



Rosacea is a chronic inflammatory disease of the skin thought to be caused by a hypersensitivity to normal environmental stimuli. It primarily affects the skin of the face including the nose, cheeks, forehead, and chin as well as the sebaceous glands present in these areas.1,2 Rosacea causes the development of dilated telangiectatic vessels, which are prone to flushing, producing the characteristic reddish complexion the condition is known for. If left untreated, rosacea can result in scarring that negatively impacts cosmetic appearance and tissue function.
Rosacea is estimated to affect up to 5% of the population,3 with 16 million Americans living with the condition.4 Rosacea most frequently occurs in middle-age, as 80% of rosacea patients are 30 years old (or older), with peak incidence occurring between 40-59 years of age.5 Children can also be affected, although this is less common.6 Females are more frequently diagnosed with facial rosacea than males; however, this may be due to a difference in care-seeking behavior.5,7 Rosacea is more common in Caucasians, particularly those with fairer skin, but can affect any race.8-10
The National Rosacea Society Expert Committee divides rosacea into four subtypes and one variant: erythematotelangiectatic, papulopustular, phymatous, ocular rosacea, and granulomatous variant.11 Subtype 4, Ocular Rosacea (OR), is a form of rosacea that primarily affects the eyelids and ocular surface. It is characterized by the growth of telangiectatic vessels on the eyelids, especially along the lid margin, and inflammation of the ocular surface, giving the eyes a chronically red appearance. dry eye, meibomian gland dysfunction (MGD), and blepharitis are commonly present along with OR, resulting in further ocular surface irritation and lid damage.
OR can occur along with facial rosacea or it can occur in isolation, but many treatments are shared between the different forms of rosacea. Likewise, as dry eye is a common comorbidity, many of the same treatments used to manage dry eye are implemented in the treatment of OR.
Unlike other forms of rosacea, OR affects males and females equally.5 Of those diagnosed with rosacea, an estimated 58-72%1,12 have OR, with an incidence of 6-72%.12-14 In 20% of rosacea cases, ocular involvement occurs before other facial signs develop, and in 90% of cases that involve both cutaneous and OR, the signs of facial rosacea are considered subtle.13
Unfortunately, this often leads to OR being overlooked and underdiagnosed because of the subtlety and nonspecific nature of its own signs and symptoms.15 Therefore, it is crucial to properly identify OR and initiate treatment, as OR can result in significant disruption to the eyelids and ocular surface with negative impacts on vision, comfort, and cosmetic appearance.
There is no cure for OR, but it can be managed. OR treatment is multi-faceted, so eyecare providers should be familiar with the condition and the treatment options available.
Etiology and Pathophysiology
While rosacea is understood to be inflammatory in nature, the exact underlying etiology of the condition is unknown.15 It is hypothesized that rosacea is caused by an abnormal response of the innate immune system to normal environmental stimuli.16-18 Research points to an abnormally high expression of Toll-like receptor 2 (TLR2) in keratinocytes of the epidermis16-18 as the mechanism responsible for this hypersensitivity.16-18 Stimulation of TLR2 receptors by environmental factors, such as extreme heat or cold, leads to increased KLK5 activity, a serine protease responsible for the production of cathelicidin.16,17
Cathelicidins are antimicrobial peptides capable of inducing inflammation and angiogenesis as part of the innate immune system.17-19 A rise in cathelicidins in turn increases VEGF expression, which results in the development of the telangiectatic vessels characteristic of rosacea. Dilation of these abnormal blood vessels produces the hallmark erythematous-flushed appearance for which rosacea is commonly known.
Other inflammatory factors have also been implicated in OR, such as MMP-8 and 9, interleukin-1α and β, ICAM-1, and TNF-α20. Additionally, patients suffering from OR display lower levels of Phospholipase A2 Group IIA, an antimicrobial protein with the ability to kill Gram-positive bacteria.21
Although these mechanistic details of rosacea are widely accepted, the ultimate cause of the abnormal immune response observed in rosacea is debated. Several organisms have been proposed as causative factors including the bacteria Helicobacter pylori and Staphylococcus epidermidis as well as the parasitic mites Demodex folliculorum and Demodex brevis.15,16,18,22-28 A genetic component has also been suggested, as rosacea is more common in certain races and ethnic groups.29
While the evidence for a bacterial origin of rosacea is mixed15, there is strong support for the role of Demodex. Demodex is an ectoparasitic mite that lives in hair follicles and sebaceous glands.30 While Demodex is part of the normal microfauna of the skin, overpopulation can cause blepharitis and MGD.31 Rosacea patients tend to display a greater presence of Demodex, and the mites are capable of eliciting the immune response observed in rosacea.26,32,33 Likewise, Demodex are more likely to be found in patients exhibiting eyelid inflammation which is commonly seen in OR.26,32,33An alternative explanation suggests Demodex are merely a vector for other infectious microorganisms, specifically Bacillus olenorium, which are ultimately responsible for inducing the inflammatory response of rosacea.16,17,27,32,34
Clinical Presentation
OR typically occurs bilaterally and can affect the eyelids and entire ocular surface.35 The most common sign of OR, and often the most common complaint, is eye redness caused by telangiectatic blood vessel growth and inflammation of the eyelids and ocular surface, especially the lid margin and intrapalpebral conjunctiva (see Figure 1). This results in the eyes exhibiting an injected, watery appearance.36

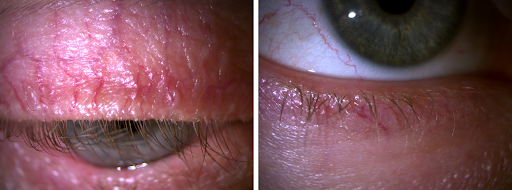
Figure 1
Common symptoms include foreign body sensation, burning, stinging, itching, dryness, photophobia, and blurry or fluctuating vision.36 The severity of OR is not usually tied to the severity of any associated cutaneous rosacea22,33,35,37,38, but rather related to the degree of telangiectasia present.39 Rosacea, including OR, is characterized by periods of relapse and remission, as well as acute exacerbations due to environmental triggers, so the severity of signs and symptoms can vary.15 Rosacea also tends to be progressive, so if left untreated the condition may worsen.15
Figure 2 demonstrates telangiectatic blood vessel growth on the lower and upper eyelids of two patients with OA.

Figure 2
Dry eye, specifically dry eye due to blepharitis and MGD, is commonly associated with OR.5,35 It is estimated that 92% of cases of OR involve MGD35, and 56-62.5% of cases involve dry eye in general33,40,41, which is likely a gross underestimation.
Figure 3 shows the meibography of a patient with OR-related MGD displaying significant meibomian gland loss in both the right and left upper and lower eyelids.

