Pregnancy is often full of surprises, and each pregnancy has its own unique plethora of challenges. Women and their partners know to expect certain physical and emotional changes, however, many are unaware of how pregnancy can affect the eye and visual system. As optometrists, we are responsible for educating pregnant and planning-to-become-pregnant patients on how pregnancy may affect their eye health. We must also explain how their
eyecare during pregnancy may affect their growing babies.
This article will review the physiologic ocular changes that can occur in pregnancy. We’ll dive into the pregnancy-specific ocular pathophysiology and how to manage ocular disease among this patient demographic. Optometrists must thoroughly understand these changes to better educate and serve our patients during this particularly vulnerable time in their lives.
Physiological changes during pregnancy
Throughout the typical 40 weeks of pregnancy, several hormones are variably released by the mother and placenta. They include progesterone, estrogen, prolactin, and relaxin. Increased levels of these hormones are responsible for the physiological changes that occur in a pregnant woman.
The following sections describe these changes and how they specifically affect the eye and adnexae.
Melasma
Melasma, also known as chloasma, is skin hyperpigmentation most commonly around the eyes and cheeks (as seen in Figure 1) but may also include the forehead, bridge of the nose, and upper lip area.1 Estrogen, progesterone, and melanocyte-stimulating hormone steadily increase during pregnancy and are together responsible for these brown-gray patches, which are colloquially known as the “mask of pregnancy.”
“The increased melanin is found in the dermis and/or epidermis layers of the skin.”
Once hormone levels return to baseline a few months after delivery, the melasma patches typically fade.2-3 However, if the skin pigmentation does not return to normal, several treatments are available to reduce the appearance of these dark spots.
Figure 1 shows a patient with melasma on the forehead and cheeks.
Figure 1: Courtesy of Nistico et al.
Blepharoptosis
Blepharoptosis may affect one or both upper eyelids due to dysfunction of the levator palpebrae superioris muscle and levator aponeurosis. Higher levels of estrogen cause increased water retention in the extracellular space of the muscle and connective tissue, leading to
mechanical ptosis.
5 The ptosis, which is usually unilateral, as seen in Figure 2, typically resolves during the postpartum period.
Figure 2 highlights unilateral blepharoptosis.
Figure 2: Courtesy of Pauly et al.
Dry eye syndrome
Dry eye syndrome, already more common in females than males, is another consequence of pregnancy-related physiological changes in the body. Pregnancy causes downregulation of androgen receptors on the ocular surface. In addition, the effects of androgens on the ocular surface are dampened by elevated estrogen and progesterone.
6 “Prolactin directly causes inflammation and damage to the acinar cells of the lacrimal gland.”
This disrupts the normal production and secretion of proteins, water, and immunoglobulin A (IgA) onto the ocular surface, leading to tear film instability.7 Dehydration due to nausea or vomiting and the medications to treat these symptoms can further exacerbate dry eye symptoms.
Changes in corneal thickness
The cornea itself also undergoes biomechanical changes during pregnancy. Some studies show that increased
corneal thickness and steepened corneal curvature result from increased pregnancy hormones.
8-9 These changes may be accompanied by subclinical corneal edema and a change in the refractive index of the cornea. Differences in keratometry and corneal refractive index are responsible for temporary refractive changes that typically return to baseline several months into the postpartum period.
Keratoconus
While pregnancy is not a risk factor for the development of
keratoconus, it may be associated with the manifestation of keratoconus in women with form fruste corneas and the progression of known keratoconus. It is thought that increased estrogen activates estrogen receptors on the cornea and consequently decreases corneal rigidity.
