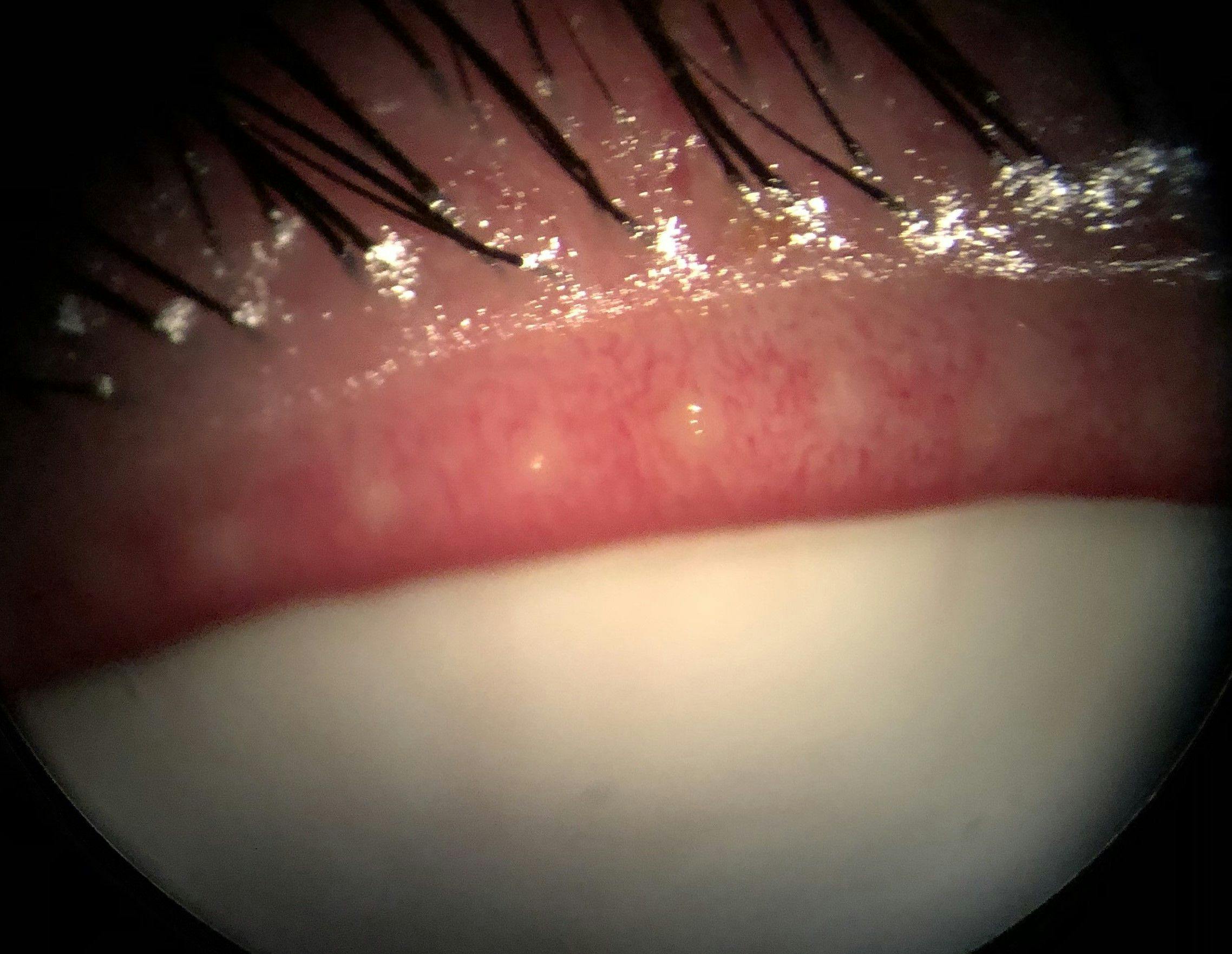
Figure 3: Courtesy of Cory Lappin, OD, MS, FAAO.
3. The tear film
The quality of the tear film provides vital information about the health of the ocular surface. Tear breakup time (TBUT) and tear meniscus height evaluation are both valuable and easily performed assessments that require only the use of sodium fluorescein dye and the cobalt blue filter of the slit lamp, as in Figure 4.