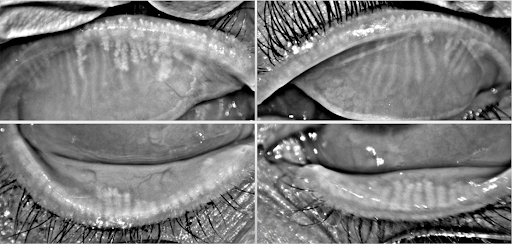
Figure 3
Because of OR’s association with MGD and blepharitis, it is common to observe inspissated meibomian glands, an accumulation of inflammatory debris on the lid margin, and a notched or scalloped appearance to the lid margin due to chronic inflammation. Collarettes and debris on the eyelashes may also be noted, suggesting Demodex blepharitis.13 The tear film is often unstable with the presence of debris and saponification, resulting in a reduced tear breakup time (TBUT).33,37,40 Recurrent hordeola and chalazia are also common MGD-related complications that occur in OR.35 However, it is important to differentiate these lid lesions from a sebaceous gland carcinoma, which can mimic a recurrent hordeolum or chalazion.42
Figure 4 illustrates lash debris and collarettes indicative of Demodex blepharitis commonly observed in OR (left) and significant scalloping or notching of the lid margin due to chronic OR-related inflammation (right).


Figure 4
OR can induce a chronic papillary reaction of the palpebral conjunctiva13 due to persistent inflammation of the ocular surface. If unchecked, this prolonged inflammation can result in significant scarring, including conjunctival cicatrization.43,44
Rosacea keratitis is a major concern for patients with OR due to potentially vision-threatening complications. Corneal involvement occurs in about 1/3 of OR cases.1,13 Rosacea keratitis typically begins with the appearance of superficial punctate keratitis, usually on the inferior aspect of the cornea followed by development of peripheral neovascularization and inflammatory subepithelial infiltrates as the condition progresses.1,35,45,46 If left untreated, these subepithelial infiltrates can develop into ulcers that can cause vision-threatening scarring or even corneal perforation.35,45,46
In Figure 5, we see peripheral neovascularization of of the right and left cornea of a patient with rosacea keratitis.

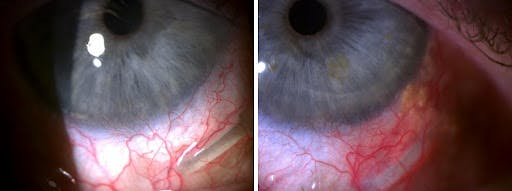
Figure 5
Other potential ocular disorders associated with OR include recurrent corneal erosions (RCE)47-49 and inflammatory conditions like episcleritis, scleritis, and iritis.35, 50
The global ROSacea COnsensus (ROSCO) expert panel has devised a grading scale specifically for OR that is based upon the extent of tissue involvement.51 Mild OR consists of mild blepharitis with lid margin telangiectasia, Mild-to-Moderate OR is characterized by blepharoconjunctivitis, Moderate-to-Severe OR entails blepharokeratoconjunctivitis, and Severe OR is defined as sclerokeratitis and/or the presence of anterior uveitis.51
Figure 6 illustrates a patient with moderate to severe OR displaying eyelid, conjuntival, and corneal involvement who has also developed trichiasis due to chronic blepharitis disrupting the normal architecture of the left lower lid margin.
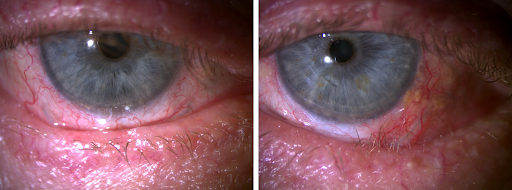
Figure 6
Differential Diagnosis
The diagnosis of all types of rosacea, including OR, is made clinically, based upon signs and symptoms.35 However, most of these signs and symptoms are subtle and nonspecific which makes differentiating OR from other ocular surface conditions, such as dry eye and blepharitis, a challenge, as they share similar presentations and often occur concomitantly.35
For this reason, the National Rosacea Society Expert Committee recommends considering a diagnosis of OR if one or more of the previously listed signs or symptoms are present.36 Therefore, recognizing the characteristic features of rosacea, such as acute exacerbations that occur with certain triggers, in the presence of other nonspecific findings can ultimately lead to a diagnosis of OR.
Treatment
While not curable, OR is treatable11, so it is important for eye care providers to familiarize themselves with the treatment options available. Additionally, dry eye conditions such as MGD and blepharitis usually occur alongside OR, so these disorders must also be addressed as part of a complete treatment regimen11. For this reason, the treatment protocols used for OR often mirror those used in the treatment of dry eye.
Trigger Avoidance
A key feature of all types of rosacea is a hypersensitivity to normal environmental stimuli that triggers inflammation and vasodilation. This induces the characteristic flushing of facial rosacea and exacerbates ocular irritation and discomfort in patients with OR. Triggers vary from person to person, so a central element to any rosacea treatment plan involves identifying and avoiding irritating stimuli.7
Some of the most common triggers include:2,11,35,52
- Environmental stimuli
- Extreme heat
- Extreme cold
- Wind and sun exposure
- Emotional triggers
- Stress
- Anger
- Embarrassment
- Physiological stimuli
- Strenuous exercise
- Dietary triggers
- Caffeine
- Chocolate
- Alcohol
- Dairy products
- Hot beverages
- Spicy food
- Pharmaceuticals and supplements
- Nasal and topical (cutaneous) steroids
- Beta blockers
- Amiodarone
- Niacin
- Vitamins B6 and B12
- Certain cosmetics
To help patients identify their specific triggers, they can be advised to keep a rosacea diary in which they track their symptoms, symptom severity, and any associated foods, activities, medications, or cosmetics.
Topical Cutaneous Treatments
Two of the most commonly used cutaneous rosacea treatments are metronidazole, a topical antibiotic available in 0.75% and 1% formulations (Rosadan, G&W Laboratories) and azelaic acid, a topical antiseptic available in a 15% gel and 20% cream (Azelex, Allergan). Both medications have anti-inflammatory properties and are used BID, although studies have shown no difference in efficacy when azelaic acid is dosed QD rather than BID.53 While these treatments are primarily intended for facial rosacea, metronidazole can also be beneficial in treating eyelid-related inflammation.54 It is advised to consult the patient’s co-managing dermatologist regarding the use of topical cutaneous therapies.
Artificial Tears
The use of artificial tears (AT) in OR is primarily palliative, but ATs offer quick relief and can prevent irritation when used prophylactically. Lipid-based ATs are the lubricating drops of choice for OR, as they help stabilize the lipid component of the tear film which is often disrupted by MGD.55 There is also evidence lipid-based ATs are capable of reducing inflammatory factors present in the tear film.55 ATs are usually dosed QID to PRN.
