


Dry eye disease and ocular allergy are two of the most common ocular surface conditions eyecare providers (ECPs) encounter, affecting an estimated 5 to 15% and 40% of the US population, respectively.1-4
Dry eye and ocular allergies can share many of the same clinical signs and symptoms, making the task of delineating the two conditions a potential challenge.5 Complicating things even further is the fact that it is not uncommon for a patient to display signs and symptoms of each condition concurrently, as an estimated 31 to 36% of patients with allergic conjunctivitis also have dry eye.6
Not only are dry eye and ocular allergies extremely common, but they even share seasonal patterns, with both tending to flare during the spring months.7,8 Fortunately, there are a few tell-tale signs and tests that make distinguishing dry eye and ocular allergies relatively straightforward.
The allergic conjunctivitis story
Classic allergic conjunctivitis (AC) typically presents in two ways: acute/seasonal allergic conjunctivitis and chronic/perennial allergic conjunctivitis. Both forms are Type I hypersensitivity reactions that result in itching, a papillary conjunctival reaction, and stringy/ropey discharge.
However, as their names indicate, seasonal allergic conjunctivitis (SAC) tends to be associated with seasonal allergens, such as pollen, whereas perennial allergic conjunctivitis (PAC) persists throughout the year, as it is caused by routinely present allergens like pet dander, dust mites, and mold.9-18
Although they share the same signs and symptoms, PAC tends to have a milder presentation than SAC.12 However, dry eye and allergic conjunctivitis in each form can result in red, itchy, and watery eyes.9-21 Additionally, lid edema and chemosis are possible in both as well, sometimes making clinical diagnosis challenging.9-12,14,16,17,22-25
When allergies meet dry eye
There are several hallmark signs unique to allergic conjunctivitis that set it apart from classic dry eye. Although ocular itching is the primary symptom associated with allergic conjunctivitis, the nature of the itching experienced by the patient can help determine the underlying cause.
If the itching improves with eye rubbing, then it is likely due to dry eye, whereas if the itching worsens with rubbing, then it is likely associated with allergies.26-29 The reason for this is that mechanical rubbing can stimulate the production of reflex tears, which can improve the itching caused by dry eye, but this same mechanical stimulation can cause further degranulation of histamine from mast cells, which only serves to exacerbate allergic pruritus.26-29
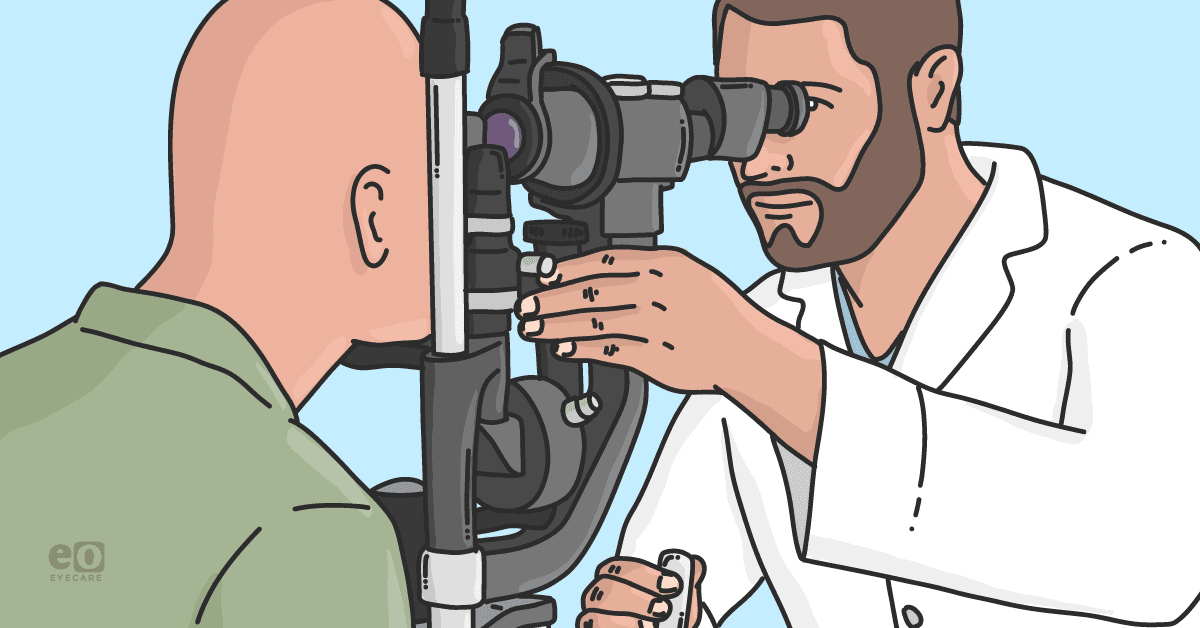
Other signs that point to the presence of allergy rather than dry eye are stringy or ropey discharge along with the presence of conjunctival papillae, as displayed in Figures 1 and 2, respectively.9-21 These whitish strands, which can often be found balled up at the nasal canthus coupled with a papillary reaction are classic signs of allergic conjunctivitis that are not typically associated with dry eye.