TBUT and tear meniscus height evaluation
A TBUT value of 10 seconds is generally considered normal, with any shorter time being suggestive of DED.16-17 While a reduced TBUT is traditionally associated with the premature tear film evaporation present in MGD and evaporative dry eye, it can also be reduced in aqueous deficient dry eye.18
Measuring tear meniscus height can provide vital information regarding tear production. The tear meniscus height is highly correlated with tear film volume, as the meniscus holds an estimated 70 to 90% of the total tear volume on the ocular surface.19-22
A height of ~0.3mm is considered normal, whereas a height of less than 0.2mm can be indicative of aqueous deficiency, and heights above 0.45 to 0.50mm are suggestive of possible overproduction of tears as a compensatory mechanism for dryness, which can lead to epiphora.23,24
Figure 4 shows a TBUT and tear meniscus height evaluation using a sodium fluorescein dye and cobalt blue filter at a slit lamp.

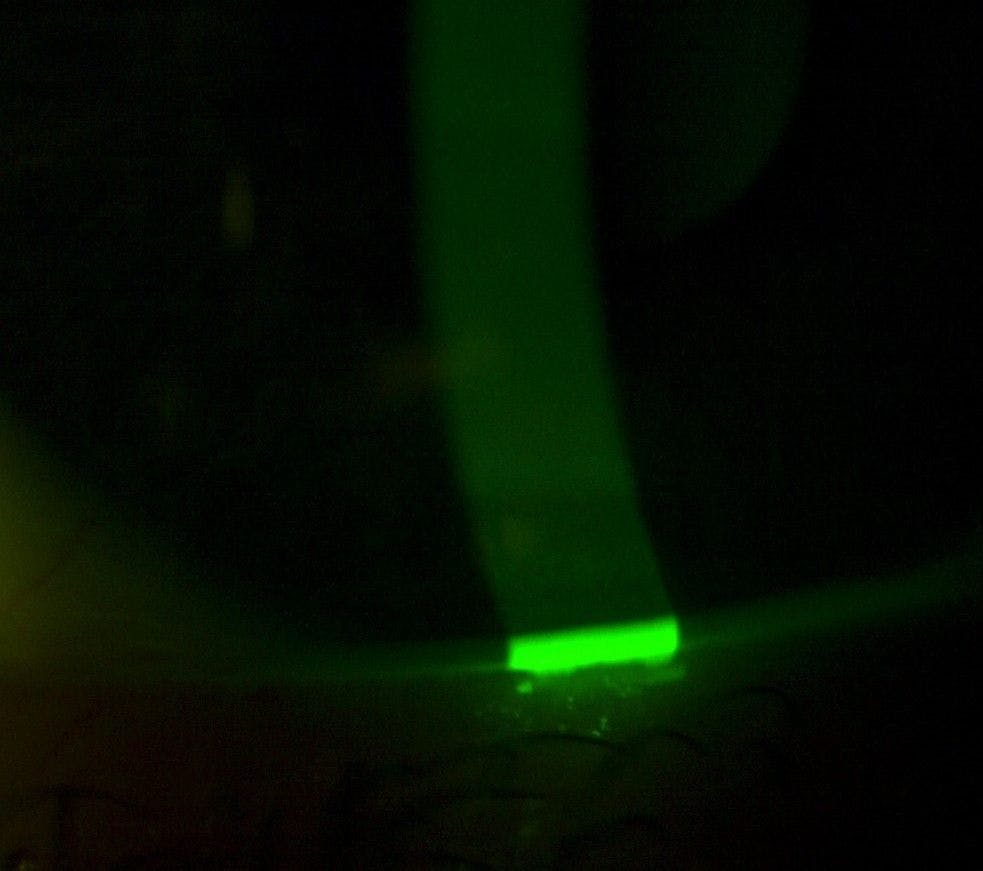
Figure 4: Courtesy of Cory Lappin, OD, MS, FAAO.
Schirmer strips
Though traditionally used to assess tear production, the use of Schirmer strips has inherent flaws that result in the test providing little real-world value in my clinical experience. When a test strip is inserted into the lower fornix, it stimulates reflex tearing, which is innately different from the basal tear production we are interested in when assessing dry eye.