If a patient feels the need to use ATs more than four times per day, a preservative-free AT is strongly recommended, as they otherwise risk developing surface toxicity due to repeated preservative exposure. However, if a patient is using ATs more frequently than QID, that is an indication additional treatments may be needed to manage their discomfort. Refresh Optive Mega-3 (Allergan)is an excellent choice for use in OR, as it is a preservative free lipid-based AT.
Lid Hygiene
Lid hygiene is another important element of OR treatment. While general cleansers like baby shampoo have been used in the past, there are better and more effective options available. Tea tree oil (Melaleuca alternifolia) has anti-inflammatory and antimicrobial properties, as well as the ability to eradicate Demodex, making it an ideal treatment for OR.31 Tea tree oil comes in several forms, including lid scrubs and foaming cleansers. It is recommended that 50% tea tree oil be used BID for a minimum of six weeks to ensure eradication of Demodex, as this corresponds to two life cycles of the mites.56 It can then be used daily for prophylaxis.
Although tea tree oil has demonstrated effectiveness against Demodex and its use is widespread, there is currently no FDA-approved treatment for Demodex. However, the use of 0.25% lotilaner ophthalmic solution is currently being investigated as a novel treatment for Demodex blepharitis.57
Another option in terms of lid hygiene is hypochlorous acid (HOCl). Hypochlorous acid is an antiseptic that is naturally produced by leukocytes of the immune system to neutralize bacterial toxins58 and exhibits anti-inflammatory properties. Due to its broad antibacterial activity, HOCl works well in reducing overgrowth of Staphylococcus epidermidis, which can contribute to blepharitis and tear film saponification observed in OR.21
Lid Therapies
Given the presence of MGD in the majority of cases of OR, addressing the eyelids and associated structures is a core element of a comprehensive management plan. Conservative treatment may involve using warm compresses followed by lid massage to liberate clogged meibum present in the meibomian glands. However, the temperature achieved by most warm compresses is unlikely to reach that required to completely liquefy the oil, so this treatment is primarily palliative.59
While warm compresses are helpful in treating MGD, they should be used cautiously in the presence of OR, as the heat from the compress may exacerbate any present inflammation. If a patient can use compresses without issue, they can be performed daily or as needed. A mask-like compress specifically made for the treatment of MGD, such as a Bruder Moist Heat Eye Compress (Bruder) or Dry Eye Relief Mask (EyeEco), is preferable to “homemade” compresses, such as a washcloth or rice-filled sock, as these masks retain heat for a longer duration and the level of heat is more controlled.
Patients are also advised to perform blink exercises consisting of several complete blinks followed by a sustained forceful blink. This exaggerated blinking practice encourages proper blinking mechanics and behavior60, which are critical for normal meibum secretion and tear film renewal. Blinking exercises can be recommended as often as every 20 minutes, or as frequently as is practical.
More advanced treatment of MGD involves in-office thermal pulsation procedures, such as LipiFlow® (Johnson & Johnson), iLux® (Alcon), or TearCare® (Sight Sciences). Thermal pulsation treatment has been shown to improve signs and symptoms of MGD.61,62 Thermal pulsation involves heating the meibum inside the meibomian glands to its melting point by warming the lids to a temperature of about 42.5°C63 followed by mechanical pulsation to express the oil from the glands.64 Through expression, the meibomian glands are essentially “reset” as they are cleared of any clogged oil and primed to produce new meibum. During this period patients are strongly encouraged to take an omega-3 supplement if they are not already doing so, as omega-3 fatty acid supplementation improves the quality of the meibum produced.35
Microblepharoexfoliation, such as BlephEx® (Alcon), can be used as an adjunct to thermal pulsation procedures or as a standalone therapy. In blepharitis, inflammatory debris and bacterial biofilm can build up on the lid margin, causing chronic inflammation that results in scarring and keratinization. This debris may also obstruct the meibomian glands, worsening MGD and making the patient prone to hordeolum and chalazion development. Debridement of the lid margin with microblepharoexfoliation removes inflammatory debris, reduces the bacterial load, and decreases the number of Demodex present.65 Performing debridement prior to thermal pulsation also ensures the terminal ends of the meibomian glands are patent, allowing for improved gland expressibility and better treatment outcomes.
Oral Antibiotics
Oral antibiotics, specifically tetracyclines, are considered by many to be a standard of care for rosacea, including OR.50,66 The most commonly used oral tetracycline is doxycycline due to its better tolerability, lower side effect profile, and less frequent dosing when compared with other tetracyclines.15 Doxycycline has multiple benefits including anti-inflammatory and anti-angiogenic effects.15,67 Doxycycline not only improves inflammation caused by rosacea, but also has positive effects on MGD and dry eye as well.68 Doxycycline reduces inflammation by inhibiting MMP-969,70 and VEGF15, and improves meibum quality.68
The specific formulation of doxycycline and dosing frequency used to treat OR is provider dependent, as there is no established standard dose or duration of treatment.71 Typically, a loading dose is initiated followed by a lower maintenance dose. This often involves using 40-100 mg QD-BID for one-two weeks followed by 20-40 mg QD for one-four months. Some providers prefer to keep patients on a low, long-term maintenance dose, whereas others prefer to use shorter courses of doxycycline, discontinuing and restarting its use as needed.20
When doxycycline is used for rosacea, it is usually prescribed below its minimum effective dose for antibacterial activity because at low doses (20-40 mg) it retains its anti-inflammatory properties without inducing antibacterial effects. This is appropriate for the treatment of OR, as doxycycline is utilized for its anti-inflammatory effects rather than its antibacterial activity.69 The use of lower doses also increases tolerability and reduces likelihood of antibiotic resistance.72,73
Generic doxycycline can effectively be used in the treatment of OR, however, a unique formulation of doxycycline indicated specifically for use in rosacea is available in the form of Oracea (Galderma). Oracea is formulated as a 40 mg tablet consisting of 30 mg of immediate-release and 10 mg of extended-release doxycycline and is taken once daily.74 Oracea has been shown to be effective for up to four months and safe for up to nine months.20
Doxycycline should not be used in women who are pregnant or nursing, and in children under seven years of age as it can have adverse effects on bone and tooth development.75 It is also important to counsel patients on the potential side effects of doxycycline including GI disturbances and increased photosensitivity.15
In cases where doxycycline is contraindicated, or the patient is non-responsive to its use, azithromycin is a good alternative.12,76,77 Azithromycin is a macrolide antibiotic that can also decrease inflammation and improve symptoms of OR when dosed 500 mg QD for two weeks.12
Other oral medications that have been used in the treatment of rosacea and OR include tetracycline, minocycline, and isotretinoin (Accutane). These are not usually recommended as tetracycline’s short half-life requires more frequent dosing (QID compared to QD-BID for doxycycline20), minocycline has little evidence to support its use in treating rosacea and carries more side effects2, and while isotretinoin may be helpful for facial rosacea, its side effects include blepharitis, conjunctivitis, and meibomian gland destruction which can all worsen OR.78
Topical Antibiotics
Topical antibiotics can also be useful therapies in the treatment of OR. Erythromycin 0.5% ophthalmic ointment applied QHS can be used as a nocturnal therapy to decrease bacterial burden on the lids and provide lubrication throughout the night.38 However, some patients may find erythromycin irritating in which case other topical ointments and gels can be utilized for nighttime comfort.