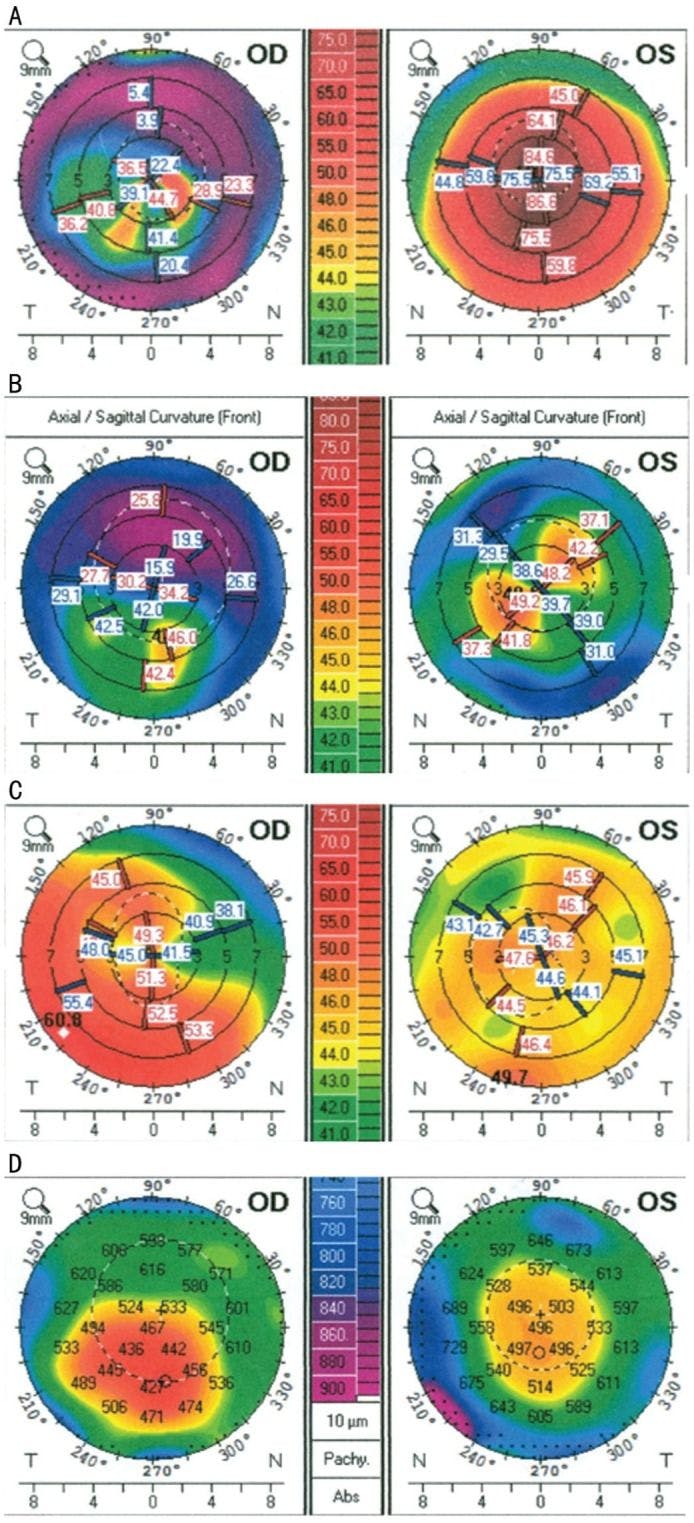
11-12Below, Figure 3 highlights a case in which a woman with keratoconus had bilateral
corneal transplant surgery prior to her pregnancy and then experienced recurrent keratoectasia in the grafts while pregnant several years later.
Figure 3 shows Pentacam anterior corneal curvature maps of a pregnant patient with recurrent keratoectasia; A: OD exhibits irregular astigmatism post-DALK, OS exhibits keratoconus (2013). B: OD exhibits irregular astigmatism in the DALK graft, stable, and OS exhibits regular astigmatism post-penetrating keratoplasty (PK) (2014). C: OD exhibits recurrent ectasia in the DALK graft, and OS exhibits irregular astigmatism in the PK graft (2015, postpartum). D: OD exhibits corneal thinning in recurrent ectasia, and OS exhibits normal corneal thickness (2015, postpartum).13
Figure 3: Courtesy of Gatzioufas et al.
Intraocular pressure
Melasma,
blepharoptosis, dry eye syndrome, refractive changes, and corneal ectasia are considered negative or undesirable physiological ocular changes. However, pregnancy hormones are also responsible for reduced intraocular pressure, which may benefit women with ocular hypertension or glaucoma.
During pregnancy, intraocular pressure is typically reduced by about 10%, along with an overall reduction in diurnal fluctuation.