Figure 1 is a clinical image of a patient with stringy/ropey discharge caused by allergic conjunctivitis.

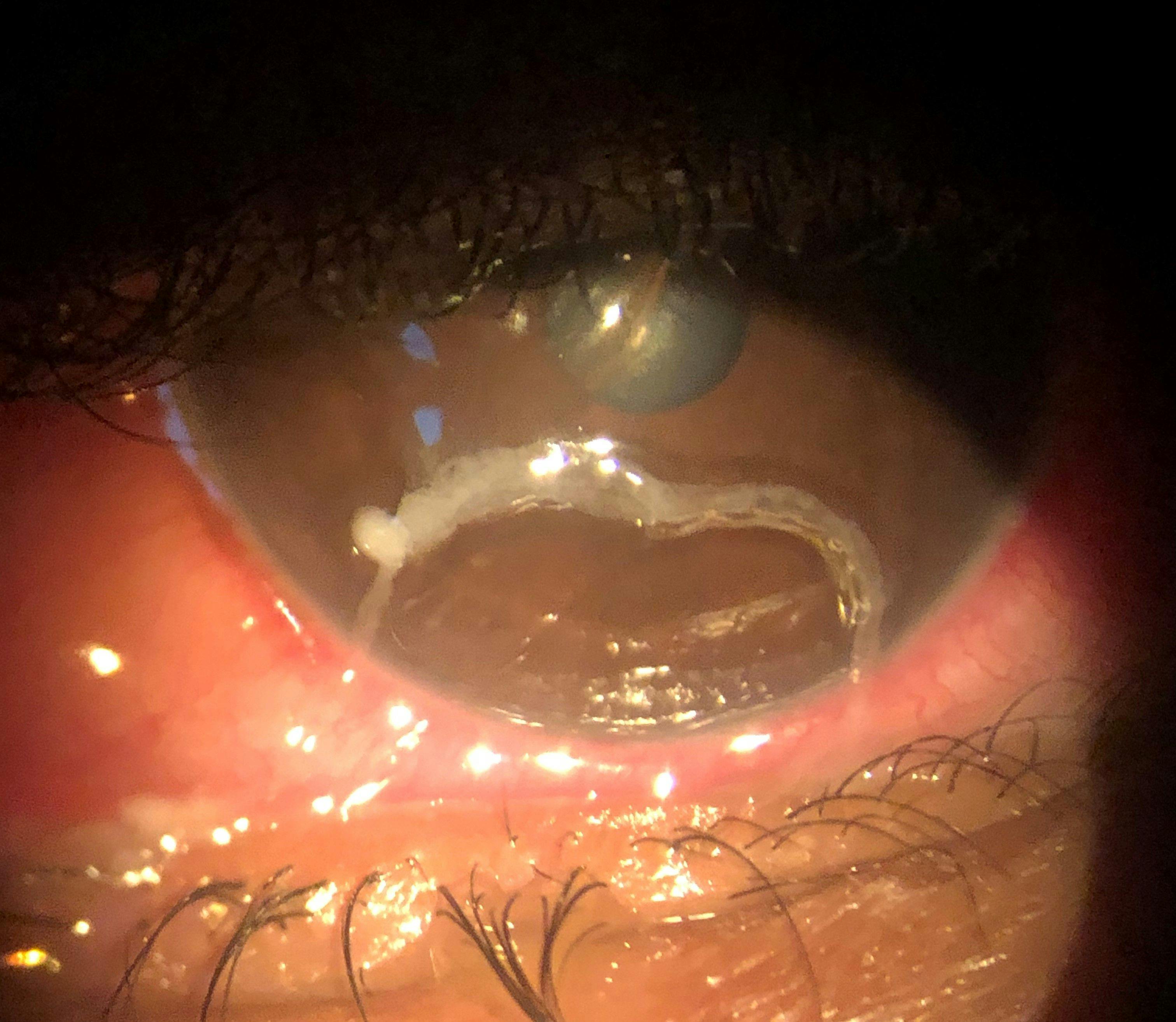
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO.