A novel treatment involves the off-label use of topical azithromycin. The application of Azasite (azithromycin 1% ophthalmic solution, Akorn Pharmaceuticals) to the lid margin has been shown to improve MGD and decrease inflammation79. Azithromycin penetrates tissue well and has a prolonged duration of action, so treatment is started with a loading dose followed by a lower maintenance dose. Two potential dosing schedules are BID for 2 days followed by QD for 30 days or QHS for 2 weeks then twice per week as maintenance.
Topical Anti-inflammatories
Topical corticosteroids are excellent for treating acute inflammation but are not ideal for long-term OR management due to the risk of intraocular pressure spikes and cataract development.35 A soft steroid with a lower side effect profile, such as loteprednol etabonate, is a good choice for treating OR flares, however stronger steroids may be necessary depending on the degree of inflammation present. A typical dosing protocol to relieve initial inflammation or control an acute flare would be 0.5% loteprednol etabonate BID-QID for one-two weeks, but longer tapered dosing of up to four weeks may be necessary.
It is worth noting topical steroid use itself can trigger flares in rosacea patients.80 Although this is typically seen with cutaneous and nasal preparations, it is another reason steroids are best suited for treating acute episodes rather than long-term inflammation control.
Other anti-inflammatory medications, such as Xiidra (5% lifitegrast ophthalmic solution, Novartis), Cequa (0.09% cyclosporine ophthalmic solution, Sun Pharmaceuticals), and Restasis (0.05% cyclosporine ophthalmic emulsion, Allergan) are better suited for the management of chronic inflammation associated with OR. All three drops are dosed BID and can safely be used long-term. Lifitegrast and cyclosporine both reduce inflammation by inhibiting the activity of T cells but act through different mechanisms. Lifitegrast blocks LFA-1 from binding ICAM-181-83, whereas cyclosporine inhibits calcineurin.84 Lifitegrast may be particularly helpful in treating OR-related inflammation, as ICAM-1 is elevated in OR.40
Topical preparations of tacrolimus have also shown promise in managing OR and associated blepharitis and MGD. One study found improvements in erythema, meibomian gland secretion, and lid telangiectasia after dosing tacrolimus 0.03% ointment BID for four weeks.85 Tacrolimus is a calcineurin inhibitor similar to cyclosporine.86
Diet and Supplements
Dietary supplements play an important role in OR management. Numerous studies have demonstrated the benefits of omega-3 fatty acid consumption including anti-inflammatory effects.87-89 Omega-3 supplementation is a mainstay of MGD treatment as it improves the signs and symptoms of the condition.35,90,91 However, not all omega-3 supplements are of the same quality, which can significantly impact efficacy. Therefore, it is strongly recommended that patients use a high quality, re-esterified, triglyceride-based omega-3 supplement with a 3:1 EPA to DHA ratio and at least 2 grams of combined EPA and DHA to achieve the optimal benefits of supplementation, as this specific formulation has been shown to effectively improve MGD.92
Beyond avoidance of triggering foods, early research suggests other dietary practices may also aid in the management of rosacea. The use of probiotics can potentially alleviate rosacea signs and symptoms,93 and a high fiber diet may be helpful as well.94
Intense Pulsed Light (IPL)
Intense Pulsed Light (IPL) is a noninvasive procedure that entails applying high intensity polychromatic light (515-1200 nm) directly to the skin. IPL has several potential mechanisms of action that address inflammation, erythema, and MGD, as well as bacterial and Demodex blepharitis95, making it one of the most promising treatments for OR. When used for OR and dry eye, treatment is applied to the periocular region from tragus to tragus, with shields in place over the eyelids or corneas.96 The standard protocol involves four total treatments, typically spaced three-four weeks apart.96,97 However, additional treatments can be added if necessary, and many patients require maintenance treatments in the future.
While the use of IPL for the treatment of rosacea is widely supported98, the exact underlying mechanisms of IPL are unknown.95 It is thought IPL acts through photobiomodulation. Photobiomodulation refers to the process of delivering energy to a target tissue in the form of light, which stimulates intracellular biological processes at the gene and protein levels which can trigger anti-inflammatory mechanisms.95,99,100
In the context of ocular surface and dry eye disease, IPL reduces inflammation and improves the signs and symptoms of dry eye and MGD.95,101 It is thought to improve inflammation on the ocular surface by stimulating production of anti-inflammatory cytokines while decreasing proinflammatory factors.102-107 In terms of MGD, it has been proposed that the energy delivered by the light is great enough to liquefy meibum in clogged glands108,109 thereby improving the quality of secretions. IPL is also capable of eradicating Demodex, as pigment in the mite’s exoskeleton absorbs light energy produced by IPL leading to its destruction.110, 111 Additionally, IPL decreases the bacterial load present on the lid margins.95 Cosmetically, IPL improves the appearance of facial and ocular erythema by destroying telangiectatic vessels.95,98
Although IPL has been used for the treatment of ocular surface conditions like dry eye and MGD for over a decade, this use was off label. However, the OptiLight™ IPL device (Lumenis)recently received FDA-approval for the treatment of MGD and dry eye112,113 making this use of IPL an on-label indication. Seeing as IPL is capable of treating OR through several mechanisms using a single modality, it makes the procedure an ideal treatment option.
Other Treatment
Other treatments in the management of OR include vasoconstrictive agents. Although oral antibiotics, lid hygiene, and topical anti-inflammatories can reduce erythema associated with inflammation, they do not address redness due to the perpetually dilated state of telangiectatic vessels.2 Vasoconstrictors are helpful in addressing this source of redness, which is especially useful in improving cosmetic appearance.
Lumify (0.025% brimonidine tartrate ophthalmic solution, Bausch + Lomb) is a highly selective α2-adrenergic agonist, which causes constriction of the conjunctival veins and venules resulting in a whiter appearance of the eyes.114 Additionally, instances of rebound redness and tachyphylaxis–which products like Visine (0.05% tetrahydrozoline hydrochloride, Johnson & Johnson) and ClearEyes (0.012% naphazoline hydrochloride, Prestige Consumer Healthcare) are known for115,116–are rare with brimonidine use.114 Therefore, Lumify can be a powerful tool in managing a patient’s cosmetic concerns as it relieves ocular injection within minutes, can be used up to four times per day, and lasts for five-eight hours.117,118
While punctal plugs are sometimes used in the management of dry eye, their use in the presence of OR is controversial. The therapeutic goal of plugs is increasing the tear volume that remains on the ocular surface by reducing drainage through the puncta. But in the case of OR, numerous inflammatory factors are elevated in the tear film119, so occluding the puncta may create a “cesspool” effect, in which a stagnant pool of inflammatory factors remains on the ocular surface for a longer period provoking further inflammation.