If an anesthetic is instilled to prevent the stimulation of reflex tearing prior to strip insertion, the results are still altered due to the anesthetic blocking nerve sensation, which is vital to normal blinking and tear production. In fact, it has been shown that Schirmer testing, in general, has poor sensitivity, specificity, and reproducibility.19,21 Therefore, more noninvasive means of assessing tear production are recommended.
Slit lamp mirror reflection of the tear film
A lesser utilized but still helpful assessment of tear film quality can be performed by evaluating the quality of the reflection of the slit lamp mirror on the tear film. If the reflection appears crisp and clear, as shown in Figure 5, this indicates a healthy tear film, whereas a blurry or unstable reflection demonstrates tear film instability or poor quality. Likewise, the presence of debris or overly mucoid tears also signals tear film dysfunction associated with DED.
Figure 5 highlights a healthy tear film with a clear reflection from a slit lamp mirror reflection.


Figure 5: Courtesy of Cory Lappin, OD, MS, FAAO.
4. The cornea and conjunctiva
The health of the cornea and conjunctiva are readily evaluated using sodium fluorescein and lissamine green vital dyes as well as direct observation. Areas that stain with sodium fluorescein—which is ideal for assessing the cornea—represent damaged and/or devitalized cells as well as epithelial defects.23,25 Lissamine green provides greater contrast, which makes it a better choice for evaluating the conjunctiva, and stains dead and devitalized cells.25
Corneal findings
The staining pattern itself also provides valuable information. An inferior band of staining, as displayed in Figure 6, is commonly seen in cases of lagophthalmos, especially where there is nocturnal exposure, while interpalpebral staining can represent incomplete blinking.23 Diffuse corneal staining can be due to inflammation and is often associated with aqueous deficiency and inflammatory conditions like Sjögren’s syndrome.26
