“
Optimizing the ocular surface” is a commonly used phrase in eyecare, but what does this actually mean? Essentially, it means an effort to encourage or restore homeostasis.
Homeostasis is a self-regulating process by which biological systems maintain physiological stability, regardless of outside environmental factors—meaning the body will keep physiological variables within a set range to maintain proper function.
Homeostasis and the ocular surface
Therefore, these biological systems exist in a state of dynamic equilibrium, where variables constantly adjust in response to the environment to remain in this optimal range. Because this process is feedback dependent, it relies on biological “sensors” to collect data which can be integrated with feedback from other systems to determine the appropriate response.
However, homeostasis is lost if the body cannot maintain physiological values within the preset range, and disease or even death can occur. As such, there must be a balance between internal and external environmental challenges and a biological system’s response; the ocular surface is no exception.
When faced with a challenge to homeostasis, such as an arid climate, the ocular surface must respond to maintain proper function. But if it is unable to do so, disease, such as dry eye, can occur.
What makes up the ocular surface?
The ocular surface is an excellent example of a homeostatic system, as it is more than just the cornea and conjunctiva, but also the tear film (and its constituent components), the eyelids and lashes, meibomian glands, lacrimal glands, and goblet cells as well.
These elements must work together for the greater system to function properly. The ocular surface is further integrated into an even larger system, including higher-order processing at the level of the brain.
Foreign bodies on the ocular surface
An example of homeostasis in action occurs when a foreign body gets in the eye. When a
foreign body touches the cornea, it threatens to disrupt homeostatic balance (i.e., it can damage the surface epithelium, which impairs proper function), so the corneal nerves sense its presence.
This nerve signal is then relayed to the brain, which in turn sends a signal to the lacrimal gland and orbicularis oculi muscle to stimulate reflex tearing and blinking, respectively, in an attempt to expel the foreign body and restore homeostasis.
This illustrates the importance of the ocular surface’s ability to sense and adapt to external challenges in a self-regulated fashion. In this example, the body responds to the foreign body without conscious effort, allowing the system to remain functional.
Dry eye disease
Dry eye disease (DED) is likely the most common disruptor of the ocular surface. However, to properly understand dry eye and, more importantly, how to treat it, one must first understand how the ocular surface and its constitutive elements function in health and disease. The proper functioning of the ocular surface as a system must be viewed through a homeostatic lens.
“If one does not understand this self-regulating process [homeostasis], then it is not possible to comprehend fully the function of the body in health and in disease.” - George Billman, PhD
Consequently,
dry eye treatment must also be considered from a homeostatic perspective. DED is caused by a loss of homeostasis of the tear film, resulting in inflammation and damage. However, dry eye is multifactorial in nature, with the cornea, conjunctiva, tear film, meibomian glands, lacrimal glands, and the eyelids and lashes all potentially being affected, so the entire ocular surface must be treated to address the condition properly, not just a single element.
Therefore, determining which component(s) is/are the cause of the breakdown of homeostasis will determine what treatment is necessary to restore it.
Addressing the root cause of ocular surface dysfunction
Additionally, a key element of treating dry eye from a homeostatic perspective involves treating the root cause of the dysfunction. For example, while inflammation can occur in
meibomian gland dysfunction (MGD)-associated dry eye (“evaporative dry eye”), this inflammation is often a result or symptom of the condition stemming from a premature evaporation of the tear film rather than inflammation being the root cause of the MGD.
So, while using steroids as treatment in such a case may quell the inflammation caused by this premature breakup of the tear film, their use does not fundamentally restore homeostasis at a base level, as it does not address the underlying cause. When treating from a homeostatic perspective, the goal of treatment should be to address the underlying cause instead of just masking symptoms.