The use of amniotic membranes can be helpful in more severe corneal cases of OR, particularly in cases of persistent epithelial defects and ulceration. Amniotic membranes have robust anti-inflammatory and healing properties120 that can be a powerful tool in managing rosacea keratitis.
Figure 7 shows the progression of an OR patient before and after initiating a treatment protocol, including doxycycline, omega-3 supplements, hypochlorous acid, Xiidra, Lumify, and IPL.

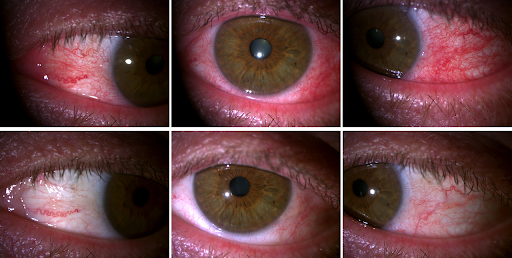
Figure 7
Can OR patients wear contact lenses?
A particular area of concern for some OR patients is contact lens wear. While OR patients can wear contact lenses successfully, it is best to advise these patients to avoid lens wear during periods of acute inflammation or, ideally, discontinue lens wear until their condition is well controlled, as contact lens wear itself may be intrinsically inflammatory.121
Likewise, the health of the ocular surface should be optimized before fitting lenses in OR patients. It is strongly recommended for OR patients to be fit in daily disposable lenses for increased comfort and ocular surface health. In some cases, it may be necessary for patients to discontinue contact lens wear indefinitely if lens use appears to be a significant irritant or elicits worsening of their condition, such as increased neovascularization.
Patient education on ocular rosacea
Patient education is a critical component of OR treatment.
A typical script would be:
“Rosacea is an inflammatory disease that affects the skin and oil glands of the face, which causes development of spider-like blood vessels. These blood vessels are prone to dilating which causes the facial redness you may experience when you eat spicy food or go out in cold weather. OR is a form of rosacea that mainly affects your eyelids and eyes and causes redness and irritation. It is possible for you to have OR without facial rosacea, which is very common. Many people with OR also have dry eye, so you may also be experiencing a gritty or burning sensation. Rosacea and OR cannot be cured but there are many treatments we can use to help manage it and keep it under control.”
Emphasizing that OR is not curable but can be managed will help set expectations as well as help the patient understand why some treatments require long-term use.
Additionally, it is beneficial to explain the role each treatment element plays, as patients are more likely to be compliant with a treatment program if they understand the purpose of each part.
Summary
OR can have a significant impact on ocular health, appearance, and comfort. However, because many of its signs and symptoms are nonspecific and it is not as easily recognizable as other forms of rosacea, OR often goes undiagnosed. Additionally, the majority of cases of OR include other conditions such as blepharitis and MGD, which will also need to be treated.
A complete OR treatment plan often involves a mix of oral antibiotics, topical anti-inflammatory drops, palliative therapies, lid hygiene, supplements, trigger avoidance, and more advanced procedures such as thermal pulsation and IPL. Therefore, it is important for eyecare providers to familiarize themselves with the condition and the various treatment options available.
References
- Starr PA, Macdonald A. Oculocutaneous aspects of rosacea. Proc R Soc Med. 1969;62(1):9-11.
- Oge’ LK, Muncie HL, Phillips-Savoy AR. Rosacea: diagnosis and treatment. Am Fam Physician. 2015;92(3):187-196.
- Elewski BE, Draelos Z, Dréno B, Jansen T, Layton A, Picardo M. Rosacea - global diversity and optimized outcome: proposed international consensus from the Rosacea International Expert Group. J Eur Acad Dermatol Venereol. 2011;25(2):188-200
- Drake L, ed. Rosacea Now Estimated to Affect at Least 16 Million Americans. Rosacea Review. Rosacea.org website. https://www.rosacea.org/rosacea-review/2010/winter/rosacea-now-estimated-to-affect-at-least-16-million-americans. 2010. Accessed June 27, 2021.
- Spoendlin J, Voegel JJ, Jick SS, Meier CR. A study on the epidemiology of rosacea in the U.K. Br J Dermatol. 2012;167(3):598-605
- Hong E, Fischer G. Childhood ocular rosacea: considerations for diagnosis and treatment. Australas J Dermatol. 2009;50(4):272-27
- Baldwin HE. Diagnosis and treatment of rosacea: state of the art. J Drugs Dermatol. 2012;11(6):725-730.
- Browning DJ, Rosenwasser G, Lugo M. Ocular rosacea in blacks. Am J Ophthalmol. 1986;101(4):441-444.
- Alexis AF, Callender VD, Baldwin HE, Desai SR, Rendon MI, Taylor SC. Global epidemiology and clinical spectrum of rosacea, highlighting skin of color: Review and clinical practice experience. J Am Acad Dermatol. 2019;80(6):1722-1729.e7.
- Abram K, Silm H, Oona M. Prevalence of rosacea in an Estonian working population using a standard classification. Acta Derm Venereol. 2010;90(3):269-273.
- Wladis EJ, Adam AP. Treatment of ocular rosacea. Surv Ophthalmol. 2018;63(3):340-346.
- Bakar O, Demircay Z, Toker E, Cakir S. Ocular signs, symptoms and tear function tests of papulopustular rosacea patients receiving azithromycin. J Eur Acad Dermatol Venereol. 2009;23(5):544-549
- Ghanem VC, Mehra N, Wong S, Mannis MJ. The prevalence of ocular signs in acne rosacea: comparing patients from ophthalmology and dermatology clinics. Cornea. 2003;22(3):230-233.
- Wise G. Ocular rosacea. Am J Ophthalmol. 1943;26:591-609.
- Vieira ACC, Höfling-Lima AL, Mannis MJ. Ocular rosacea--a review. Arq Bras Oftalmol. 2012;75(5):363-369.
- Yamasaki K, Kanada K, Macleod DT, et al. TLR2 expression is increased in rosacea and stimulates enhanced serine protease production by keratinocytes. J Invest Dermatol. 2011;131(3):688-697.
- Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77-81.
- Del Rosso JQ. Advances in understanding and managing rosacea: part 1: connecting the dots between pathophysiological mechanisms and common clinical features of rosacea with emphasis on vascular changes and facial erythema. J Clin Aesthet Dermatol. 2012;5(3):16-25.
- Zanetti M. Cathelicidins, multifunctional peptides of the innate immunity. J Leukoc Biol. 2004;75(1):39-48.
