




Our understanding of dry eye disease (DED) has changed dramatically in the last decade. There is now a consensus that inflammation (not just a lack of tears) is a root cause of the disease.1 There have been huge leaps in technology in both diagnostic and therapeutic ways to manage DED, but the truth is that most dry eye patients still remain untreated. Effective therapy doesn't always need to cost thousands of dollars to work, but tailored solutions in concert with proper patient education is key.
Let’s walk through a dry eye cheat sheet from low tech to the cutting edge.
Where to start?
A good dry eye questionnaire is a perfect way to start the conversation with your patients. These surveys provide invaluable information about frequency and severity of symptoms at minimal cost. A proper comprehensive eye examination to rule out systemic disease contributing to dryness is also important. However, having some specialized dry eye diagnostic equipment is critical for the patient to “buy into” in-office therapy.
It can be as easy as using your cell phone to take pictures of the lids or repurposing an existing slit lamp camera. Staining to highlight dry eyes (fluorescein or lissamine) and showing these pictures to your patients is low cost yet impactful. Meibography can be done simply by using a penlight or red light in the absence of dedicated technology.
Advanced meibography options range from Meibox to Lipiscan and Oculus 5K (which integrates non-invasive TBUT and various advanced dry eye features along with topography). Tear osmolarity is a quantitative analysis of DED and several options exist to measure this important marker, including Tearlab and Ipen.
Economical options for treating DED
In-office dry eye treatment begins with heating of the eyelids (despite the patient's best effort, at-home hot compresses are oftentimes simply not enough without in-office treatments to complement it). Heating the meibomian glands allows for easier expression and removal of debris from the lashes.
Some low-cost options include TheraPearl or the Bruder mask. There is also TearRestore, which does not require a microwave and doesn't obstruct vision. Patients can also bring their own heating mask to professional treatments (or purchase one in the office). can also bring their own heating mask to professional treatments (or purchase one in the office). For time efficiency, staff can prepare the heating device for the patient and have them treated in the waiting room (or dedicated area). Manual expression of the meibomian glands can then be performed.
Doing the procedure at the slit lamp gives a more magnified view and allows a more complete diagnostic assessment of the quality of the meibum. In some cases, it may be easier outside the slit lamp and loupes can be employed if needed. Collins forceps and Mastroda paddle are two preferred instruments. This procedure is comparable to pimple popping and the discomfort experienced is usually similar (momentary and tolerable). Anesthesia with alcaine or equivalent can be used if patients are sensitive, although there is an argument to be made for withholding the numbing drops to get more accurate patient feedback.
Lid debridement: Low cost, high impact
Debridement of the lid margin is another low tech, low cost procedure that can make a big difference for Meibomian Gland Dysfunction (MGD) patients. Vital stains can be employed to highlight the Line of Marx (LOM) and clean off debris and biofilm formations. While a golf spud can be adequate, the Karpecki debrider is an excellent tool specifically designed for the task.
For removal of deposits on the lashes, Zocular ZEST is a fantastic disposable option based on natural ingredients (okra) which kill demodex. Another solution with some upfront costs is BlephEx (Alcon) or AB Max (Myco Industries). Mechanized units may be more effective for heavier deposits while ZEST (Zocular) can provide gentler pressure (as it’s performed manually).
In this video, Dr. Eltis performs meibomian gland expression, lid debridement, and ZEST.
View this post on Instagram
Figure 1 illustrates a patient suffering from demodex blepharitis.

Figure 1: photo credit Mark Eltis.
Figure 2 demonstrates a patient following Zocular ZEST cleaning.