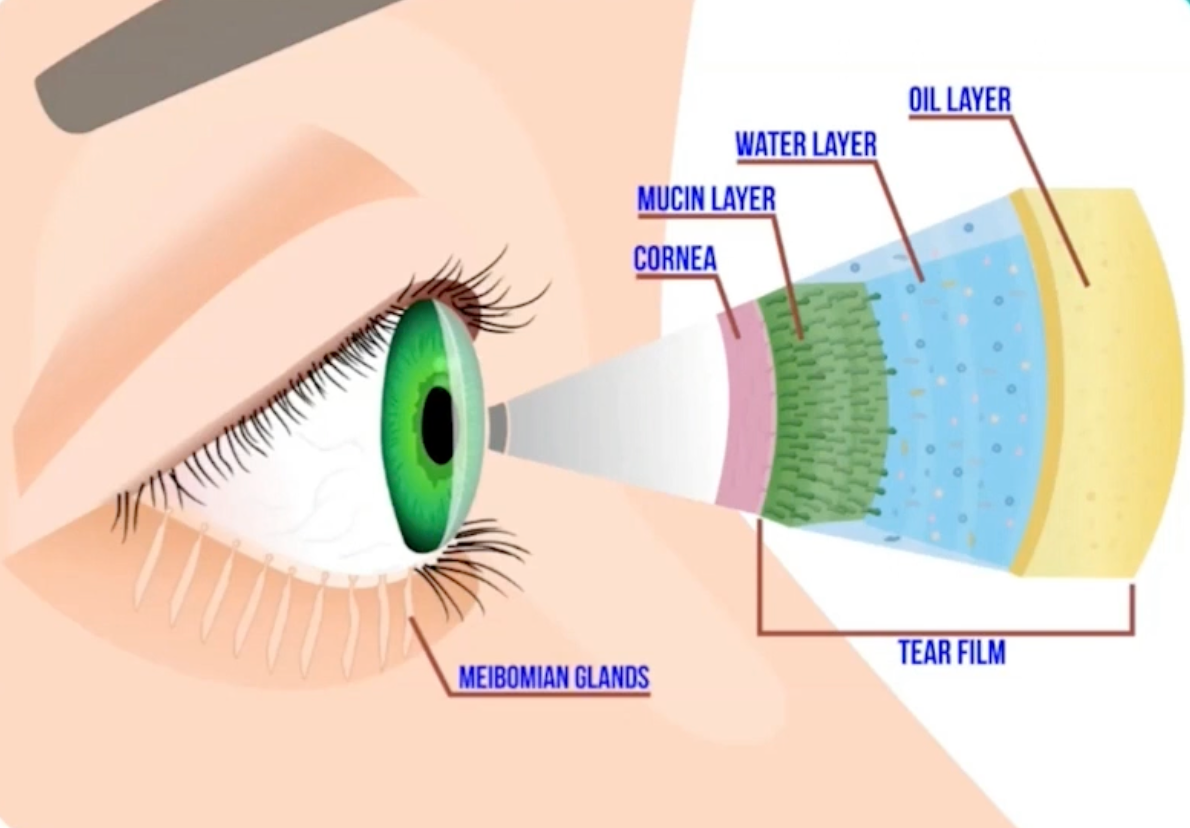
Figure 1 highlights the ocular surface system, with the layers of the tear film layer, including the mucin, water, and oil layers, as well as the cornea and meibomian glands.
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO
Dissecting the ocular surface: the tear film and corneal nerves
The tear film comprises three main components, which, although heterogeneous in actuality, can be simplified into the mucin layer, the aqueous layer, and the lipid layer. The mucin layer is the foundation of the tear film, produced primarily by goblet cells and secondarily by the lacrimal glands, and it anchors the mainly water-based tear film onto the hydrophobic cornea.
The aqueous layer, produced by the lacrimal glands and accessory lacrimal glands, is made up of 98% water and hydrates, nourishes, and
protects the cornea. The lipid layer, which is produced by the meibomian glands, comprises over 600 different lipid species, which all work together to act as the “roof” of the tear film, preventing evaporation, providing a smooth ocular surface, and reducing surface tension.
Corneal nerves and ocular surface disease
As previously mentioned, homeostasis relies on feedback, so functioning corneal nerves are vital to achieving and maintaining a healthy ocular surface. The cornea is the most densely innervated structure in the body, providing feedback (including sensation). This feedback allows for proper routine epithelial cell turnover, wound healing, blinking, and lacrimation.
One of the most well-known examples of corneal nerve involvement in dry eye is reflex tearing in
meibomian gland dysfunction. If the tear film evaporates too quickly, as is often the case in meibomian gland dysfunction, this leads to corneal irritation, to which the corneal nerves respond by sending a signal to the brain. This, in turn, results in increased aqueous production by the lacrimal gland, often resulting in epiphora.
This is why patients may believe they do not have dry eye because their eyes constantly water when in reality, this is a compensatory homeostatic response to evaporative dry eye.
Dry eye: a modern ocular surface disease?
The ocular surface and our visual system developed over millions of years to aid a lifestyle emphasizing distance vision owing to our hunter-gatherer ancestors who relied on distance vision to spot predators and prey. However, over the span of several hundred years, the emphasis of our visual focus has switched primarily to near activities.
Modern technologies have imposed an extreme emphasis on our near vision, forcing the ocular surface to function in a manner far different from the circumstance under which it developed, so the system must constantly battle to maintain balance. The rapid rise in our reliance on near vision, partly due to increased literacy and
computer and phone use, contributes to this challenge, as a mismatch exists between our modern environment and evolutionary history.
