



Platelet rich plasma (PRP) is the future of dry eye treatment. In every form of dry eye disease, a lubricating eye drop is needed. However, even with the hundreds of artificial drops on the market, not a single drop comes close to matching the biochemistry of our own natural tears. PRP is not only similar to our natural tears in pH and osmolarity, but also contains several healing growth factors making it the perfect substitute lubricant in dry eye disease.
Blood biologics such as PRP are being used successfully in other parts of medicine for tissue regeneration including dermatology, orthopedics, dentistry, and cardiology. It certainly has its place in ophthalmological care too. Dry eye disease causes serious discomfort for patients and can negatively impact the quality of their life. For various reasons, there is a breakdown in our biological tears which leads to the development of dry eye disease.
One of the missing links in treating ocular surface disease is the need for lubricants that mimic the properties of our natural tears. We know that human tears not only contain several vitamins, proteins and growth factors which nourish and protect the ocular surface, but they also have anti-inflammatory and antimicrobial activities.1 Not only is PRP made of similar content as the natural tears, but they also contain no preservatives, stabilizers or additives found in artificial products. PRP has been reported as a successful treatment for dry eye disease. It may be considered superior to autologous serum due to its richer concentration of growth factors and other platelet derivatives.
What is platelet rich plasma (PRP)?
Our blood is made of several components including red blood cells, white blood cells, platelets and plasma. To produce PRP, blood from patients is collected and centrifuged with an anticoagulant. The anticoagulant prevents clotting of blood and activation of platelets, thus keeping the platelets in their native form. Centrifugation separates the blood components, making the red and white blood cells settle at the bottom of the collection tube since they are the densest. Platelets and plasma remain on top and are collected with a syringe and put in eye drop bottles to be used as eye drops by patients. PRP can contain 2.5 to 8.0 times the concentration of platelets found in whole blood.2
What is so special about platelets and plasma?
Platelets are the first cell type to arrive at the site of tissue injury.3 They are considered tiny powerhouses for healing damaged tissue. They contain an abundance of growth factors which are released to repair injured tissue. It’s these growth factors that are thought to be responsible for cell growth, collagen production, cell adhesion and healing of corneal and conjunctival cells.2,3,4 The specific function of growth factors can be found in Table 1.
Plasma also plays an important role in tissue repair and is required for optimal platelet function.5 Plasma is rich in albumin, proteins, immunoglobulins and electrolytes. Albumin is particularly important as it reduces the degradation of growth factors and cytokines in areas of tissue injury.5,6 Plasma components also aid in neutralizing inflammatory cytokines and preventing microbial invasion.
By using PRP as eye drops for dry eye disease, we are not only providing high concentration of healing growth factors but also cytokines and proteins that help to reduce inflammation, prevent infections, and have natural analgesic actions to reduce pain.6
Growth factors found in platelets and their function2,3,4
| Growth Factors In Platelets | Function of Growth Factor |
|---|---|
| Platelet Derived Growth Factor (PDGF) | Cell growth, regeneration and repair of blood vessels, collagen production, mitogenic properties |
| Epithelial Growth Factor (EGF) | Proliferation and migration of epithelial cells, inhibit apoptosis and acceleration of wound healing |
| Vascular Endothelial Growth Factor (VEGF) | Promotion of wound healing, promotion of angiogenesis |
| Transforming Growth Factor Beta (TGF-β) | Growth and neogenesis of epithelial cells and vascular endothelial cells and promotion of wound healing |
| Insulin Growth Factor (IGF) | Regulates cell growth |
| Keratinocyte Growth Factor (KGF) | Growth of keratinocytes |
| Fibroblast Growth Factor (FGF) | Tissue repair, cell growth and collagen production |
| Nerve Growth Factor (NGF) | Proliferation of epithelial cells, restores function of injured neurons |
Autologous serum is not Platelet Rich Plasma
While autologous serum shares many properties with PRP, it is important to note that PRP carries several advantages over autologous serum.
Autologous serum does not contain platelets
To make autologous serum, blood is allowed to clot in the collection tube before it is centrifuged. The clotting process activates the platelets to release their content including growth factors in the collection tube rather than in response to tissue injury at the site of damaged tissue. The centrifugation then separates the blood components and activated platelets settle at the bottom of the tube with red blood cells.