Further considerations for discerning between dry eye and ocular allergies
That being said, this delineation is not always straightforward. It is not unusual for a patient to present with both dry eye and ocular allergies, so they are not mutually exclusive.5 Additionally, in some cases of dry eye, especially more advanced cases, patients can illustrate mucoid-tears due to increased mucus production as a compensatory mechanism and papillae can develop if excess mechanical friction from dryness occurs.30
However, the mucus associated with dry eye does not tend to form rope-like strands like those that develop in allergic conjunctivitis, but more of a thin, thread-like strand that is typically adherent to the cornea rather than free moving.31 Further, a papillary reaction is much more common in AC than dry eye.
But if you are still in doubt, or wondering if a dry eye patient who demonstrates itching has an allergic component to their ocular surface disease, there is a simple in-office test that can help quickly identify the presence of an allergic element.
In cases where I suspect an allergic component but the signs and symptoms are not definitive, I will instill one drop of an antihistamine-mast cell stabilizer (AH-MCS) combination drop, such as Pataday Once Daily Relief Extra Strength (olopatadine hydrochloride ophthalmic solution 0.7%, Alcon), and wait about 1 minute.
If the itching improves after drop instillation, then this points to the presence of a classic allergic process, as histamine is the source of itching present in allergies. If the itching persists then the origin of the itching is likely due to some other ocular surface condition.
Figure 2 features conjunctival papillae caused by allergic conjunctivitis.

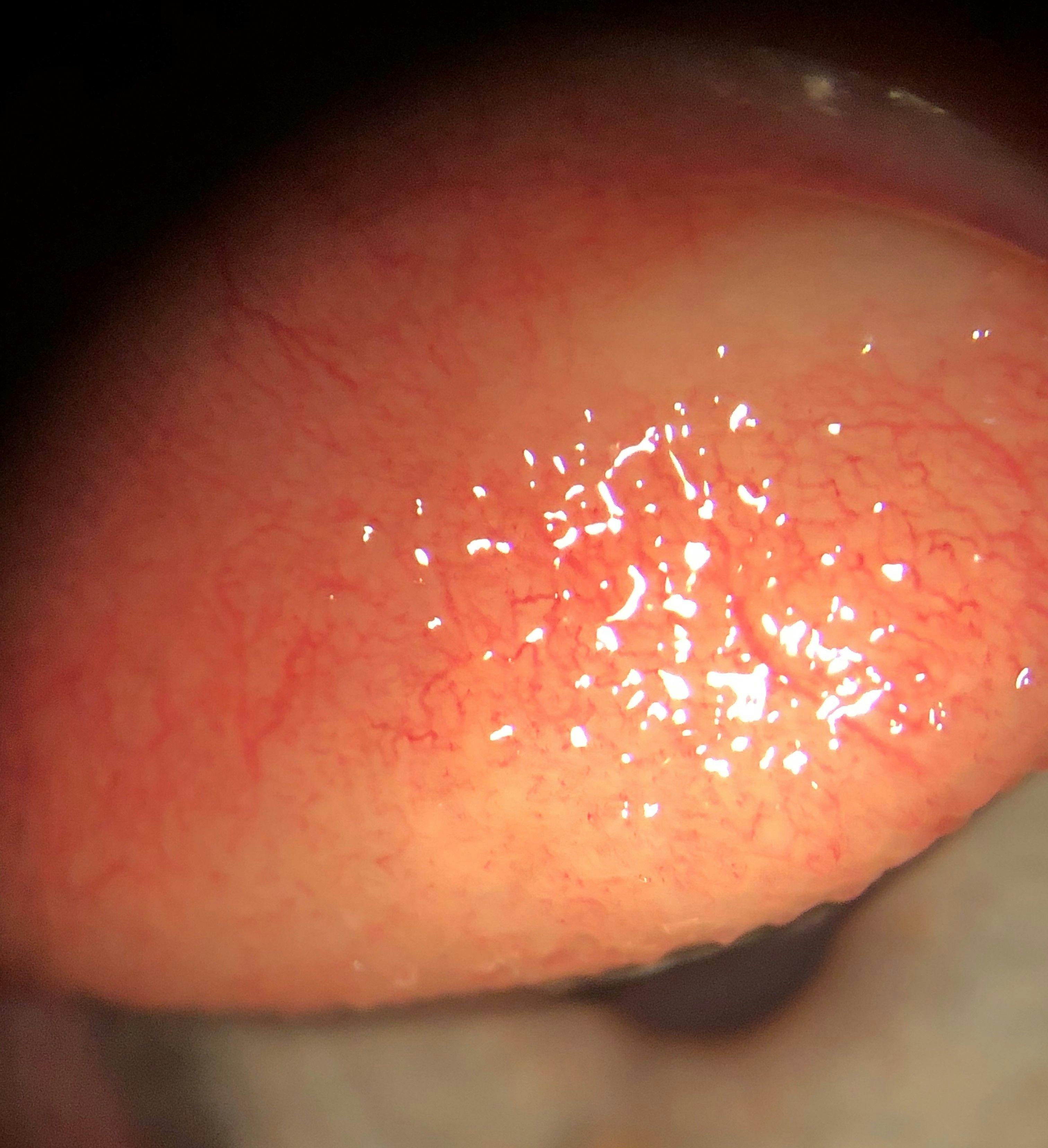
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO.