Such changes, driven by ever-increasing screen time, have fundamentally altered how we use our eyes, including our blinking behavior, which can have a negative impact on proper ocular surface function.
A result of these changes is that DED, a condition once associated almost exclusively with older females, has now spread to every demographic.
Inflammation and ocular surface disease
When homeostasis breaks down, and the body fails to maintain balance, inflammation is the body’s last attempt at protecting itself. However, the negative side effects of inflammation often outweigh the benefits.
There are two main types of inflammation, primary and secondary:
- Primary inflammation: Occurs when inflammation is the root cause of the disease, such as in Sjögren's syndrome and other inflammatory diseases.
- Secondary inflammation: Occurs as the result of a disruption of homeostasis, such as meibomian gland dysfunction.
Knowing if the inflammation present is primary or secondary determines how it is treated because, as previously discussed, if an anti-inflammatory, such as a topical steroid, is used to treat secondary inflammation, it is essentially just masking a symptom of a problem rather than addressing the root cause.
Causes of disruption to the ocular surface
Meibomian gland dysfunction is one of the
leading causes of dry eye. The meibomian glands and lipid layer have been particularly affected by the relatively recent changes in our modern lifestyle, mainly increased screen time and altered diet, as the function of the meibomian glands is intrinsically tied to these two factors.
The impact of diet on ocular surface disease
A modern diet, which is often lacking in
omega-3 fatty acids, can alter meibum composition, resulting in thickened oils with an increased melting point, which can impair secretion. Additionally, when a person looks off into the distance, they blink 16 to 18 times per minute, but when focused on a near target, that number can drop to four or less.
The issue with this change is twofold: first, the ocular surface can begin to physically dry out as the tear film is not continually replenished over the surface, and second, our blinking mechanics are fundamentally altered.
Blinking and ocular surface dysfunction
When we blink, it is thought that the orbicularis oculi muscle pressurizes the glands. When the lids completely touch the muscles of Riolan, which encircle and close off the orifices of each meibomian gland, they relax, allowing meibum to be secreted.
However, when focusing on near tasks, there is an increase in
partial or incomplete blinks. In these cases of incomplete blinking, the lids never fully touch. Therefore, the muscles of Riolan never relax, so the meibomian glands remain sealed, and the meibum contained within the glands is never secreted.
Meibum will continue to be produced, even if the meibum already present has not been secreted, leading to clogging and distension of the glands, which can damage gland structure, causing MGD. The end result of these disruptions is the unstable tear film, ocular irritation, and blurred vision commonly associated with MGD.
To treat MGD, dietary issues can be addressed with omega-3 supplements, blink exercises that can encourage proper blinking mechanics, and warm compresses that can help comfort the eye.
Additionally, procedures such as LipiFlow, iLux, and TearCare can treat clogged glands, and intense pulsed light (IPL) can promote healthy meibomian gland structure and function.
Aqueous deficiency and ocular surface disease
Aqueous deficiency is far less common than MGD. However, in cases of inflammatory disease, such as Sjögren's syndrome, the lacrimal glands can become damaged, resulting in disrupted aqueous production.
In these cases, anti-inflammatories are often necessary to restore a healthy aqueous layer, as inflammation is the driving force behind the dysfunction.
Immunomodulators such as Xiidra, Cequa, and Restasis all aid in accomplishing this, while neurostimulators like Tyrvaya and the iTear100 device can encourage tear production.
Corneal nerve dysfunction and ocular surface disease
Corneal nerve dysfunction is an often overlooked cause of ocular surface disease. However, corneal nerve dysfunction, such as
neurotrophic keratitis, can significantly impact homeostasis, as the nerves are responsible for controlling routine epithelial cell turnover, wound healing, blinking and tearing, and providing sensation. Nerve damage can be caused by herpetic infection, refractive surgery such as LASIK, injury, chronic preservative exposure from glaucoma medications, or systemic diseases such as diabetes or stroke.
While traditional treatments for neurotrophic keratitis include amniotic membranes, neurostimulators, and surgical interventions (such as tarsorrhaphy), there have been major advancements in treating nerve dysfunction, including the development of Oxervate.
Oxervate (cenegermin-bkbj) is a recombinant form of human nerve growth factor (rhNGF) that directly repairs damaged nerves, addressing the root cause of neurotrophic keratitis.