Autologous serum is considered platelet-poor since platelets are actually eliminated in the process of making it. As a result, autologous serum has significantly lower growth factor levels when compared to PRP.2,6 It is also important to note that serum is not the same as plasma. Serum is the liquid that remains after clotting has occurred and therefore contains lower concentrations of tissue repairing plasma factors.6,7
Autologous serum contains inflammatory cytokines
Some studies indicate that autologous serum of patients with active autoimmune diseases such as secondary Sjogren’s Syndrome have significantly higher amounts of inflammatory cytokines which are deleterious to the ocular surface and can lead to further damage.7 It is the presence of leukocytes during the autologous serum preparation procedure which increases the level of proinflammatory cytokines such as interleukin 6 and tumor necrosis factor-α.8 In addition, autologous serum also contains high amounts of Transforming Growth Factor Beta (TGF-β). Although this platelet-derived growth factor plays an important role in epithelial cell repair, in high amounts, it is thought to suppress wound healing.
Autologous serum is often diluted with saline to reduce the concentration of inflammatory cytokines and TGF-β in serum.4,8 However, this further dilutes the concentration of the healing growth factors. The most common concentration used in clinical studies for autologous serum is 20%. PRP, on the other hand, is not diluted with saline before dispensing.
Benefits of PRP
The simple process of manufacturing PRP maintains the integrity of the platelets and allows the platelets to activate at the site of tissue injury rather than in a test tube. It is thought that when the platelets activate in response to the damaged tissue, the growth factors released are presumably in a biologically relevant ratio. Because it is the combination of these factors and their interactions that leads to homeostasis rather than factors acting in isolation.9,10
JUST RELEASED: The 2025 Dry Eye Report
Get insights from hundreds of optometrists in the highly-anticipated 2025 Dry Eye Report! Explore trends, treatments, tools, and advice to help you stay ahead in dry eye management, all for FREE! Click here to download!
Who and when to treat?
PRP eye drops have been shown to be effective in the treatment of moderate to severe dry eye disease (both evaporative and aqueous deficiency) including neuropathic and LASIK induced dry eye disease.9,11,12,13 Studies have also shown that PRP eye drops promote healing of dormant corneal ulcers that failed other treatment options.10 Furthermore, they were shown to significantly reduce the mean frequency of recurrent corneal erosions in patients with epithelial basement membrane dystrophy.11
TFOS DEWS II recommends treatment with blood-based products as third-line therapy in the management of dry eye disease. However, many eye care experts may favor blood-derived eye drops as a second-line therapy, citing their potential advantages over traditional therapies and low profile for side effects.
How accessible is PRP?
Manufacturing PRP eye drops is minimally invasive and uncomplicated. However, the process can be overwhelming as there are currently over 40 different systems available that make PRP in medicine.8 Furthermore, there is no standardized protocol in place to manufacture PRP. The final concentration of platelets in PRP depends on how much blood is drawn, how long the blood is spun in the centrifuge, and at what speed.
However, even with these variations, blood products have a role in treating dry eye disease, and access to these products is improving. Optometrists can look to implement a PRP system in their own practice or work in conjunction with local labs and pharmacies to make PRP eye drops. At Vancouver Eye Doctor, we have been using PRP eye drops for our dry eye patients for the last two years and have found it to be an effective option for recalcitrant dry eye.
Results of our patient using PRP eye drops can be seen in figures 1 and 2.
Figure 1 shows results of PRP eye drops used four times a day for three months in severe ocular surface disease.

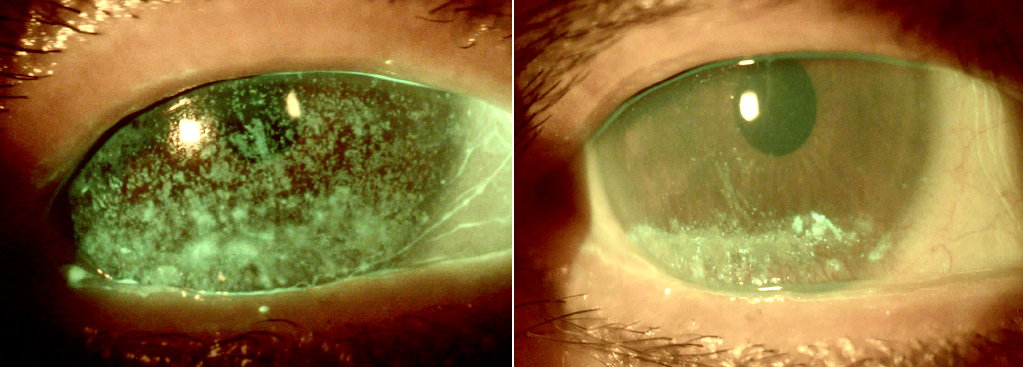
Figure 1
Figure 2 demonstrates results of a patient with LASIK induced dry eye disease using PRP eye drops as monotherapy for two months.

