While dry eye has traditionally been divided into the categories of aqueous deficient and evaporative, in many ways, this is an oversimplification. Thanks to advancements in our
understanding of dry eye disease (DED), we are well aware it is a multifactorial condition.
1So, in reality, most cases of dry eye do not neatly fit into the buckets of aqueous deficient or evaporative but rather exist on a spectrum that comprises many different ocular surface disorders. These other conditions, such as
blepharitis and
ocular rosacea, also contribute to dry eye by feeding into and often exacerbating one another.
However, there is significant clinical relevance to delineating the contributing factors to an individual patient’s dry eye. This value lies not solely in assigning a label to the type of dry eye but rather in teasing apart the specific elements of the patient’s condition.
Contributing conditions in dry eye
In the majority of cases, a patient will have
several conditions contributing to their dry eye at once, and each one must be addressed to treat the disease completely. However, because dry eye exists on a spectrum and the signs and symptoms of the contributory conditions are often nonspecific and inevitably overlap, it can be somewhat challenging to determine which factors are in play.
For this reason, I attempt to simplify this process by assigning each of the most common contributing factors to DED a single unique sign or symptom that sets it aside from the myriad of other ocular surface diseases which allows for easy identification, diagnosis, and subsequent treatment.
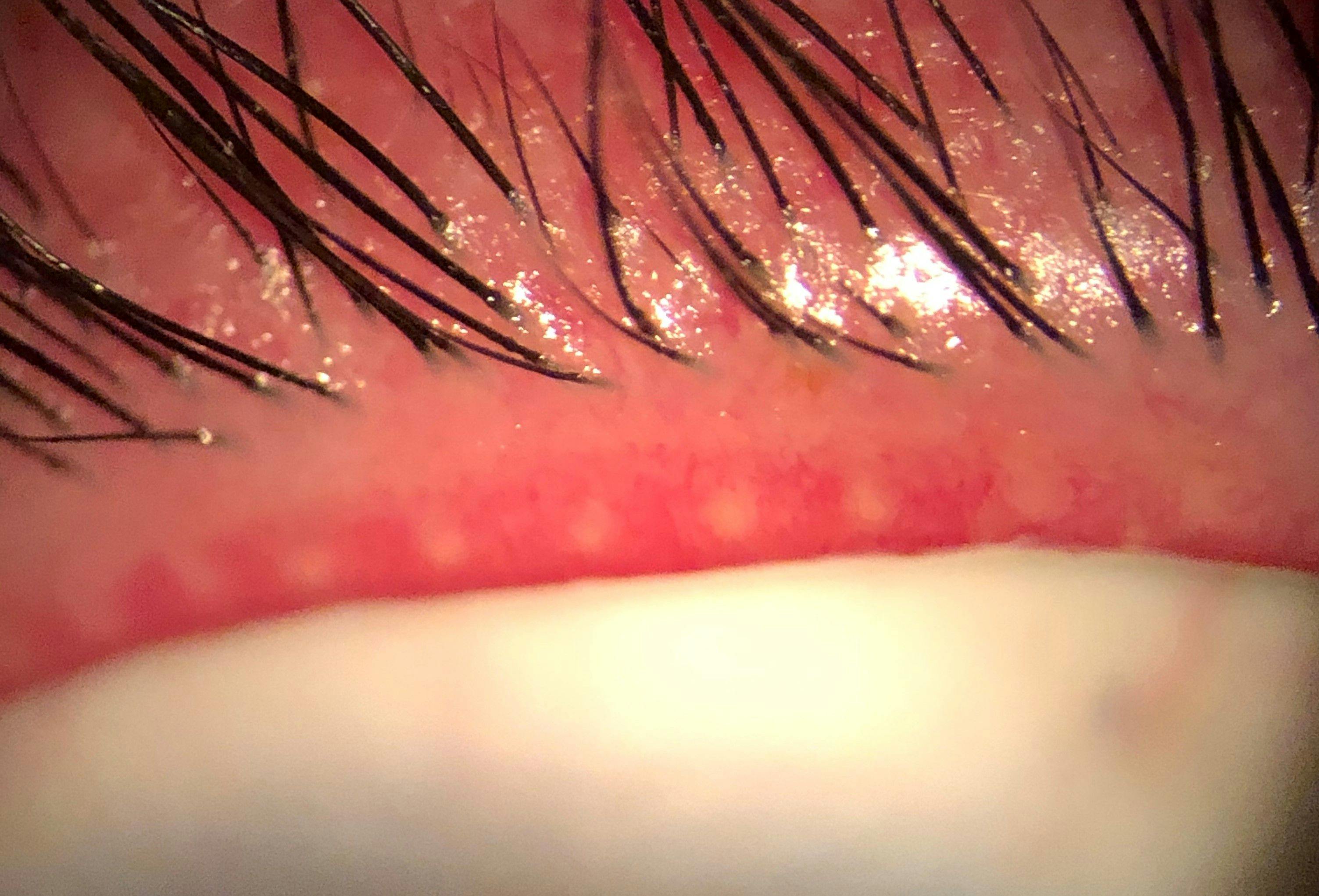
Figure 1 is a clinical image of inflamed, distended, and inspissed meibomian glands caused by MGD.