Ocular rosacea and ocular surface disease
Ocular rosacea is another often overlooked cause of ocular surface dysfunction. In health, an antimicrobial peptide called cathelicidin is produced in response to potential pathogens as part of our innate immune response. However, in all forms of rosacea, including ocular rosacea, there is a hypersensitization of this immune response, which can be triggered by normal environmental and physiologic stimuli such as cold weather, spicy food, stress, and other factors.
This results in an overproduction of cathelicidin, leading to an increase in vascular endothelial growth factor (VEGF) expression, resulting in the development of telangiectatic vessels on the ocular surface that causes the redness and inflammation classically associated with rosacea. While there is currently no cure for ocular rosacea, the inflammation associated with the condition can be managed with oral tetracyclines, such as doxycycline, low-dose steroids, and immunomodulators.
Additionally, eye drops such as Lumify can constrict the abnormal vessels, providing cosmetic redness relief. The closest treatment to addressing the root cause of ocular rosacea is IPL, which can destroy the telangiectatic vessels, reducing the associated inflammation and making it one of the best treatment options for the condition.
Mechanical eyelid issues and ocular surface disease
Mechanical eyelid issues are another cause of ocular surface disease. Proper blinking and eyelid closure allow the tear film to be replenished and spread over the ocular surface in a healthy eye. Complete lid closure also offers protection and allows the ocular surface to recover during sleep. However, incomplete lid closure can result in nocturnal exposure that causes significant ocular surface damage.
Classic signs of incomplete lid closure are dryness that is worse in the morning, and inferior superficial punctate keratopathy (SPK), indicating the lids are not closing fully. Although incomplete lid closure is often associated with conditions like
Bell’s palsy, it is also common among older patients, as a natural decrease in lid elasticity occurs with age.
In these cases, there may not be an obvious issue with lid closure, however, there may exist what is referred to as a poor lid seal, where the upper lid merely rests on the lower lid rather than forming a tight seal. The signs and symptoms of a poor lid seal are often the same as traditional lagophthalmos. Because surgery could possibly worsen symptoms, it should be approached with caution.
Safe, reliable treatments of incomplete lid closure include nocturnal lubrication, sleep goggles, and barrier lenses like bandage or scleral contact lenses (for daytime use). IPL may also help improve blink mechanics by reducing lid laxity through increased collagen synthesis.
Demodex mites and ocular surface disease
While bacteria and Demodex mites are part of our skin’s natural microflora, an overpopulation of these microbes can disrupt the ocular surface, usually in the form of
blepharitis. Overpopulation of Demodex will result in a buildup of proinflammatory sleeve-like collarettes on the bases of the lashes and a blockage of the meibomian glands, as the two species of Demodex mites found on human skin, D. folliculorum and D. brevis, inhibit the lash follicles and meibomian glands, respectively.
Bacterial overgrowth will cause inflammation of the ocular surface and present with frothy or foaming-appearing tears (saponification), lid notching, and loss of lashes due to the production of proinflammatory enzymes and lipases. Proper lid hygiene will reduce the presence of bacteria and Demodex, as using hypochlorous acid, tea tree oil, and okra-based cleansers are all ways to regain control of the microbial balance, reduce bacteria, and manage Demodex.
Additionally, a new treatment option for Demodex is on the horizon, as lotilaner ophthalmic solution has shown promising results in treating Demodex blepharitis and could become the first FDA-approved treatment for the condition.
Besides traditional lid hygiene products, microblepharoexfoliation of the lid margin can also be helpful with devices such as NuLids PRO and BlephEx, which can remove debris and biofilm associated with bacteria and Demodex.
Allergies/sensitivities and ocular surface disease
Lastly, allergies and hypersensitivities such as atopic keratoconjunctivitis (AKC) and
vernal keratoconjunctivitis (VKC) can also disrupt ocular surface health. Similar to ocular rosacea, allergies result from an exaggerated response to normal stimuli, such as pollen. The allergic response results in itching, swelling, mucus formation, and inflammation that disrupts and damages the ocular surface.
One of the best ways to restore balance in these cases is to block the response at its source with antihistamine-mast cell stabilizer combos or, in the case of acute exacerbation, steroids.
The newly FDA-approved drop Verkazia can be used for long-term inflammation management in cases of VKC.
Environmental challenges to homeostasis
While bacteria, mites, and overactive immune responses may be obvious causes of ocular surface damage, environmental challenges cannot be ignored. Homeostasis is naturally more challenging to maintain in some climates than others. Hot, dry climates stress the ocular surface, and patients often report improvement in their dry eye symptoms when visiting more mild environments.
"Beyond outdoor stressors, air conditioning, ceiling fans, and furnaces create a challenging indoor environment."