The reason for this is multifactorial, these include increased uveoscleral aqueous outflow, decreased episcleral venous pressure secondary to increased estrogen and progesterone, and decreased scleral rigidity (specifically within the trabecular meshwork and Schlemm's canal) secondary to the hormone relaxin.10,14,15
Pregnancy-specific conditions
Gestational diabetes mellitus
Gestational diabetes mellitus (GDM) is a subtype of
diabetes that is diagnosed in pregnant women during the 2nd and 3rd trimesters. GDM results from decreased insulin production by pancreatic beta cells, as well as from increased insulin resistance. The pathophysiology is secondary to hormones released by the placenta, specifically lactogen, growth hormone, prolactin, corticotropin-releasing hormone, and progesterone.
“Screening for GDM is recommended between 24 and 28 weeks of pregnancy with a 1-hour oral glucose tolerance test.”
If this is abnormal, then it is confirmed with a 3-hour oral glucose tolerance test. Treatment for GDM is aimed at improving diet and increasing daily exercise to manage hyperglycemia. However, if this is not enough to achieve optimal glycemic control, then insulin treatment is initiated. Metformin and glyburide are sometimes used off-label to treat GDM, but due to side effects to the growing fetus, these oral hypoglycemic agents are not first-line therapies.16-17
Risk factors for GDM
Women with pre-existing type 1 or type 2 diabetes mellitus are at a significantly higher risk of developing
new or worsening diabetic retinopathy when they are pregnant. Disrupted autoregulation of retinal blood vessels in response to increased blood volume is a significant cause of this.
Pregnant women have about a 40% increase in cardiac output and the retinal vasculature does not compensate for this change in blood circulation.
Growth hormone released by the placenta causes increased secretion of insulin-like growth factor, which can promote angiogenesis in the retina. The placenta also influences the upregulation of pro-inflammatory mediators and the downregulation of anti-inflammatory mediators. Longer durations of metabolic disease, how well it is controlled, and the presence of pre-existing diabetic retinopathy prior to pregnancy can all contribute to the risk of new or worsening retinal changes.18
Preeclampsia
Preeclampsia is a
hypertensive disorder occurring only during pregnancy or postpartum. A woman with preeclampsia has a sudden increase in blood pressure. Preeclampsia is considered when a rise in blood pressure >140/90 occurs on two separate occasions at least 4 hours apart or >160/110 on a single occasion.
Preeclampsia is specifically defined as hypertension along with proteinuria or thrombocytopenia, impaired kidney or liver function, pulmonary edema, acute stroke, seizures (properly known as eclampsia), headaches, and/or visual symptoms (aura, photopsia, light sensitivity, scotomas, blurred vision).21
Although it may be obvious, it is absolutely necessary to check blood pressure in the office on any pregnant patient with complaints of a new visual disturbance.
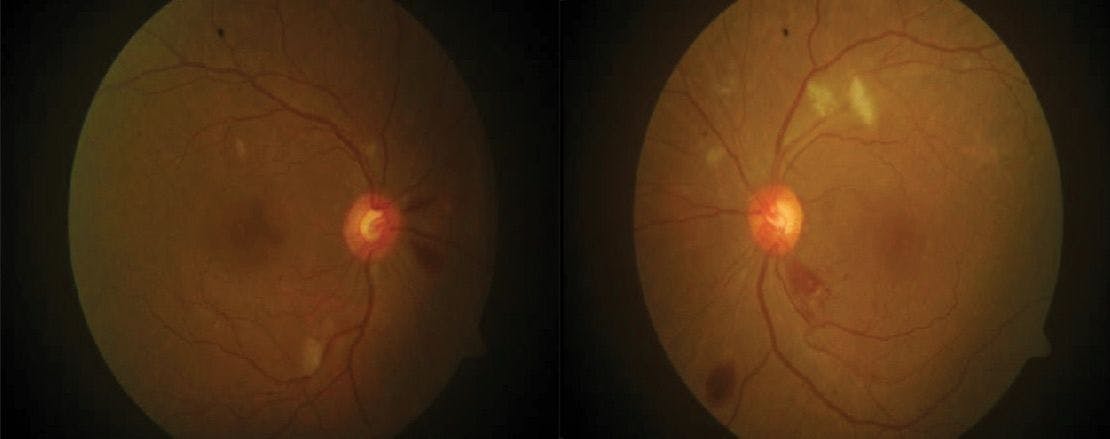
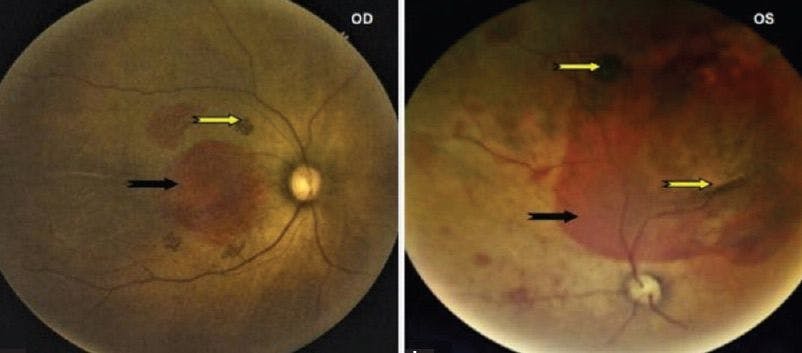
In addition to visual symptoms, women with preeclampsia may also exhibit specific retinal pathology similar to hypertensive retinopathy, like the fundus pictured in Figure 4. The most common sign seen in about 70% of women with preeclampsia is retinal arteriolar spasm. This is described as segmental or generalized constriction/narrowing of retinal arterioles. Other signs include retinal hemorrhages, retinal edema, and cotton wool spots.