Staining of the lid wiper region, which is adjacent and posterior to the line of Marx and is responsible for spreading tears over the ocular surface with each blink, represents lid wiper epitheliopathy (LWE) and is thought to result from mechanical friction between the lid wiper and the ocular surface due to dryness.27 Therefore, the presence of staining with either dye can represent ocular surface stress, damage, and/or inflammation.28
Figure 6 features an inferior band of staining with sodium fluorescein dye, which is often associated with lagophthalmos.

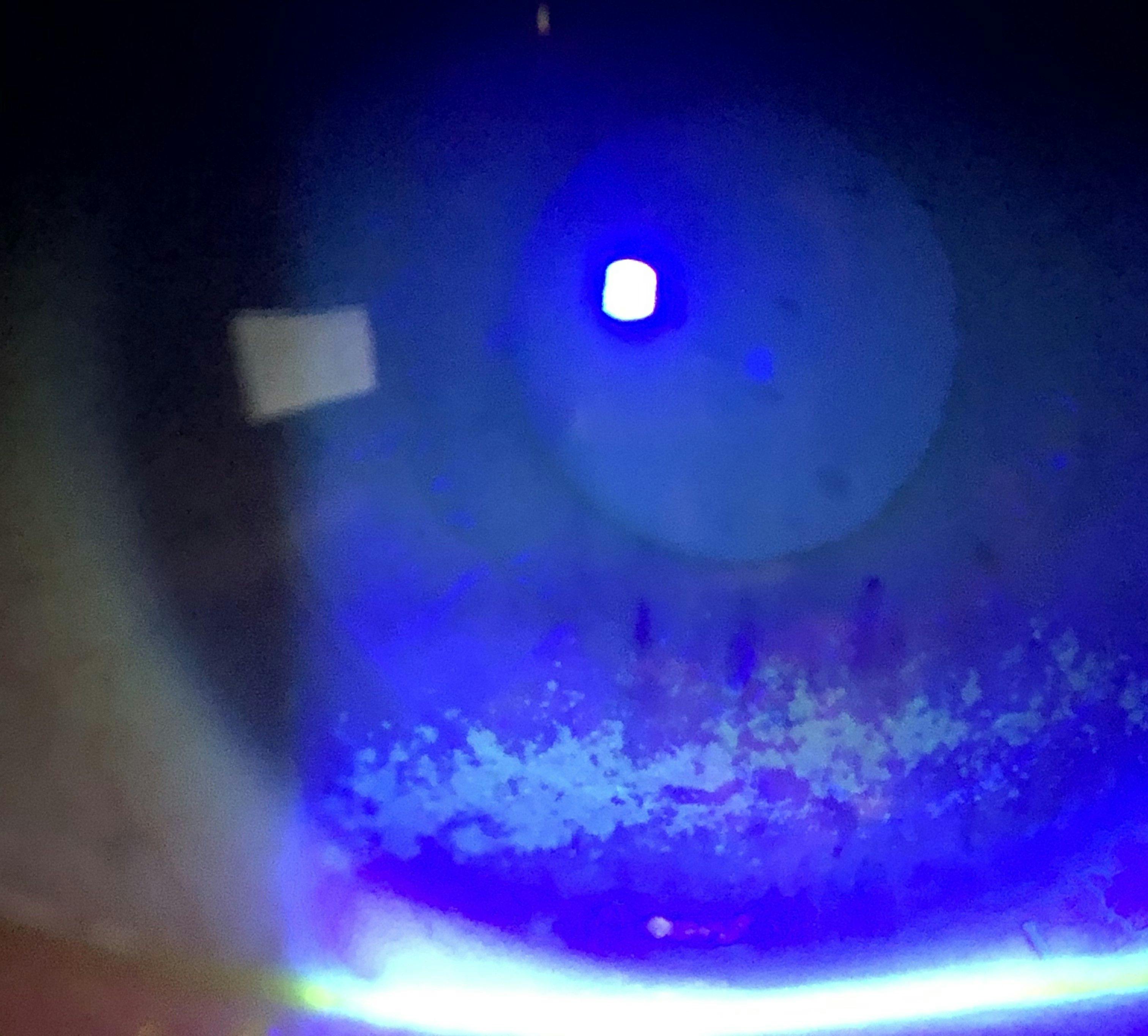
Figure 6: Courtesy of Cory Lappin, OD, MS, FAAO.
Conjunctival findings
Although conjunctival hyperemia is often dismissed as a purely cosmetic concern, significant conjunctival injection can also represent ocular surface stress and inflammation as the conjunctival vessels dilate in response to a myriad of insults such as excess dryness or mechanical irritation.29-32 Therefore, ocular redness can be penciled in as another key indicator of DED and OSD.
The palpebral conjunctiva provides findings that are helpful in diagnosing both dryness and allergies. The presence of papillae, as shown in Figure 7, alongside stringy or ropey discharge and complaints of itching are hallmark findings of ocular allergy.33-45 Large papillae can be suggestive of mechanical friction induced by ocular surface dryness, especially in contact lens wearers, which manifests as giant papillary conjunctivitis (GPC).46-48
Figure 7 demonstrates a patient with papillae, which is usually indicative of ocular allergies.

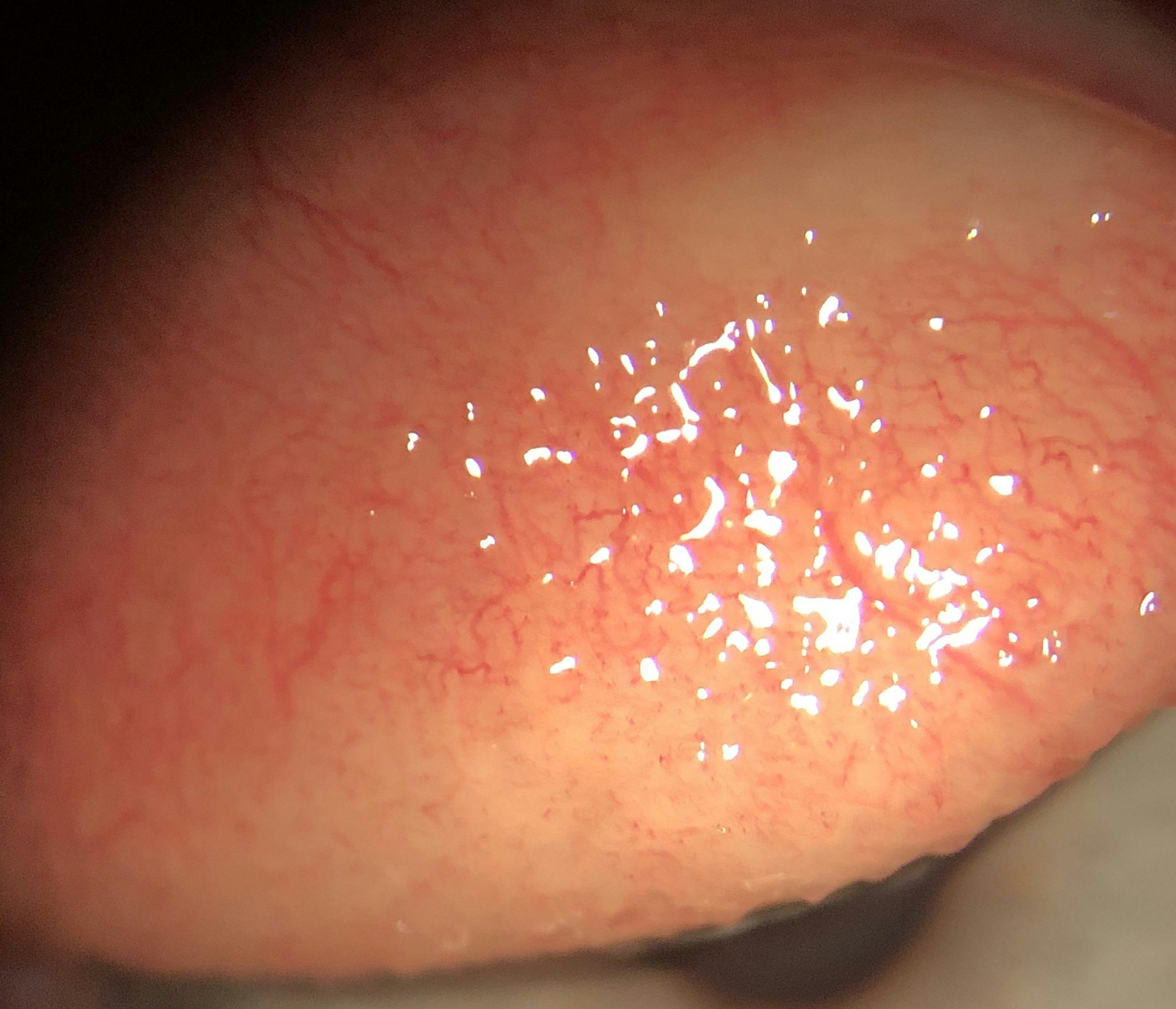
Figure 7: Courtesy of Cory Lappin, OD, MS, FAAO.
Corneal nerve findings
An often-overlooked component of the ocular surface is the corneal nerves. However, the health and function of the nerves can be tested by teasing and forming a wisp at the end of a cotton-tipped applicator.