The masqueraders part 1: Demodex
Dry eye is not the only ocular surface condition that can present similarly to allergic conjunctivitis. For instance, the most common symptom associated with Demodex blepharitis is ocular itching.32 Likewise, Demodex blepharitis can also cause redness and chemosis.32,33 Fortunately, once again, there is an easy way to identify the culprit.
The presence of cylindrical, sleeve-like build-ups at the base of the lashes, as shown in Figure 3, is indicative of collarettes, which are pathognomonic for Demodex blepharitis.34,35 Therefore, if a patient experiences symptoms of ocular itching in the presence of collarettes, Demodex blepharitis should be considered as a potential cause.
Likewise, if a patient has signs and symptoms of allergic conjunctivitis, but itching persists even with traditional allergic conjunctivitis treatments, including mast-cell stabilizer-antihistamine combos or even topical corticosteroids, then looking for the presence of collarettes could help identify Demodex as the cause of the persistent symptoms.
Currently, Demodex blepharitis is routinely treated with a topical tea tree oil cleanser or an okra-based cleanser, such as Zocular. However, we now have the first FDA-approved treatment indicated for Demodex blepharitis in the form of XDEMVY (lotilaner ophthalmic solution 0.25%, Tarsus Pharmaceuticals), which has demonstrated a significant eyelid health improvement in the form of mite eradication and erythema reduction.36-38
Figure 3 depicts collarettes on a patient’s lid margin, caused by Demodex blepharitis.


Figure 3: Courtesy of Cory Lappin, OD, MS, FAAO.
The masqueraders part 2: MFS, FK, and GCP
There are a few other conditions worth mentioning in the dry eye versus allergy discussion are mucus fishing syndrome (MFS), filamentary keratitis (FK), and giant papillary conjunctivitis (GCP).