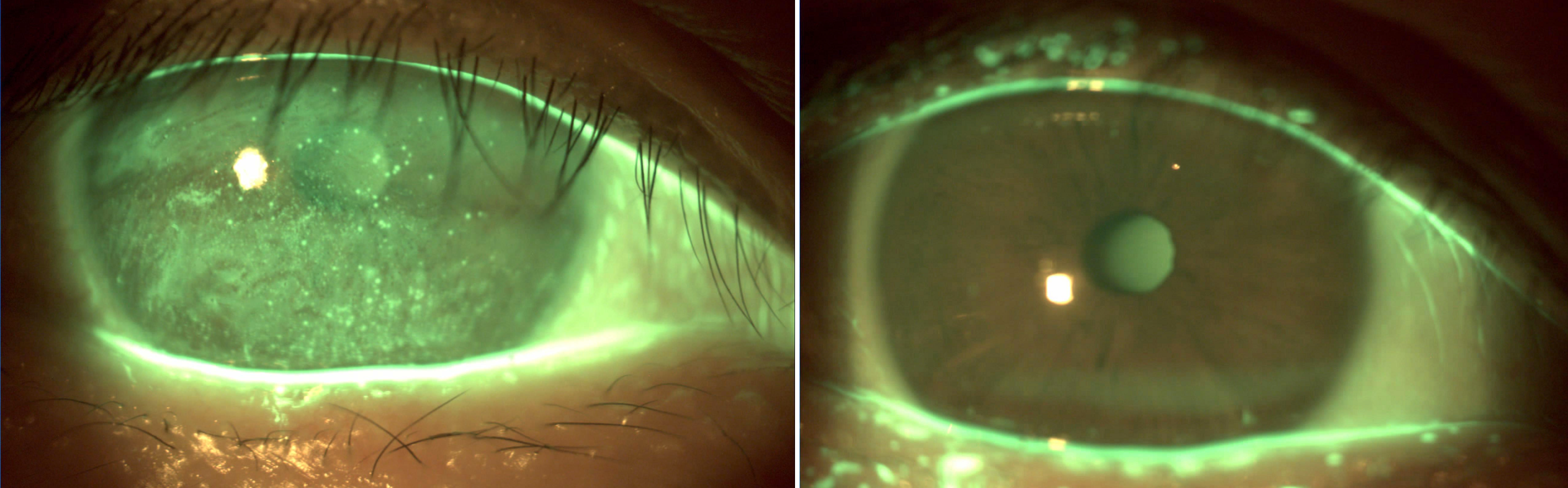
Figure 2
How is PRP used?
PRP eye drops are typically used four to six times a day for dry eye disease treatment for three months, then at a frequency determined by their optometrist for ongoing management. An average blood draw (100ml) yields about a three-month supply of PRP eye drops. It is critical that patients maintain the safe handling of blood products to prevent contamination. Drops must be kept in the refrigerator or stored in the freezer when not being used. Patients could expect to pay $400-$600 for a three-month supply of PRP eye drops. PRP can be used as monotherapy or in conjunction with other therapies such as immunomodulators or in-clinic lid treatments.
What else is in the pipeline?
The advancement in the field of blood biologics for ocular surface disease has seen a huge increase and has sparked interest for doctors and patients due to their safe and effective profile; but we are still only at the surface of understanding our body’s ability to heal.
Although studies have indicated that PRP is effective for evaporative dry eye disease, currently clinical evidence is lacking if PRP can regenerate meibomian glands. PRP has been injected into meibomian and lacrimal glands and is showing promising results; however, the sample sizes are too small.12 There are a plethora of studies in dermatology and orthopedics that support tissue regenerative properties of PRP, so I am eager to see its further role in ophthalmological care.