Figure 4 features fundus images of a pregnant woman with hypertensive retinopathy secondary to preeclampsia.
Figure 4: Courtesy of Devaru et al.
The link between preeclampsia and retinal detachment
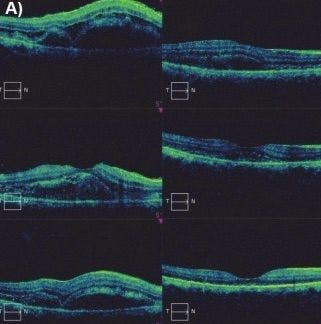
Some women may have serous
retinal detachments that are bilateral and cyst-like. There may also be a retinal vein or artery occlusions and signs of retinal pigment epithelium (RPE) damage. A condition called Purtscher-like retinopathy may also be noted in these women. As the name suggests, this condition has a clinical appearance similar to Purtscher retinopathy secondary to trauma.
Figure 5 highlights macula OCT progression from onset to the resolution of a pregnant woman with serous retinal detachment secondary to preeclampsia.
Figure 5: Courtesy of Dinc et al.
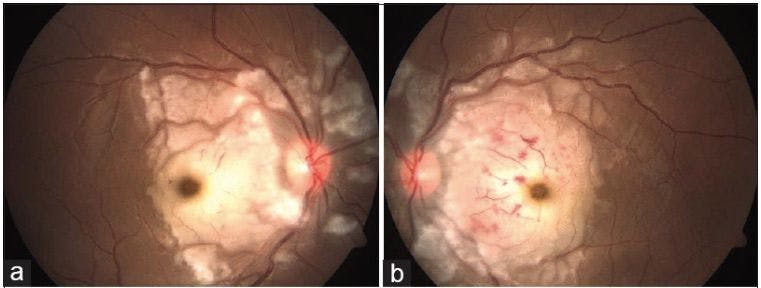
Purtscher retinopathy and Purtscher-like retinopathy are characterized by cotton wool spots, retinal hemorrhages, and Purtscherflecken, which are well-defined white lesions separated by a clear zone from the retinal vasculature. A small percentage (less than 15%) of women may experience transient cortical blindness secondary to preeclampsia-induced posterior reversible encephalopathy syndrome (PRES).20
Figure 6 shows a fundus image illustrating retinal changes that occurred in a pregnant woman with Purtscher-like retinopathy.
Figure 6: Courtesy of Raval et al.
The etiology of preeclampsia is not entirely clear; however, research suggests that abnormal placental implantation is a major part of the pathophysiology.
Downstream effects of preeclampsia include:
- Uterine ischemia and oxidative stress
- Atypical inflammation
- Abnormal angiogenesis and dysregulation of blood vessels
- Damage to the endothelial lining of blood vessels
- The pathological activity of the immune system in response to the above-mentioned vascular abnormalities19-21
A woman is at higher risk for preeclampsia if she is positive for anti-phospholipid antibodies and/or if she had preeclampsia in a previous pregnancy. Moderate risks include pre-existing diabetes, family history of preeclampsia, being pregnant with multiples, or if this is the first pregnancy. There is also a risk for preeclampsia when a woman is over 40 years old during pregnancy or has an elevated body mass index (BMI).19
Risk of reproductive cancer
Pregnancy plays a protective role in certain types of reproductive
cancers. Most specifically, there is a reduced risk of breast, ovarian, and endometrial cancer with a history of pregnancy later on in life. This risk is further reduced with multiple pregnancies and earlier age of first pregnancy.