Mucus fishing syndrome
Mucus fishing syndrome starts out with ocular surface irritation, usually in the form of foreign body sensation related to dry eye, which results in the patient frequently rubbing and “digging” at their eyes.39,40
This behavior actually results in further friction and mechanical irritation, to which the ocular surface responds by producing mucus to reduce this friction. However, this mucus itself can cause irritation, which causes the patient to repeat their “fishing” behavior to remove the mucus, resulting in a vicious cycle.39,40
Itching is also common in MFS, as is a papillary reaction, so this condition can easily mimic allergic conjunctivitis, and allergic conjunctivitis itself can lead to MFS. Therefore, it is crucial to ask patients about “fishing” behavior to help diagnose this condition. Fortunately, the treatment for MFS is similar to the treatments for both dry eye and allergic conjunctivitis, including a topical AH-MCS, artificial tears, compounded 10% n-acetylcysteine (NAC), and a short course of topical steroids.39-41
Filamentary keratitis
Filamentary keratitis is also commonly associated with dry eye disease.42 It is thought to result from mechanical friction between the corneal surface and the palpebral conjunctiva. As the lids blink over the corneal surface, degenerated epithelial cells form strand-like structures that cause further friction and irritation.
To reduce this friction and irritation, the eye produces mucus to coat these epithelial strands, resulting in a degenerated epithelial cell core-mucus coat complex that forms the stringy strands we refer to as filaments, as shown in Figure 4.
The difference between the mucus strands produced in FK and those in allergic conjunctivitis, is that the strands present in FK will be attached to the cornea, whereas those in allergic conjunctivitis are typically mobile. There are numerous treatments for FK, including topical steroids, bandage contact lenses, autologous serum, and compounded 10% n-acetylcysteine, in addition to supportive dry eye therapies.42
Figure 4 highlights filaments caused by degeneration of the epithelial cell core-mucus coat complex, as seen in filamentary keratitis.

Figure 4: Courtesy of Cory Lappin, OD, MS, FAAO.
Giant papillary conjunctivitis
Giant papillary conjunctivitis is characterized by its namesake giant papillae that typically appear on the superior palpebral conjunctiva. Additionally, GPC can elicit a foreign body sensation, redness, and produces a stringy or ropey discharge. While this presentation is suggestive of allergic conjunctivitis, it lacks the classic itching that is associated with classic allergic conjunctivitis.43-45
This is because is not an allergic reaction, but rather caused by chronic mechanical irritation due to friction between deposits on the surface of a contact lenses or the lens edge and the superior palpebral conjunctiva with each blink.43-45 Therefore, if a patient displays an allergic conjunctivitis-like reaction with large papillae (up to 1mm in diameter like those found in Figure 5) in the presence of contact lens wear, but lacks itching, then the condition is likely GPC rather than allergic conjunctivitis.
GPC is managed with topical corticosteroids dosed for 1 to 2 weeks, or tapered over several weeks for more severe cases, during which the patients should discontinue contact lens wear. Once the condition has resolved, the patient should be refit into a contact lens of a different brand, material, or wear schedule. Ideally, daily disposables, as they are less likely to accumulate surface deposits and material degradation associated with repeated wear.43
Figure 5 shows large papillae and an allergic conjunctivitis-like reaction in a patient with GPC.


Figure 5: Courtesy of Cory Lappin, OD, MS, FAAO.
Clinical presentations of atopic conditions
When managing ocular surface disease, it is also vital to be on the lookout for vernal keratoconjunctivitis (VKC) and atopic keratoconjunctivitis (AKC), which are atopic forms of allergic conjunctivitis caused by Type I and IV hypersensitivity reactions.46-48 Both conditions are associated with intense ocular itching and significant inflammation.9,47-51
Vernal keratoconjunctivitis
VKC has a seasonal presentation, being more pronounced in the spring months, and also is more common in warmer climates, tending to affect pediatric patients, which typically self-resolves as the patient ages.9,7,46,47,52
Other signs that differentiate VKC from classic allergic conjunctivitis are giant papillae that are referred to as cobblestones, as shown in Figure 6, which are typically present on the superior palpebral conjunctiva along with whitish raised lesions at the limbus referred to as Trantas dots noted in Figure 7. In rare cases, corneal ulcers, known as “shield ulcers,” can result from chronic inflammation and friction.9,46,47,49,52,53
Figure 6 is a clinical image of giant papillae (cobblestones) caused by vernal keratoconjunctivitis.