With options like autologous serum, PRP, cenegermin, amniotic fluid and amniotic membranes, it will be exciting to see high-quality clinical trials comparing these treatment options. But for now, a standardized protocol to manufacture autologous blood products is desperately needed. Currently, the only consensus that exists is that PRP is an effective treatment for ocular surface disease; however, at what concentration of platelets and its components is the most effective — this is to be told!
References:
- Zhou L, Zhao SZ, Koh SK, Chen L, Vaz C, Tanavde V, et al. . In-depth analysis of the human tear proteome. J Proteom. (2012) 75:3877–85. 10.1016/j.jprot.2012.04.053
- Alio JL, Rodriguez AE, Ferreira-Oliveira R, Wróbel-Dudzińska D, Abdelghany AA. Treatment of Dry Eye Disease with Autologous Platelet-Rich Plasma: A Prospective, Interventional, Non-Randomized Study. Ophthalmol Ther. 2017;6(2):285-293. doi:10.1007/s40123-017-0100-z
- Boswell SG, Cole BJ, Sundman EA, Karas V, Fortier LA. Platelet-rich plasma: a milieu of bioactive factors. Arthroscopy. 2012 Mar;28(3):429-39. doi: 10.1016/j.arthro.2011.10.018. Epub 2012 Jan 28. PMID: 22284405.
- Hartwig D, Harloff S, Liu L, Schlenke P, Wedel T, Geerling G. Epitheliotrophic capacity of a growth factor preparation produced from platelet concentrates on corneal epithelial cells: a potential agent for the treatment of ocular surface defects? Transfusion. 2004 Dec;44(12):1724-31. 10.1111/j.0041-1132.2004.04079.x.
- Ribeiro M, Ribeiro E, Ribeiro L. The Use of Platelet-Rich Plasma in Dry Eye Disease. DOI: 10.5772/intechopen.76090
- Cole BJ, Seroyer ST, Filardo G, Bajaj S, Fortier LA. Platelet-rich plasma: where are we now and where are we going?. Sports Health. 2010;2(3):203-210. doi:10.1177/1941738110366385
- Ma IH, Chen LW, Tu WH, Lu CJ, Huang CJ, Chen WL. Serum components and clinical efficacies of autologous serum eye drops in dry eye patients with active and inactive Sjogren syndrome. Taiwan J Ophthalmol. 2017;7(4):213-220. doi:10.4103/tjo.tjo_102_17
- Villatoro AJ, Fernández V, Claros S, Alcoholado C, Cifuentes M, Merayo-Lloves J, Andrades JA, Becerra J. Regenerative Therapies in Dry Eye Disease: From Growth Factors to Cell Therapy. Int J Mol Sci. 2017 Oct 28;18(11):2264. doi: 10.3390/ijms18112264. PMID: 29143779; PMCID: PMC5713234.
- Kim KM, Shin YT, Kim HK. Effect of autologous platelet-rich plasma on persistent corneal epithelial defect after infectious keratitis. Jpn J Ophthalmol. 2012 Nov;56(6):544-50. doi: 10.1007/s10384-012-0175-y. Epub 2012 Sep 13. PMID: 22972393.
- Alio JL, Abad M, Artola A, et al. Use of autologous platelet-rich plasma in the treatment of dormant corneal ulcers. Ophthalmology. 2007;114:1286–1293.e1
- Lee JH, Kim MJ, Ha SW, Kim HK. Autologous Platelet-rich Plasma Eye Drops in the Treatment of Recurrent Corneal Erosions. Korean J Ophthalmol. 2016;30(2):101-107. doi:10.3341/kjo.2016.30.2.101
- Avila MY. Restoration of human lacrimal function following platelet-rich plasma injection. Cornea. 2014 Jan;33(1):18-21. doi: 10.1097/ICO.0000000000000016. PMID: 24240491.
- Sanchez-Avila RM, Merayo-Lloves J, Riestra AC, Fernandez-Vega Cueto L, Anitua E, Begoña L, Muruzabal F, Orive G. Treatment of patients with neurotrophic keratitis stages 2 and 3 with plasma rich in growth factors (PRGF-Endoret) eye-drops. Int Ophthalmol. 2018 Jun;38(3):1193-1204. doi: 10.1007/s10792-017-0582-7. Epub 2017 Jun 15. PMID: 28620707.