- Awais M, Anwar MI, Iftikhar R, Iqbal Z, Shehzad N, Akbar B. Rosacea - the ophthalmic perspective. Cutan Ocul Toxicol. 2015;34(2):161-166.
- Kari O, Aho VV, Peltonen S, et al. Group IIA phospholipase A(2) concentration of tears in patients with ocular rosacea. Acta Ophthalmol Scand. 2005;83(4):483-486.
- Crawford GH, Pelle MT, James WD. Rosacea: I. Etiology, pathogenesis, and subtype classification. J Am Acad Dermatol. 2004;51(3):327-341; quiz 342-344.
- Lacey N, Delaney S, Kavanagh K, Powell FC. Mite-related bacterial antigens stimulate inflammatory cells in rosacea. Br J Dermatol. 2007;157(3):474-481.
- Szlachcic A, Sliwowski Z, Karczewska E, Bielański W, Pytko-Polonczyk J, Konturek SJ. Helicobacter pylori and its eradication in rosacea. J Physiol Pharmacol. 1999;50(5):777-786.
- Diaz C, O’Callaghan CJ, Khan A, Ilchyshyn A. Rosacea: a cutaneous marker of Helicobacter pylori infection? Results of a pilot study. Acta Derm Venereol. 2003;83(4):282-286.
- Lazaridou E, Giannopoulou C, Fotiadou C, Vakirlis E, Trigoni A, Ioannides D. The potential role of microorganisms in the development of rosacea. J Dtsch Dermatol Ges. 2011;9(1):21-25.
- O’Reilly N, Menezes N, Kavanagh K. Positive correlation between serum immunoreactivity to Demodex-associated Bacillus proteins and erythematotelangiectatic rosacea. Br J Dermatol. 2012;167(5):1032-1036.
- Whitfeld M, Gunasingam N, Leow LJ, Shirato K, Preda V. Staphylococcus epidermidis: a possible role in the pustules of rosacea. J Am Acad Dermatol. 2011;64(1):49-52
- Steinhoff M, Buddenkotte J, Aubert J, et al. Clinical, cellular, and molecular aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011;15(1):2-11.
- Steinhoff M, Schauber J, Leyden JJ. New insights into rosacea pathophysiology: a review of recent findings. J Am Acad Dermatol. 2013;69(6 Suppl 1):S15-26.
- Liu J, Sheha H, Tseng SCG. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010;10(5):505-510.
- Li J, O’Reilly N, Sheha H, et al. Correlation between ocular Demodex infestation and serum immunoreactivity to Bacillus proteins in patients with Facial rosacea. Ophthalmology. 2010;117(5):870-877.e1.
- Lazaridou E, Fotiadou C, Ziakas NG, Giannopoulou C, Apalla Z, Ioannides D. Clinical and laboratory study of ocular rosacea in northern Greece. J Eur Acad Dermatol Venereol. 2011;25(12):1428-1431.
- Meyer-Hoffert U, Schröder J-M. Epidermal proteases in the pathogenesis of rosacea. J Investig Dermatol Symp Proc. 2011;15(1):16-23.
- Oltz M, Check J. Rosacea and its ocular manifestations. Optometry. 2011;82(2):92-103.
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the national rosacea society expert committee on the classification and staging of rosacea. J Am Acad Dermatol. 2002;46(4):584-587.
- Quarterman MJ, Johnson DW, Abele DC, Lesher JL, Hull DS, Davis LS. Ocular rosacea. Signs, symptoms, and tear studies before and after treatment with doxycycline. Arch Dermatol. 1997;133(1):49-54.
- Odom R, Dahl M, Dover J, et al. Standard management options for rosacea, part 2: options according to subtype. Cutis. 2009;84(2):97-104.
- Keshtcar-Jafari A, Akhyani M, Ehsani AH, et al. Correlation of the severity of cutaneous rosacea with ocular rosacea. Indian J Dermatol Venereol Leprol. 2009;75(4):405-406.
- Pisella PJ, Brignole F, Debbasch C, et al. Flow cytometric analysis of conjunctival epithelium in ocular rosacea and keratoconjunctivitis sicca. Ophthalmology. 2000;107(10):1841-1849.
- Gudmundsen KJ, O’Donnell BF, Powell FC. Schirmer testing for dry eyes in patients with rosacea. J Am Acad Dermatol. 1992;26(2 Pt 1):211-214.
- Doxanas MT, Green WR. Sebaceous gland carcinoma. Review of 40 cases. Arch Ophthalmol. 1984;102(2):245-249.
- Cohen AF, Tiemstra JD. Diagnosis and treatment of rosacea. J Am Board Fam Pract. 2002;15(3):214-217.
- Ravage ZB, Beck AP, Macsai MS, Ching SST. Ocular rosacea can mimic trachoma: a case of cicatrizing conjunctivitis. Cornea. 2004;23(6):630-631.
- Gracner B, Pahor D, Gracner T. [Repair of an extensive corneoscleral perforation in a case of ocular rosacea with a keratoplasty]. Klin Monbl Augenheilkd. 2006;223(10):841-843.
- Al Arfaj K, Al Zamil W. Spontaneous corneal perforation in ocular rosacea. Middle East Afr J Ophthalmol. 2010;17(2):186-188.
- Akpek EK, Merchant A, Pinar V, Foster CS. Ocular rosacea: patient characteristics and follow-up. Ophthalmology. 1997;104(11):1863-1867.
- Jenkins MS, Brown SI, Lempert SL, Weinberg RJ. Ocular rosacea. Am J Ophthalmol. 1979;88(3 Pt 2):618-622.
- Ramamurthi S, Rahman MQ, Dutton GN, Ramaesh K. Pathogenesis, clinical features and management of recurrent corneal erosions. Eye (Lond). 2006;20(6):635-644.
- Alvarenga LS, Mannis MJ. Ocular rosacea. Ocul Surf. 2005;3(1):41-58.
- Tan J, Almeida LMC, Bewley A, et al. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (Rosco) panel. Br J Dermatol. 2017;176(2):431-438.
- Levin J, Miller R. A guide to the ingredients and potential benefits of over-the-counter cleansers and moisturizers for rosacea patients. J Clin Aesthet Dermatol. 2011;4(8):31-49.
- Thiboutot DM, Fleischer AB, Del Rosso JQ, Graupe K. Azelaic acid 15% gel once daily versus twice daily in papulopustular rosacea. J Drugs Dermatol. 2008;7(6):541-546.
- Barnhorst DA, Foster JA, Chern KC, Meisler DM. The efficacy of topical metronidazole in the treatment of ocular rosacea. Ophthalmology. 1996;103(11):1880-1883.
- Lim A, Wenk MR, Tong L. Lipid-based therapy for ocular surface inflammation and disease. Trends Mol Med. 2015;21(12):736-748.