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO
These dysfunctional glands have turbid or toothpaste-like secretions upon expression rather than the typical olive-oil consistency observed in healthy glands. These findings are indicative of evaporative dry eye, as the abnormal meibum secreted (or lack of secretion) results in a poor lipid layer that causes instability and premature evaporation of the tear film.3
Evaluation through meibography
If available,
meibography is the single best way to evaluate the health of the meibomian glands, as this will display signs of meibomian gland dysfunction.
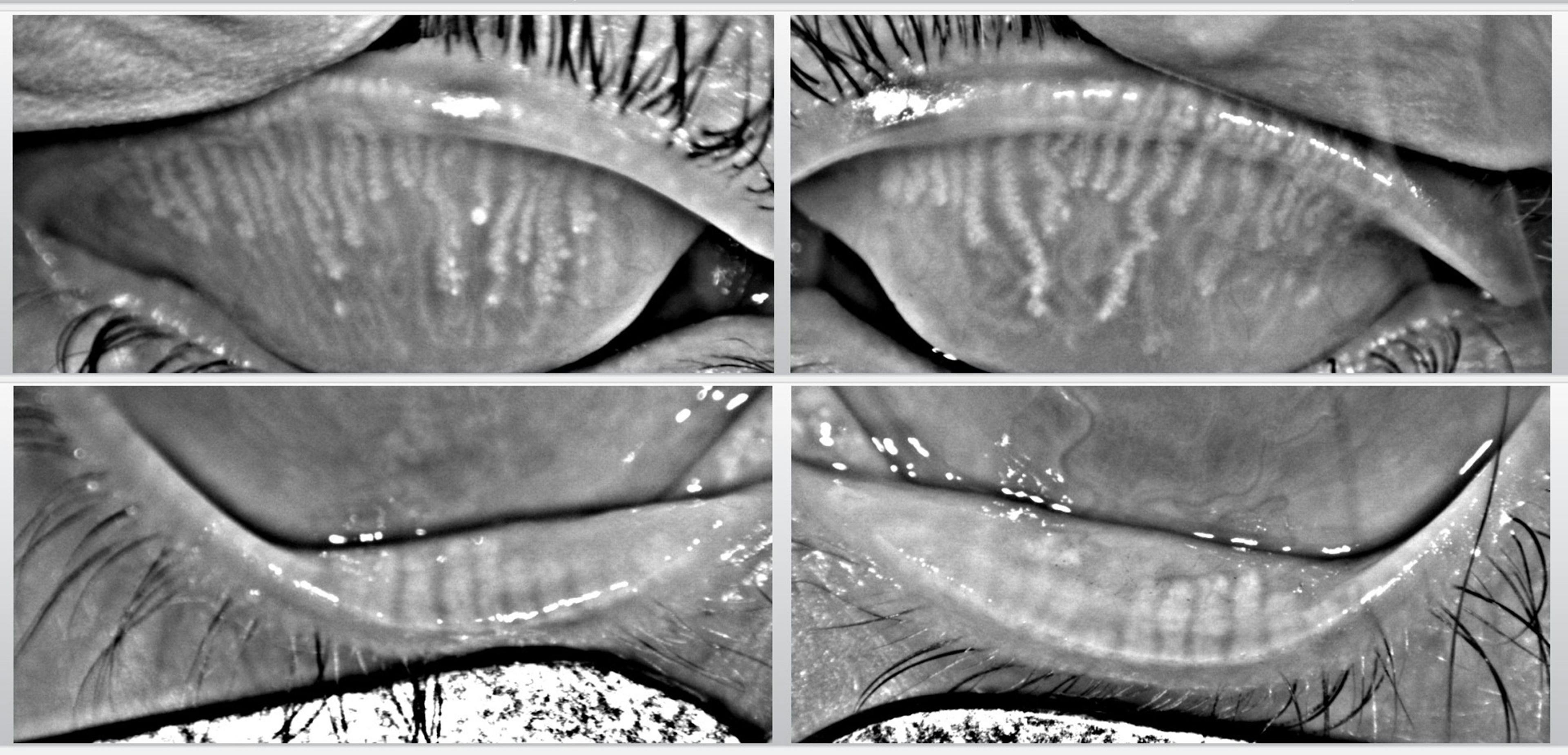
Figure 2 highlights meibography OU showing meibomian gland obstruction, inflammation, and drop out.