25-26“When a woman becomes pregnant while she already has cancer, there is a risk that the fetus may be affected by cancer cell transmission through the placenta.”
While this is incredibly rare, the cancer types that are more likely to pass through the placenta include lymphoma, leukemia, and
melanoma (including uveal melanoma).
27 Interestingly to us as optometrists, a woman with a previously known uveal melanoma may be at risk for accelerated growth of the melanoma while pregnant.
Other ophthalmic neoplasms that have reported accelerated growth during pregnancy include optic nerve sheath meningioma, sebaceous carcinoma, and orbital schwannoma. This is thought to be secondary to hormonal changes that may alter the microenvironment around these tumors, along with other changes in immune system reactivity and changes in angiogenesis and blood volume.28
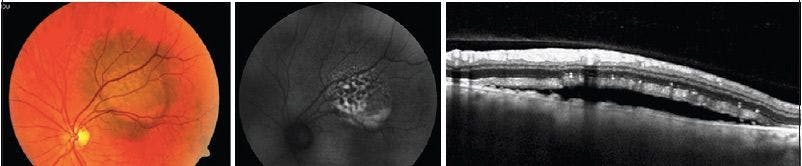
Figure 7 features a fundus image of choroidal melanoma with lipofuscin, fundus autofluorescence image showing hyperautofluorescence, and a macula OCT showing associated serous retinal detachment.
Figure 7: Courtesy of Rishi et al.
TORCH
TORCH is a mnemonic to remember a specific group of diseases that can be transmitted to the child during pregnancy that causes congenital conditions. A mother may pass the disease to her baby while pregnant through the placenta, while giving birth through physical contact in the birth canal, and/or after birth through breast milk.
These infections include toxoplasmosis, syphilis, hepatitis B, rubella, cytomegalovirus, and herpes simplex virus. Human immunodeficiency virus and Zika virus are also sometimes considered part of this group of infections. TORCH infections account for 2 to 3% of all congenital disorders in newborn babies.
Each infection typically shares the following features:
- Jaundice
- Low birth weight
- Microcephaly
- Rashes
- Cardiac problems
- Developmental delays
- Hearing impairment
- Vision impairment
- Vision impairment is likely due to cataracts, chorioretinitis, and microphthalmia31
Figure 8 shows fundus images of a 4-week-old infant with chorioretinitis with a seropositive cytomegalovirus (CMV) infection.
Figure 8: Courtesy of Suganya et al.
Obstetricians routinely educate their pregnant patients on the importance of regular handwashing and hygiene, being up to date on vaccines (specifically rubella), safe sex practices to avoid sexually transmitted infections (syphilis, HSV, HIV), not traveling to countries with a high prevalence of Zika virus, and abstaining from eating undercooked foods and cleaning cat litter boxes (to avoid toxoplasmosis). If a pregnant woman is infected with one of the TORCH infections, then treatment is necessary to reduce the transmission or severity of the disease for their infant baby.31
Pregnant patients' susceptibility to retinal vascular occlusions
Retinal vascular occlusions are rare in women without cardiovascular risk factors, however, pregnancy puts a woman in a hypercoagulable state, and thus she is more susceptible to retinal vein and artery occlusions during pregnancy.
This hypercoaguable state is a physiological adaptation to pregnancy to prevent postpartum hemorrhage. There are increased concentrations of the coagulants fibrinogen and thrombin, and decreased concentration of protein S, an anticoagulant.
In addition, the placenta activates the production of plasminogen activator inhibitor 1, producing plasminogen activator inhibitor 2, which inhibits fibrinolysis and anticoagulation when in high concentrations. Venous stasis may also occur due to other pregnancy-related hormonal changes. As a result of these physiological changes, pregnant women have a four- to five-fold increased risk of thrombosis compared to when not pregnant.32-34
Figure 9 exhibits a fundus image of a 25-week pregnant woman with acute branch retinal artery occlusion.