The wisp can then be touched against the cornea in four quadrants and centrally to assess corneal sensation, as is demonstrated in Figure 8.49,50 If the patient displays reduced or absent sensitivity, this is indicative of nerve dysfunction and can represent neurotrophic keratitis (NK).51-53
While I recommend performing corneal sensitivity testing on all dry eye patients, it is especially important to perform on refractive surgery patients or patients with a history of herpetic infection as these are two common causes of NK.54,55 If you are unsure if a patient’s symptoms are due to direct ocular surface disruption or some other cause, the instillation of topical anesthetic can help aid in this differentiation.
Further, if the patient’s symptoms improve upon anesthetic instillation, this likely means the source of their discomfort is direct ocular surface disruption, whereas if the symptoms persist, this suggests the pain may stem from a different source, such as centralized neuropathic pain.56
Figure 8 shows a patient undergoing a corneal sensitivity examination with a cotton-tipped applicator.


Figure 8: Courtesy of Cory Lappin, OD, MS, FAAO.
Creating a foundational dry eye treatment regimen
Just as I recommend taking a systematic approach to evaluating the ocular surface, I likewise recommend creating a treatment plan that addresses DED and OSD in the same manner. We all know DED is multifactorial as it can stem from dysfunction of any component of the ocular surface, as each of its constitutive elements needs to work in concert to maintain homeostasis.57,58
Therefore, each contributing element of DED must be addressed to treat an individual patient’s DED completely. And, again, getting a patient started on a foundational DED treatment does not require any advanced treatment devices, just a targeted plan that addresses each element of their DED.