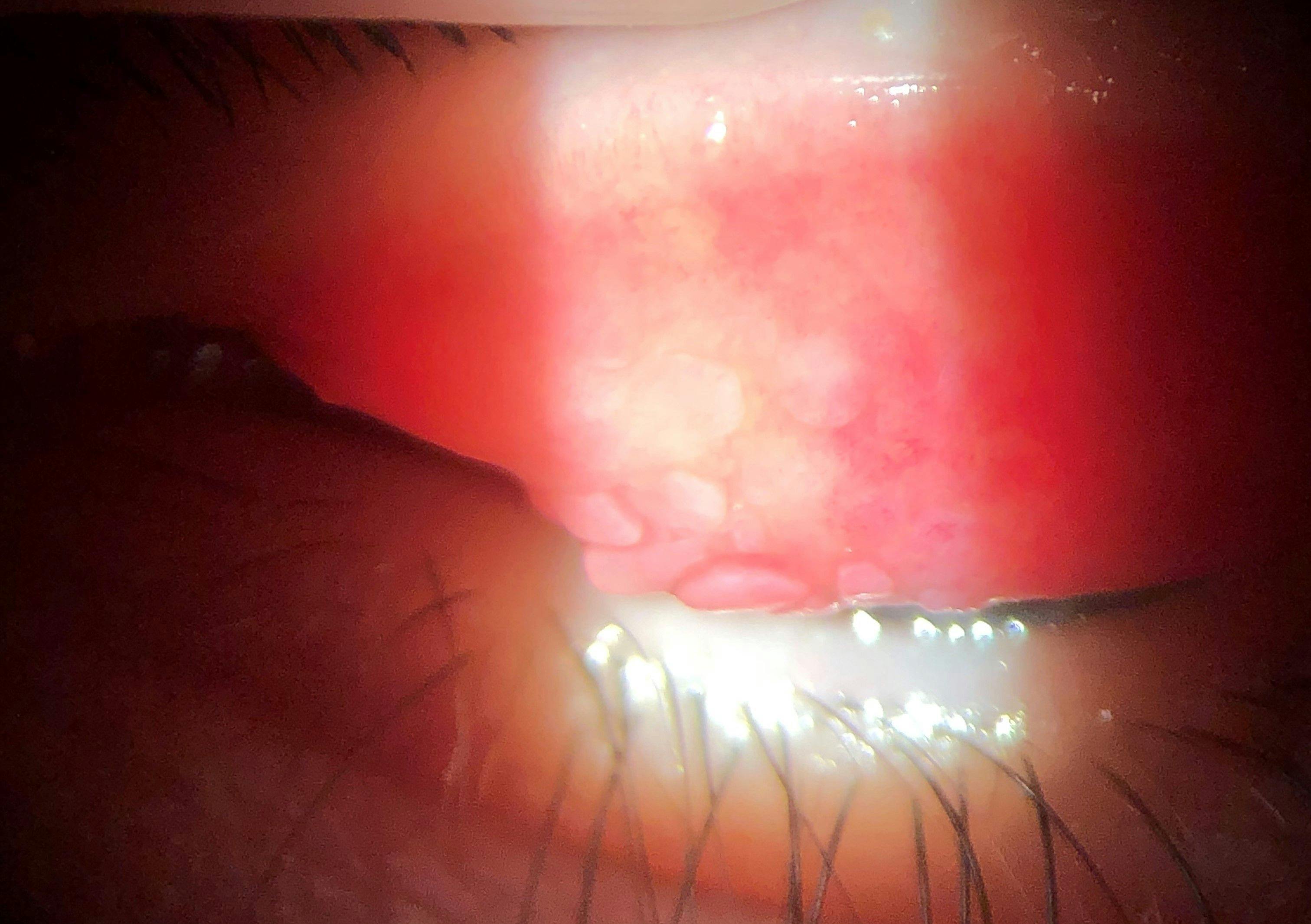
Figure 6: Courtesy of Cory Lappin, OD, MS, FAAO.
Figure 7 shows a patient with whitish raised lesions at the limbus, called Trantas dots, caused by VKC.