Figure 2: photo credit Mark Eltis.
Advanced techniques for DED management
Advanced techniques are rarely used in isolation but rather are employed in concert with the aforementioned lower-cost procedures.
For patients with MGD related to rosacea, we recommend adding intense pulsed light (IPL) therapy as soon as the patient allows. IPL is a powerful tool that can help reduce inflammation and improve the health of meibomian glands over time by using light energy to destroy abnormal telangiectatic blood vessels.2 Patients also enjoy the added benefit of improvement in facial rosacea and skin texture. Multiple sessions are needed to see results and are often scheduled 2-4 weeks apart. Treatments are limited to Fitzpatrick skin types I-V. The OptiLight (Lumenis) recently received FDA approval for the treatment of MGD, making this the only on-label treatment option.
Other IPL brands include Lumecca (InMode), Icon (Cynosure), and E>Eye (ESW Vision). Incorporating lid debridement and meibomian gland expression following IPL treatment is also beneficial to improve meibomian gland function. If there is significant meibum stasis, the patient may also be scheduled for an in-office thermal pulsation treatment.
In this video, Dr. Madan performs IPL treatment.
View this post on Instagram
Intense pulsed light to thermal pulsation
Having IPL and thermal pulsation treatments gives patients a “kick start” to managing their DED which can then be maintained with at-home treatments.
Thermal pulsation options include Lipiflow (Johnson and Johnson) and iLux (Alcon). Both systems produce comparable results however, the operator can view the meibum being expressed when using the iLux system which is helpful in assessing the meibum quality.3,4 Gland expressions done by thermal pulsation systems may provide sustained results for up to 12 months5 and may be more gentle and effective when compared to manual expression.2,3 In-office heating devices can be more effective than at-home products that do not reach the necessary temperature to melt the meibum and cool off too quickly.5 Patients need to be closely monitored to see if repeat treatments are needed.
Unlike Lipiflow or iLux, TearCare (TearCare) uses heat exclusively (without pressure) to liquify meibomian gland contents which are then expressed using a provided handheld device.5 Heating with TearCare does not obstruct natural blinking and has shown a decrease in dry eye symptom scores following treatment.5 Another option is Meiboflow (Mibo Medical) which has a reusable silver tip but does require a staff member/doctor to manually oversee the heating process.
What about radio frequency and LLT?
Another in-office technology that can be employed for MGD treatment is radiofrequency (RF). Radiofrequency uses radio wave energy to heat the treatment area. This procedure can help soften the meibum in the meibomian glands and allow for effective meibomian gland expression.6 RF is also heavily used in the dermatology space for its ability to improve skin laxity. Therefore, it’s a useful tool for patients who need improvement in lid apposition and patients looking to enhance cosmesis.
The three common systems available are TempSure Envi (Cynosure), Forma-I (InMode), and EndyMed (Clarion Medical). A typical treatment takes about 10-20 minutes and repeat treatments are needed to maintain results.
A less involved therapy is Low-Level Light Therapy (LLLT). It brings about photobiomodulation through light-emitting diodes (LEDs) of specific wavelengths.7 This process targets the inflammation which causes MGD. Available brands include Equinox (Marco) and Eye-Light (Topcon), which are capable of IPL treatments as well.
Meibomian gland intraductal probing is another procedure that can be employed to clear obstructions and scar tissue. However, this treatment is more costly and invasive than other manual procedures.
Regenerative medicine to the rescue
Today’s eyecare providers can also consider adding amniotic membranes to their in-clinic treatment options. Amniotic membranes can be especially helpful in patients with moderate to severe dry eye disease. They can also be beneficial in recurrent corneal erosions and neurotrophic keratitis. There are several options available from cryopreserved to dehydrated membranes.
These products have minimal upfront fees (as they can be ordered and delivered rapidly on demand). Cryopreserved membranes are significantly more costly than dehydrated ones but some find them easier to work with. While cryopreserved membranes may produce better results, patients can report discomfort with them. This can be alleviated with a modified tape tarsorrhaphy.
Another option for treating advanced DED is utilizing autologous blood-derived eye drops, such as platelet rich plasma (PRP). PRP contains essential growth factors, vitamins, and cytokines, which can help heal corneal epitheliopathy (Figure 3). ODs can provide in-house PRP services (depending on their jurisdiction) or work with compounding pharmacies and local labs to make the blood-derived drops available to patients.
Figure 3 shows the before and after use of platelet rich plasma (PRP) to help heal recalcitrant dry eye.

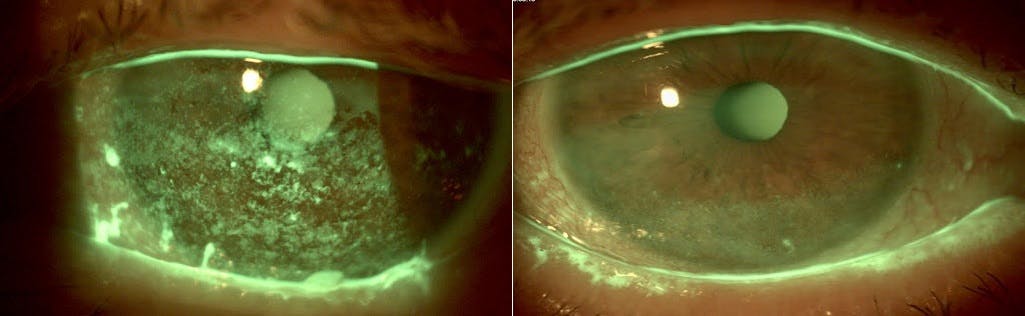
Figure 3: photo credit Mahnia Madan
There are many different kinds of artificial tears on the market for mild to severe dry eye. Laura Goldberg, OD/MS discusses the different types of artificial tears and shares her insights with a comparative list of the artificial tears on the market with a handy download. Click here to view the list.
How it all fits
At-home care combined with in-office treatments leads to much better results for patients than either one alone. Managing dry eye disease does not always need to be expensive and expensive doesn’t always mean superior. An individualized approach allows optometrists to not only offer exceptional care but to also differentiate themselves in a competitive field.
References
- Tsubota K, Pflugfelder SC, Liu Z, et al. Defining Dry Eye from a Clinical Perspective. Int J Mol Sci. 2020;21(23):9271. Published 2020 Dec 4. doi:10.3390/ijms21239271
- Suwal A, Hao JL, Zhou DD, Liu XF, Suwal R, Lu CW. Use of Intense Pulsed Light to Mitigate Meibomian Gland Dysfunction for Dry Eye Disease. Int J Med Sci. 2020 Jun 1;17(10):1385-1392.
- Blackie, C. A., Coleman, C. A., & Holland, E. J. (2016). The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clinical ophthalmology (Auckland, N.Z.), 10, 1385–1396
- Tauber J, Owen J, Bloomenstein M, Hovanesian J, Bullimore MA. Comparison of the iLUX and the LipiFlow for the Treatment of Meibomian Gland Dysfunction and Symptoms: A Randomized Clinical Trial. Clin Ophthalmol. 2020;14:405-418.
- Chester T. A Single-center Retrospective Trial of a Blink-assisted Eyelid Device in Treating the Signs and Symptoms of Dry Eye. Optom Vis Sci. 2021 Jun 1;98(6):605-612
- Jaccoma E, Litherland C, Jaccoma A, Ahmed A. Pellevé vs Lipiflow MGD-Related Dry Eye Treatment Study: The ThermaLid Procedure. Journal of Dry Eye Disease. 2018;1(1):e11-e21.
- Park, Y., Kim, H., Kim, S. et al. Effect of low-level light therapy in patients with dry eye: a prospective, randomized, observer-masked trial. Sci Rep 12, 3575 (2022). https://doi.org/10.1038/s41598-022-07427-6