Treating the lids and lashes
Lid hygiene is a vital element of any foundational dry eye treatment regimen. Hypochlorous acid-based cleansers, such as HyClear (hypochlorous acid 0.01%, Contamac), Optase Protect (hypochlorous acid 0.015%, SCOPE), and NeutraWipes (hypochlorous acid 0.0125%, TearRestore), are excellent choices for controlling bacterial blepharitis.59
Tea tree oil (TTO), like Advanced Formula 2% Tea Tree Eyelid & Facial Cleanser (EyeEco), OPTASE TTO Eyelid Cleansing Gel (SCOPE), and Cliradex Light Foam (Cliradex), as well as okra-based cleansers like ZocuFoam Eyelid Cleanser and Moisturizer and ZocuWipes (Zocular) can also be utilized as they help reduce the number of Demodex mites present on the lids and lashes.60-65
Although TTO can be helpful in reducing Demodex populations, it is a relatively harsh treatment that can induce an increased amount of symptomatology, including irritation for some patients.66 However, for cases of Demodex blepharitis (DB), we now have the first and currently only FDA-approved medication specifically indicated for the treatment of DB with Xdemvy (lotilaner ophthalmic solution 0.25%, Tarsus Pharmaceuticals), which can successfully reduce mite population, collarette number, and redness.67-69
Blink exercises can promote proper blinking mechanics and reduce the number of incomplete blinks.70 Nocturnal gels and ointments, including Siccasan gel (AGEPHA Pharma) and HYLO Night ointment (SCOPE), can aid in protecting the ocular surface from drying out in cases of nocturnal exposure as well as employing sleep goggles, such as Eyeseals 4.0 (EyeEco), or adhesive eye patches, like SleepTite/SleepRite (Ophthalmic Resources Partners).
Treating the meibomian glands
Omega-3 fatty acid supplementation is a staple of dry eye treatment as it has been shown to improve the signs and symptoms of DED and MGD.71-73 In fact, one study found that 70% of dry eye patients became asymptomatic using only an omega-3 supplement and artificial tears.74
However, to get the maximum benefit of omega-3, it is recommended to use a supplement that includes a high quality, re-esterified, triglyceride-based omega-3 supplement with a 3:1 eicosapentaenoic acid (EPA) to docosahexaenoic acid (DHA) ratio and at least 2 grams of combined EPA and DHA, such as DE3 Omega Benefits (PRN Vision Group).71-73
Warm compresses can provide increased comfort by aiding in the melting of stagnant meibum in MGD.75,76 However, the use of a dedicated dry eye compress such as a Dry Eye Relief Mask (EyeEco), Bruder Moist Heat Eye Compress (Bruder Health), Open-Eye Thermal Mask (TearRestore), or Electric Heated Dry Eye Mask (Wizard Research), is recommended over the use of at-home compresses, such as washcloths, as they may retain a higher level of heat for a longer duration of time.76
The use of oral agents such as doxycycline and azithromycin can also be helpful in managing DED and OSD, as they have anti-inflammatory properties that are retained at even low doses and have been shown to be beneficial in the management of MGD and ocular rosacea.77-81 Additionally, topical azithromycin in the form of AzaSite (azithromycin ophthalmic solution 1%, Théa) has also been shown to be beneficial in the treatment of MGD.82-84
However, the use of doxycycline should be avoided in pregnant and nursing patients as well as children 12 years old and younger due to the side effect profile.77-80
Treating the tear film
While addressing the underlying causes of tear film instability, such as MGD, will intrinsically improve tear film quality, there are also treatments available to help bolster these effects. Artificial tears are the most commonly used treatment for DED; their impact is primarily palliative but still can provide quick symptom relief when needed.85-88
When choosing an artificial tear, it is recommended that a preservative-free (PF) formulation be used. A PF lipid-based artificial tear can be useful in cases of MGD, and a non-lipid PF artificial tear can be beneficial for use with contact lenses.