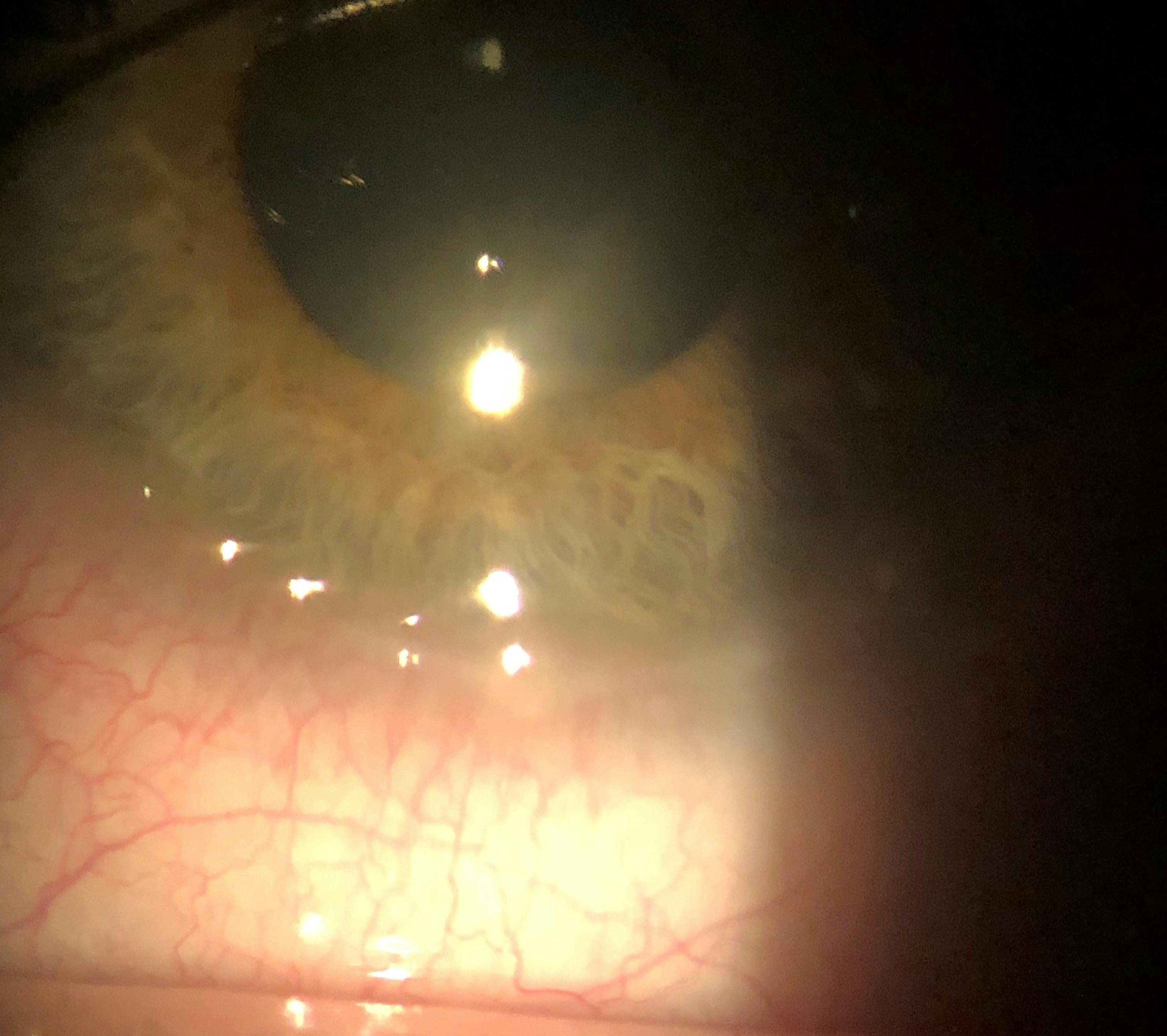
Figure 7: Courtesy of Cory Lappin, OD, MS, FAAO.