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO
If a meibographer is unavailable, transillumination of the eyelids can also reveal the general state of the meibomian glands, including gland morphology.
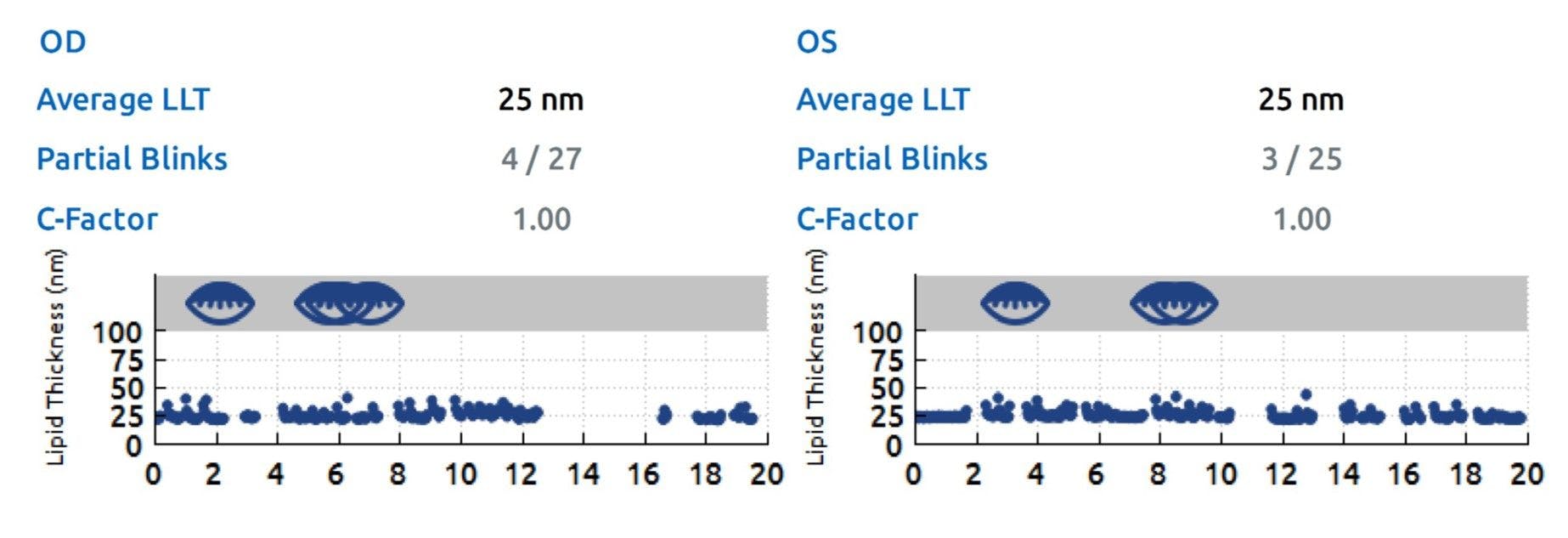
Additionally, lipid layer interferometry, such as that obtained by the
LipiView II, is an excellent way to assess meibomian gland function, as this can act as a proxy for meibum production.
Figure 3 features the results of lipid layer interferometry from the LipiView II on a patient with MGD.
Figure 3: Courtesy of Cory Lappin, OD, MS, FAAO
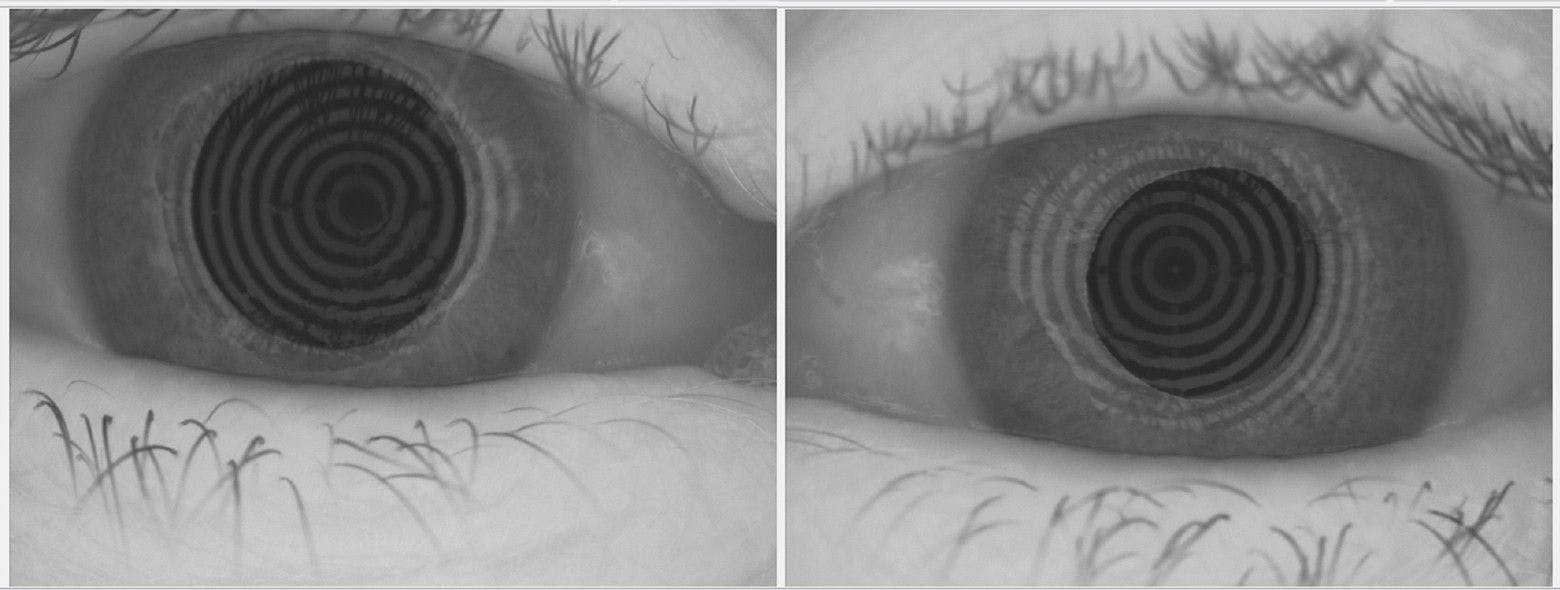
Cases of aqueous deficient dry eye, while much less common than MGD, can be identified by a low tear volume characterized by a reduced tear meniscus height (usually lower than 0.20mm), as illustrated in Figure 4.4,5
Figure 4 highlights a meibomian gland dysfunction patient with decreased tear meniscus height.
Figure 4: Courtesy of Cory Lappin, OD, MS, FAAO
Although tear production is traditionally evaluated using Schirmer strips, I have found this provides relatively little practical value as this is not a “real-world” test. By inserting the strip, you are introducing a foreign body onto the ocular surface that elicits reflex tearing which is fundamentally different than basal tear production, which is the
primary concern in dry eye. Also, performing the test with anesthetic blocks corneal nerve function, which is instrumental to normal blinking and lacrimation.
Aqueous deficient dry eye is typically associated with Sjogren’s Syndrome, so patients will also often report dry mouth and dry skin in addition to dry eye. Therefore, an effective way to assess aqueous deficiency is by evaluating tear meniscus height and taking a detailed patient history.
Analysis of tear breakup time and corneal staining
It is important to mention tear breakup time (TBUT) in the context of differentiating the causes of dry eye. While TBUT can be crucial to diagnosing dry eye in general, it is relatively nonspecific as it can be reduced in both aqueous deficient and evaporative dry eye, even though it is classically associated with