Figure 9: Courtesy of Stacy Schonberg, OD
Risk factors for retinal vascular occlusions
Central serous chorioretinopathy may occur due to this temporary hypercoagulable state, along with increased vascular permeability and other hormonal changes that affect choroidal vessel hemodynamics and circulating prostaglandin levels. The exudative retinal and/or RPE detachments resolve spontaneously near the end of pregnancy or early in the postpartum period.
35 Pre-existing ophthalmic conditions such as posterior scleritis, thyroid-associated orbitopathy, and symptoms of pituitary adenomas may worsen during pregnancy.
It is interesting to note that uveitis secondary to Vogt-Koyanagi-Harada (VKH) disease, sarcoidosis, rheumatoid arthritis, and other spondyloarthropathies may improve or go into remission during pregnancy.35
Pharmaceutical considerations in pregnancy
The last section of this article will discuss topical and systemic ophthalmic medications that are safe and those to avoid during pregnancy.
1. Mydriatic use during pregnancy
Tropicamide and cyclopentolate are the mydriatics that are safe to use when a dilated fundus exam is required, such as when a
retinal tear or detachment is suspected or when diabetic or hypertensive retinopathy is a concern.
2. Parasympatholytic use during pregnancy
Longer-acting parasympatholytics such as homatropine, scopolamine, and atropine should be avoided, along with the sympathomimetic phenylephrine, unless absolutely necessary to get a wider view of the peripheral retina.
3. Topical steroid use during pregnancy
Topical steroids such as prednisolone acetate and loteprednol etabonate can be used to treat ocular inflammation from corneal infiltrates and uveitis, but the prescribing optometrist should discuss this with the patient’s obstetrician to keep them aware.
“Oral steroids are typically contraindicated during pregnancy.”
When a topical antibiotic is necessary, the optometrist can choose topical tobramycin, azithromycin, polymixin B, and erythromycin. Topical fluoroquinolones have not been well studied in pregnancy but may be necessary for treating a
bacterial corneal ulcer in which the benefits outweigh the potential risks. A fortified cephalosporin such as cefazolin or ceftazidime is also a great choice for additional coverage of a bacterial corneal ulcer.
364. Anti-viral use during pregnancy
Oral acyclovir, valacyclovir, and famciclovir are safe to use during pregnancy as these antivirals are routinely prescribed for herpes simplex prophylaxis. Similar to a patient who is not pregnant, herpes simplex epithelial keratitis can be treated successfully with an oral antiviral. Optometrists do not need to consider the use of topical trifluridine or ganciclovir, which are contraindicated in pregnancy.36
5. Dry eye disease treatments during pregnancy
Ocular surface disease is common in pregnant women due to physiological changes in the tear film and corneal sensitivity. Dry eye syndrome should be treated conservatively with lid hygiene and artificial tears.
“Cyclosporine and Xiidra lifitegrast are contraindicated in pregnancy.”
Acute or chronic allergic conjunctivitis can be managed safely with topical alcaftadine, cool compresses, and artificial tears. However, olopatadine and bepotastine should be avoided when managing
allergic conjunctivitis.
366. Glaucoma medications during pregnancy
Glaucoma is uncommon in this patient demographic; however, optometrists do treat glaucoma and ocular hypertension in women who may become pregnant. As previously discussed, hormonal changes in pregnancy increase aqueous outflow and reduce episcleral venous pressure, together causing reduced intraocular pressure.
10,14-15 If a woman requires ocular hypotensive treatment during her pregnancy (instead of active surveillance), topical brimonidine can be prescribed safely.
Topical beta-blockers and prostaglandin analogs are contraindicated, along with topical and oral carbonic anhydrase inhibitors. Alternatively, an optometrist may consider
selective laser trabeculoplasty if medicating is not an option due to a known allergy or other contraindication.
36Conclusion
Pregnancy disrupts a woman’s internal homeostasis to allow for the growth and development of her baby. This article explored some of the effects of this via anatomical and physiological changes to the eyes, visual system, and body.
“As discussed, there are numerous safe options for pharmaceutical management of ophthalmic conditions during pregnancy.”
If a patient requires prescription medication for an ophthalmic condition, it may still be a good idea to consult with the obstetrician to ensure that there are no specific contraindications. By
co-managing these patients, the optometrist can ensure that any necessary medication or treatment is safe for both the patient and the baby.
Providing quality eyecare for pregnant patients benefits the patient and is an excellent way to collaborate with other medical providers in the community while also building your practice.