- Cheng AM, Sheha H, Tseng SC. Recent advances on ocular Demodex infestation. Curr Opin Ophthalmol. 2015;26(4):295-300.
- Tarsus Pharmaceuticals, Inc. Announces Positive Results of Saturn-1 Pivotal Trial Evaluating TP-03 for the Treatment of Demodex Blepharitis. Tarsus Pharmaceuticals website. https://ir.tarsusrx.com/news-releases/news-release-details/tarsus-pharmaceuticals-inc-announces-positive-results-saturn-1. June 21, 2021. Accessed July 1, 2021.
- Epitropoulos AT. Lid hygiene product helps reduce blepharitis, MGD symptoms. Ophthalmology Times. November 15, 2015. Accessed June 27, 2021.
- Schubert JR, Murakami DK, Blackie CA, Korb DR. Using warm compresses to treat meibomian gland disease. Optometry Times. https://www.optometrytimes.com/view/using-warm-compresses-treat-meibomian-gland-disease. Published August 11, 2015. Accessed June 29, 2021.
- Collins M, Heron H, Larsen R, Lindner R. Blinking patterns in soft contact lens wearers can be altered with training. Am J Optom Physiol Opt. 1987;64(2):100-3.).
- Greiner JV. Long-term (12-month) improvement in meibomian gland function and reduced dry eye symptoms with a single thermal pulsation treatment. Clin Exp Ophthalmol. 2013;41(6):524-530.
- Blackie CA, Coleman CA, Holland EJ. The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clin Ophthalmol. 2016;10:1385-1396.
- Borchman D. The optimum temperature for the heat therapy for meibomian gland dysfunction. Ocul Surf. 2019;17(2):360-364.
- Tavassoli S, Wong N, Chan E. Ocular manifestations of rosacea: A clinical review. Clin Exp Ophthalmol. 2021;49(2):104-117.
- Connor CG, Narayanan S, Miller W. Reduction in inflammatory marker matrix metalloproteinase-9 following lid debridement with BlephEx. Invest Ophthalmol Vis Sci. 2017;58(8):498-498.
- Pfeffer I, Borelli C, Zierhut M, Schaller M. Treatment of ocular rosacea with 40 mg doxycycline in a slow release form. J Dtsch Dermatol Ges. 2011;9(11):904-907.
- Frucht-Pery J, Sagi E, Hemo I, Ever-Hadani P. Efficacy of doxycycline and tetracycline in ocular rosacea. Am J Ophthalmol. 1993;116(1):88-92.
- Dougherty JM, McCulley JP, Silvany RE, Meyer DR. The role of tetracycline in chronic blepharitis. Inhibition of lipase production in staphylococci. Invest Ophthalmol Vis Sci. 1991;32(11):2970-2975.
- Sobrin L, Liu Z, Monroy DC, et al. Regulation of MMP-9 activity in human tear fluid and corneal epithelial culture supernatant. Invest Ophthalmol Vis Sci. 2000;41(7):1703-1709.
- Määttä M, Kari O, Tervahartiala T, et al. Tear fluid levels of MMP-8 are elevated in ocular rosacea--treatment effect of oral doxycycline. Graefes Arch Clin Exp Ophthalmol. 2006;244(8):957-962
- Stone DU, Chodosh J. Oral tetracyclines for ocular rosacea: an evidence-based review of the literature. Cornea. 2004;23(1):106-109.
- Afonso AA, Sobrin L, Monroy DC, Selzer M, Lokeshwar B, Pflugfelder SC. Tear fluid gelatinase B activity correlates with IL-1alpha concentration and fluorescein clearance in ocular rosacea. Invest Ophthalmol Vis Sci. 1999;40(11):2506-2512.
- Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007;13(8):975-980.
- Valentín S, Morales A, Sánchez JL, Rivera A. Safety and efficacy of doxycycline in the treatment of rosacea. Clin Cosmet Investig Dermatol. 2009;2:129-140.
- Chamaillard M, Mortemousque B, Boralevi F, et al. Cutaneous and ocular signs of childhood rosacea. Arch Dermatol. 2008;144(2):167-171.
- Kim J-H, Oh YS, Choi EH. Oral azithromycin for treatment of intractable rosacea. J Korean Med Sci. 2011;26(5):694-696.
- Modi S, Harting M, Rosen T. Azithromycin as an alternative rosacea therapy when tetracyclines prove problematic. J Drugs Dermatol. 2008;7(9):898-899.
- Safran AB, Halioua B, Roth A, Saurat J-H. Ocular side effects of oral treatment with retinoids. Retinoids: 10 Years On. 1991;315-326.
- Mantelli F, Di Zazzo A, Sacchetti M, Dianzani C, Lambiase A, Bonini S. Topical azithromycin as a novel treatment for ocular rosacea. Ocul Immunol Inflamm. 2013;21(5):371-377.
- Leyden JJ, Thew M, Kligman AM. Steroid rosacea. Arch Dermatol. 1974;110(4):619-622.
- Murphy CJ, Bentley E, Miller PE, et al. The pharmacologic assessment of a novel lymphocyte function-associated antigen-1 antagonist (SAR 1118) for the treatment of keratoconjunctivitis sicca in dogs. Invest Ophthalmol Vis Sci. 2011;52(6):3174-3180.
- Sun Y, Zhang R, Gadek TR, O’Neill CA, Pearlman E. Corneal inflammation is inhibited by the LFA-1 antagonist, lifitegrast (SAR 1118). J Ocul Pharmacol Ther. 2013;29(4):395-402.
- Zhong M, Gadek TR, Bui M, et al. Discovery and development of potent lfa-1/icam-1 antagonist sar 1118 as an ophthalmic solution for treating dry eye. ACS Med Chem Lett. 2012;3(3):203-206.
- Schechter BA, Katz RS, Friedman LS. Efficacy of topical cyclosporine for the treatment of ocular rosacea. Adv Ther. 2009;26(6):651-659.
- Sakassegawa-Naves FE, Ricci HMM, Moscovici BK, et al. Tacrolimus ointment for refractory posterior blepharitis. Curr Eye Res. 2017;42(11):1440-1444.
- Kapturczak MH, Meier-Kriesche HU, Kaplan B. Pharmacology of calcineurin antagonists. Transplant Proc. 2004;36(2 Suppl):25S-32S.
- Sheppard JD, Singh R, McClellan AJ, et al. Long-term supplementation with n-6 and n-3 pufas improves moderate-to-severe keratoconjunctivitis sicca: a randomized double-blind clinical trial. Cornea. 2013;32(10):1297-1304.
- Pinna A, Piccinini P, Carta F. Effect of oral linoleic and gamma-linolenic acid on meibomian gland dysfunction. Cornea. 2007;26(3):260-264.
- Gumus K, Cavanagh DH. The role of inflammation and antiinflammation therapies in keratoconjunctivitis sicca. Clin Ophthalmol. 2009;3:57-67.