MGD.
6 Therefore, its ability to differentiate the subtypes of dry eye is somewhat limited.
Vital dyes, such as sodium fluorescein and lissamine green, are also essential to evaluate the health of the ocular surface.
Sodium fluorescein is ideal for assessing the integrity of the cornea, as it stains damaged and degenerated corneal cells as well as epithelial defects, whereas lissamine green is well-suited for evaluation of the conjunctiva (due to its enhanced contrast) where it stains dead and devitalized cells.
7 Staining, in either case, can signify the presence of dry eye and ocular surface inflammation.
7,8However, similar to TBUT, staining is relatively nonspecific in regard to the subtypes of dry eye. While the presence of SPK, which is highlighted by staining, is typically associated with aqueous deficient dry eye (due in part to its association with Sjögren’s Syndrome and the inflammatory nature of the condition), SPK and staining can also be present in MGD.9
So, while valuable in assessing the state of the ocular surface, the use of vital dyes and the presence of staining do not readily separate the different types of dry eye.
Contributing factors to dry eye with unique distinguishing features:
- The presence of lash collarettes in Demodex blepharitis10,11
- Tear saponification in bacterial blepharitis12
- The presence of telangiectatic vessels on the lid margin or conjunctiva that flare with environmental triggers in ocular rosacea13,14
- Reduced or absent corneal sensation determined by sensitivity testing with a cotton wisp in neurotrophic keratitis15,16
- Incomplete lid closure is characterized by a gap between the upper and lower lid that can be revealed using a transilluminator with the patient’s eyes closed and their head in a reclined position17,18
Final thoughts
Therefore, the true importance of distinguishing the “types” of dry eye does not necessarily lie in the ability to put a label on the diagnosis but rather in identifying the individual elements of a patient’s dry eye so each factor can be properly addressed and the condition completely treated.