Atopic keratoconjunctivitis
Atopic keratoconjunctivitis also displays severe itching, significant inflammation, and giant papillae (typically on the inferior palpebral conjunctiva); however, unlike VKC, AKC tends to affect the eyelids and lid skin directly in the form of edema and dryness and flaking of the skin, whereas VKC tends to spare the lids.48,50,51,54 Further, AKC tends to be associated with eczema and asthma and has no seasonal pattern affecting the teenage to middle-aged adult population rather than children.9,50,51,54,55
In both cases, controlling inflammation is a key pillar of the treatment strategy. These patients often require the use of topical corticosteroids, as well as a topical immunomodulator, such as Verkazia (cyclosporine ophthalmic emulsion 0.1%, Harrow), which is FDA-approved for the treatment of VKC to manage long-term inflammation, in addition to a topical AH-MCS.47,54
Managing dry eye and ocular allergy
Once you have determined whether your patient is experiencing dry eye, allergies, or both, the next—and most important step—is determining how to manage it.
As we all know, dry eye is multifactorial, and each contributory component should be addressed to fully treat the condition. This same philosophy extends to ocular surface disease in general, including ocular allergy.
Treating allergic conjunctivitis
The standard first-line treatment for allergic conjunctivitis is a topical AH-MCS, as this blocks histamine from binding and causing itching while reducing the ability of allergens to bind to mast cells, allowing for the prevention of further degranulation of histamine.9,15,16,56,57 This dual mechanism can provide rapid relief from symptoms of ocular allergy while also extending prolonged protection against their recurrence bundled with a favorable safety profile for long-term use.16
Some commonly used AH-MCS drops are Pataday Once Daily Relief Extra Strength, Lastacaft (alcaftadine ophthalmic solution 0.25%, Allergan, an AbbVie Company), and Alaway (ketotifen fumarate ophthalmic solution 0.035%, Bausch + Lomb), with the latter commercially available in a preservative-free formulation. Topical steroids may also be implemented if there is a significant inflammatory component.15,16
Treating atopic allergies
In cases of atopic allergies such as VKC and AKC, a topical immunomodulator is oftentimes needed to manage the chronic inflammation associated with these conditions. For patients experiencing significant itching of, and disruption to, the eyelids skin itself, topical tacrolimus ointment can be used off-label to manage this inflammation and irritation,54 which can help spare the side effects associated with steroid ointments including skin depigmentation and thinning.58
It might be recommended to have these patients undergo a hepatic function panel to evaluate liver chemistry prior to administering tacrolimus.
New therapies available to EPCs to treat ocular allergies
In addition to these traditional treatments, a new treatment option has become available and is already proving to be one of my go-to treatments for allergic conjunctivitis, especially in patients suffering from both dry eye and ocular allergies.
Optase Allegro (SCOPE) is a preservative-free drop that contains hydroxyethyl cellulose (HEC) as its active ingredient and 2% ectoin as an inactive ingredient. While the HEC component helps soothe symptoms of dry eye, it is the inclusion of ectoin that makes this drop unique. Ectoin is an extremolyte, an organic compound naturally produced by extremophiles which are microorganisms that live in extreme environments, such as those with high heat or acidity.59,60
Ectoin has a strong affinity for water molecules, and pulls them closely to itself, which creates a barrier or “water shield,” leading to a mechanism of action referred to as preferential exclusion.59 When placed on the ocular surface, ectoin pulls water molecules close, creating a “water shield” that acts as a barrier that can prevent allergens from binding to the ocular surface and eliciting an allergic reaction.59 Like an AH-MCS, Allegro has a rapid onset, with relief experienced in as little as 30 seconds.61
While Allegro can be used as a standalone treatment, as it can help alleviate symptoms of both dry eye and ocular allergies, I have been routinely using it as an adjunct to traditional topical AH-MCS. This past allergy season was a particularly brutal one for the Southwest US, and many of my patients whose allergies were typically well-controlled with an AH-MCS were experiencing “breakthrough” allergies, requiring them to use their drops two to three times per day rather than their typical once-daily dosing.
I started having these patients use a combination of an AH-MCS in the morning and Allegro in the afternoon. These patients saw excellent results, as they were able to address their allergies from multiple different mechanisms of action due to the MCS, AH, and physical barrier component of ectoin.
Summary
Dry eye and ocular allergies are two common ocular surface conditions that present similarly and often together.
Determining the presence of a true allergic component will help determine the necessary treatment and help address each underlying cause of the ocular surface disruption.