- Macsai MS. The role of omega-3 dietary supplementation in blepharitis and meibomian gland dysfunction (An aos thesis). Trans Am Ophthalmol Soc. 2008;106:336-356.
- Oleñik A, Jiménez-Alfaro I, Alejandre-Alba N, Mahillo-Fernández I. A randomized, double-masked study to evaluate the effect of omega-3 fatty acids supplementation in meibomian gland dysfunction. Clin Interv Aging. 2013;8:1133-1138.
- Epitropoulos AT, Donnenfeld ED, Shah ZA, et al. Effect of oral re-esterified omega-3 nutritional supplementation on dry eyes. Cornea. 2016;35(9):1185-1191.
- Ellis SR, Nguyen M, Vaughn AR, et al. The skin and gut microbiome and its role in common dermatologic conditions. Microorganisms. 2019;7(11):E550.
- Weiss E, Katta R. Diet and rosacea: the role of dietary change in the management of rosacea. Dermatol Pract Concept. 2017;7(4):31-37.
- Dell SJ. Intense pulsed light for evaporative dry eye disease. Clin Ophthalmol. 2017;11:1167-1173.
- Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomed Laser Surg. 2015;33(1):41-46.
- Yuan M, Marmalidou A, Brissette A. Ocular Rosacea: Essentials for Providers. Surface Matters. MillennialEYE website. https://millennialeye.com/articles/2020-nov-dec/ocular-rosacea-essentials-for-providers/. November, 2020. Accessed June 27, 2021.
- Papageorgiou P, Clayton W, Norwood S, Chopra S, Rustin M. Treatment of rosacea with intense pulsed light: significant improvement and long-lasting results. Br J Dermatol. 2008;159(3):628-632.
- Smith K. The photobiological basis of low level laser radiation therapy. Laser Ther. 1991;3:19–24.
- Young S, Bolton P, Dyson M, Harvey W, Diamantopoulos C. Macrophage responsiveness to light therapy. Lasers Surg Med. 1989;9(5):497-505.
- Yin Y, Liu N, Gong L, Song N. Changes in the meibomian gland after exposure to intense pulsed light in meibomian gland dysfunction (Mgd) patients. Curr Eye Res. 2018;43(3):308-313.
- Stevenson W, Chauhan SK, Dana R. Dry eye disease: an immune-mediated ocular surface disorder. Arch Ophthalmol. 2012;130(1):90-100.
- Byun JY, Choi HY, Myung KB, Choi YW. Expression of il-10, tgf-beta(1) and tnf-alpha in cultured keratinocytes (Hacat cells) after ipl treatment or ala-ipl photodynamic treatment. Ann Dermatol. 2009;21(1):12-17.
- Huang J, Luo X, Lu J, et al. IPL irradiation rejuvenates skin collagen via the bidirectional regulation of MMP-1 and TGF-β1 mediated by MAPKs in fibroblasts. Lasers Med Sci. 2011;26(3):381-387.
- De Paiva CS, Volpe EA, Gandhi NB, et al. Disruption of TGF-β signaling improves ocular surface epithelial disease in experimental autoimmune keratoconjunctivitis sicca. PLoS One. 2011;6(12):e29017.
- Lee SY, Park K-H, Choi J-W, et al. A prospective, randomized, placebo-controlled, double-blinded, and split-face clinical study on LED phototherapy for skin rejuvenation: clinical, profilometric, histologic, ultrastructural, and biochemical evaluations and comparison of three different treatment settings. J Photochem Photobiol B. 2007;88(1):51-67.
- Taylor M, Porter R, Gonzalez M. Intense pulsed light may improve inflammatory acne through TNF-α down-regulation. J Cosmet Laser Ther. 2014;16(2):96-103.
- Bäumler W, Vural E, Landthaler M, Muzzi F, Shafirstein G. The effects of intense pulsed light (Ipl) on blood vessels investigated by mathematical modeling. Lasers Surg Med. 2007;39(2):132-139.
- Liu Y, Kam WR, Sullivan DA. Influence of omega 3 and 6 fatty acids on human meibomian gland epithelial cells. Cornea. 2016;35(8):1122-1126.
- Prieto VG, Sadick NS, Lloreta J, Nicholson J, Shea CR. Effects of intense pulsed light on sun-damaged human skin, routine, and ultrastructural analysis. Lasers Surg Med. 2002;30(2):82-85.
- Kirn T. Intense pulsed light eradicates Demodex mites. Skin Allergy News. 2002;33(1):37.
- Lumenis Receives FDA Approval for Its IPL Device to Manage Dry Eye Disease and Launches OptiLight. Eyewire News website. https://eyewire.news/articles/lumenis-receives-fda-approval-for-its-ipl-device-to-manage-dry-eye-disease-and-launches-optilight/. Published April 29, 2021. Accessed June 29, 2021.
- Hutton D. FDA approves IPL device to manage dry eye disease. Ophthalmology Times website. https://www.ophthalmologytimes.com/view/fda-approves-ipl-device-to-manage-dry-eye-disease. Published April 29, 2021. Accessed June 29, 2021.
- Torkildsen GL, Sanfilippo CM, DeCory HH, Gomes PJ. Evaluation of efficacy and safety of brimonidine tartrate ophthalmic solution, 0. 025% for treatment of ocular redness. Curr Eye Res. 2018;43(1):43-51.
- Vaidyanathan S, Williamson P, Clearie K, Khan F, Lipworth B. Fluticasone reverses oxymetazoline-induced tachyphylaxis of response and rebound congestion. Am J Respir Crit Care Med. 2010;182(1):19-24.
- Soparkar CN, Wilhelmus KR, Koch DD, Wallace GW, Jones DB. Acute and chronic conjunctivitis due to over-the-counter ophthalmic decongestants. Arch Ophthalmol. 1997;115(1):34-38.
- McLaurin E, Cavet ME, Gomes PJ, Ciolino JB. Brimonidine ophthalmic solution 0. 025% for reduction of ocular redness: a randomized clinical trial. Optom Vis Sci. 2018;95(3):264-271.
- LUMIFY Redness Reliever Eye Drops. Bausch + Lomb website. https://www.bausch.com/our-products/allergy-redness-relief/lumify-eye-drops. Accessed July 1, 2021.
- Barton K, Monroy DC, Nava A, Pflugfelder SC. Inflammatory cytokines in the tears of patients with ocular rosacea. Ophthalmology. 1997;104(11):1868-1874.
- Liu J, Sheha H, Fu Y, Liang L, Tseng SC. Update on amniotic membrane transplantation. Expert Rev Ophthalmol. 2010;5(5):645-661.
- Efron, N. Is contact lens-induced corneal oedema inflammatory? Aust. J. Optom. 1985;68(5): 167-172.