In these cases, taking steps to help account for these challenging climates, such as adding a humidifier or using spectacles with seals, can go a long way toward improving the ocular surface by creating a more hospitable environment or protecting the eye from external stressors.
Having the patient move to a less challenging climate is often not feasible, nor is this suggestion advisable, but rather helping the patient manage the unique challenges of their particular physical environment is the more appropriate response. Additionally, simply using
traditional dry eye treatments can also help make the tear film more resilient, which can improve the ocular surface’s ability to maintain homeostasis in more challenging climates.
Ocular surface homeostasis and contact lenses
By their very nature, contact lenses disrupt homeostasis, as contact lens wear introduces a foreign body onto the ocular surface. It has even been suggested that contact lens wear is inherently pro-inflammatory for this reason.
Therefore, when using contact lenses, the goal should be to minimize disruption to the ocular surface by using daily disposable lenses and lens materials more compatible with the ocular surface.
Out with the old: punctal plugs
One treatment that has thus far been absent from the discussion of
treating dry eye from a homeostatic perspective is the use of punctal plugs, and for good reason.
Punctal plugs are fundamentally counter to homeostasis, and their use is primarily based on an antiquated understanding of dry eye that suggests that dry eye is primarily caused by a lack of tear production, which is now known to be largely untrue, and an oversimplification of the disease.
In the vast majority of cases of dry eye, patients are producing an adequate tear volume. The true issue lies in the quality of the tears produced (for example, the poor quality of meibum produced in MGD) rather than the quantity.
Even in cases where tear production may be reduced, such as aqueous deficiency, this deficiency is usually due to an inflammatory condition and it has been shown that patients with dry eye have an increased level of inflammatory factors present in their tear film.
Digging deeper into punctal plugs
Therefore, using punctal plugs can potentially exacerbate inflammation by forcing poor-quality tears to sit on the ocular surface for a longer period, creating a “cesspool” effect. Additionally, punctal plugs do not treat the underlying cause of dry eye, as they essentially act as an extended-duration artificial tear, which is more palliative than therapeutic.
"Many patients who initially find relief from plugs will often find that this relief diminishes with time as the body adjusts to its new homeostatic set-point."
However, this is not to say there are no cases in which punctal plugs may be beneficial. In such cases, it is recommended that dissolvable collagen plugs be used first to assess their efficacy prior to the placement of semi-permanent plugs.
Due to the same rationale discussed above, punctal cauterization should be completely avoided as this procedure is irreversible without additional surgical intervention, which can lead to even further disruption of the delicate homeostatic system of the ocular surface.
Artificial tears and the ocular surface
The use of
artificial tears merits a discussion as well; artificial tears are a mainstay for the vast majority of dry eye treatment regimens, and they do indeed serve a purpose. Artificial tears provide a quick source of relief when irritation strikes. However, the comfort they provide is often fleeting.
The reason for this is that artificial tears are essentially a band-aid—they mask symptoms of dryness, but they do not treat the root cause. For this reason, artificial tears are more of a palliative treatment than a true homeostatic therapy. So, while artificial tears can be helpful and often should be included in a patient’s dry eye treatment regimen, the mistake of over-relying on artificial tears to manage the condition should be avoided.
In with the new: regenerative medicine
The primary goal of treating dry eye from a homeostatic perspective is to address, as closely as possible, the root cause of the disruption to help restore proper ocular surface function.
Regenerative therapies for ocular surface dysfunction:
- Intense pulsed light therapy: IPL is unique in the fact that it addresses several contributing factors to dry eye in a single treatment modality. Through the process of photobiomodulation, IPL is capable of repairing and encouraging the regeneration of damaged tissue.
- This is one of the proposed mechanisms by which IPL improves meibomian gland structure and function.
- Additionally, IPL can destroy the proinflammatory telangiectatic vessels associated with ocular rosacea, which is the closest we can currently get to treating the root cause of the condition.
- Amniotic membranes: Contain anti-inflammatory and growth factors that promote healing and tissue regeneration, especially cryopreserved membranes, such as Prokera.
- Oxervate: A recombinant form of human nerve growth factor (rhNGF) that directly repairs damaged nerves and enhances corneal wound healing.
These mechanisms make such regenerative therapies excellent homeostatic treatment options as they have the ability to restore function at a fundamental level.
Summary
To optimize the ocular surface, understanding the concept of homeostasis is crucial. First, one must understand how the system is intended to function in health and then determine what can cause the system to lose balance and, ultimately, what needs to be done to
restore this balance.
Therefore, homeostasis can be restored by treating the underlying cause, not just the symptoms, of dry eye and ocular surface disease, and the ocular surface will be successfully optimized.