In terms of prescription treatments, MIEBO (100% perfluorohexyloctane ophthalmic solution, Bausch + Lomb) essentially acts as a tear film stabilizer as it mimics the function of natural meibum by forming a protective monolayer over the lipid layer, which reduces premature evaporation, making it a viable option for MGD treatment.89-91
Tyrvaya (varenicline solution nasal spray 0.03mg, Viatris) is a neurostimulatory agent that increases natural tear production via nasal stimulation of the trigeminal parasympathetic pathway, which can be particularly helpful in cases of aqueous deficient dry eye.92,93
Treating the cornea and conjunctiva
Ocular surface staining and injection are often signs of inflammation and, therefore, may require the use of anti-inflammatory agents. Although topical corticosteroids are the most effective anti-inflammatory treatment, they are not fit for long-term use due to potential side effects, including premature cataract formation, increased intraocular pressure, and glaucoma development.94-100
Topical treatments for DED and OSD
Therefore, an LFA-1 antagonist such as Xiidra (lifitegrast 5% ophthalmic solution, Bausch + Lomb) and immunomodulators including Cequa (cyclosporine 0.09% ophthalmic solution, Sun Pharmaceuticals), Vevye (cyclosporine 0.1% ophthalmic solution, Harrow), and Restasis (cyclosporine 0.05% ophthalmic emulsion, Allergan, An AbbVie Company), are more appropriate long-term treatment options as they tend to reduce inflammation without carrying the side effect profile associated with prolonged steroid use.
This does not mean, however, that topical steroids do not have a place in DED management. Topical steroids, like Eysuvis (loteprednol etabonate ophthalmic suspension 0.25%, Alcon), are well-suited for the short-term management of dry eye flares and, under proper ECP supervision, can be used sparingly as a “rescue” drop, similar to a rescue inhaler, to provide rapid relief when patients are experiencing a “bad eye day.”101
Biologic treatments such as autologous serum (AS) tears and platelet-rich plasma (PRP) drops can also be beneficial in treating DED, especially where there is significant inflammation and corneal surface disruption, as both have anti-inflammatory properties and encourage ocular surface healing.102-110
Targeting conjunctival hyperemia
If a patient is experiencing significant conjunctival hyperemia, the goal would be to address the underlying cause. However, patients often desire a drop that can provide quick cosmetic redness relief when needed, such as for special events or social outings.
In such cases, Lumify (brimonidine tartrate ophthalmic solution 0.025%, Bausch + Lomb) can be recommended as the rebound effect observed with the use of other redness relievers is less common with Lumify.111-113
Managing ocular allergies
For patients displaying signs of ocular allergy, which is a common comorbidity of DED, topical antihistamine/mast cell stabilizer combination drops, such as Pataday Once Daily Relief Extra Strength (olopatadine hydrochloride ophthalmic solution 0.7%, Alcon), Lastacaft (alcaftadine ophthalmic solution 0.25%, Allergan, An AbbVie Company), and Alaway Preservative Free (ketotifen fumarate ophthalmic solution 0.035%, Bausch + Lomb) are suitable treatment options.
These drops quickly relieve itching and inflammation by inhibiting the action of histamine and preventing further degranulation of histamine by blocking the binding of allergens to mast cells.33,39,40,114,115
Additionally, Optase Allegro (SCOPE) is another effective treatment option for ocular allergies. This product is composed of both a lubricating agent in the form of hydroxyethyl cellulose and an anti-allergy agent in the form of ectoin, which functions through the mechanism of preferential exclusion whereby water molecules are drawn close together by the ectoin forming a “water shield” that blocks allergens from reaching the ocular surface.116-118
Time to get started
While all the advancements in DED and OSD diagnostics and therapeutics have improved our ability to treat these conditions, managing DED does not require having a fully equipped dry eye center of excellence to get started.
A thorough patient history, careful slit lamp exam, and the use of other readily available tools such as vital dyes, a transilluminator, and cotton-tipped applicators are all that are needed to get started diagnosing and treating DED.
A patient’s answers to a few specific questions about their symptoms plus one or two clinical signs will allow you to diagnose the majority of DED and OSD effectively you will encounter in the course of routine patient care.
Conclusion
Once the diagnosis has been made, the majority of patients can potentially improve by leveraging basic, foundational treatments such as omega-3 supplementation, lid hygiene, blink exercises, warm compresses, and artificial tears, along with an immunomodulator, tear film stabilizer, steroid or neurostimulatory agents, when medically necessary.
Therefore, if you have been wanting to dive in and treat dry eye and ocular surface disease but feel like you lack the appropriate diagnostic equipment or treatment devices to do so, in actuality, you likely already have everything you need, so now is the time to get started!
