Flares are an inevitability of
dry eye, no matter how well managed a patient may be, eventually, they will experience a flare in their signs and/or symptoms.
With this thought in mind, dry eye can be a chronic and progressive disease—so how do you determine if a patient is experiencing a flare rather than a progressive worsening of their condition?
What is a dry eye flare?
Put simply, a dry eye flare (DEF) is an acute exacerbation of a chronic condition. This means the worsening of signs or symptoms will develop quickly in a true DEF, as opposed to a gradual onset.
Additionally, DEFs are often associated with specific aggravating factors such as overwearing contact lenses,
digital screen usage, seasonal changes, chronic medications (i.e., glaucoma), or surgical procedures like cataract and
microinvasive glaucoma surgeries.
Presentation of dry eye flares
The presentation of a DEF can range from a relatively mild increase in irritation with an otherwise quiet eye to a significant worsening of symptoms with severe inflammation and
disruption of the ocular surface.
While the severity of the DEF will dictate the aggressiveness of treatment, all DEF treatments should have two characteristics in common:
- They are fast-acting
- They are only intended for short-term use
Because DEFs are an acute problem and develop quickly, an ideal treatment should be equally fast-acting and thus only require a relatively short duration of use. Therefore, DEFs do not typically require a drastic overhaul of the patient’s base treatment protocol but rather the temporary addition of another complementary therapy to get them “over the hump” and through the flare period.
These criteria make topical corticosteroids an excellent choice in the management of DEF, and highlight where steroids best fit within the dry eye treatment paradigm.
Using topical steroids to treat DEFs
Topical steroids provide rapid relief but should only be used for a short duration to avoid potentially serious side effects associated with prolonged use, such as premature cataracts,
1-6 an increase in IOP, and glaucoma development.
7 “Therefore, an over-reliance on steroids to manage dry eye symptoms should be avoided.”
However, this does not mean steroids should be feared or avoided entirely but rather used logically, and their proper use clearly communicated to patients to minimize these risks. Through proper identification of the signs and symptoms of DEFs and judicious use, steroids can be a particularly powerful and effective treatment option.
Determining a treatment approach for DEFs
The clinical presentation of the DEF can be used to determine the course of treatment. While many DEFs are relatively mild, some can be significant with severe inflammation and ocular surface disruption; however, as previously mentioned, the general treatment approach is the same—treatments should be fast-acting and, therefore, only require a short duration of use.
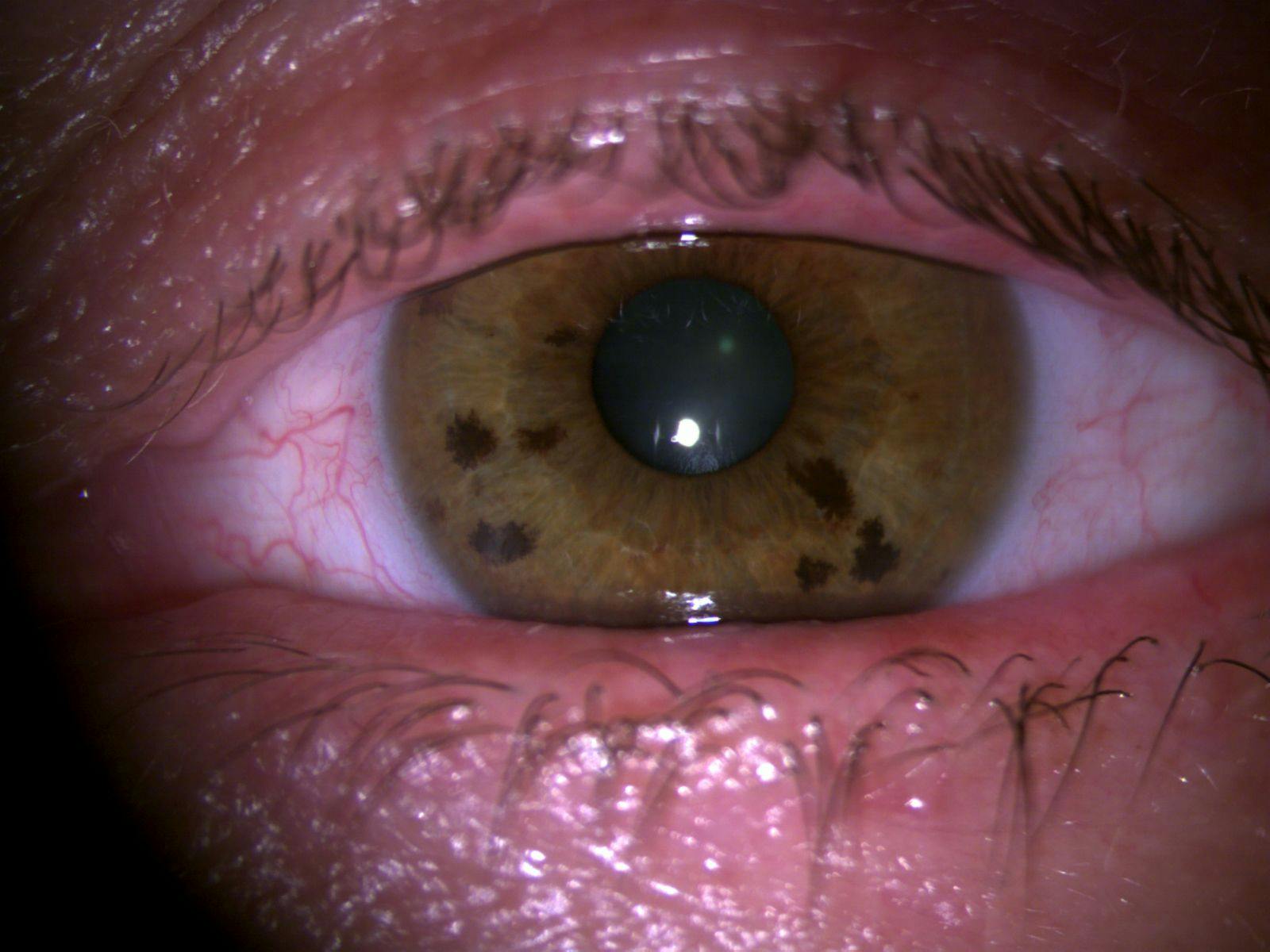
In cases of relatively mild disturbance, where the DEF is limited to primarily an increase in symptoms with little to no worsening of signs, like the mildly injected eye shown in Figure 1, typically a short pulse (e.g., BID-QID x 1 to 2 weeks) with “soft” steroids, such as loteprednol or fluorometholone, will be sufficient to resolve the DEF.
Soft steroids are excellent treatment options for many DEFs, as they are rapidly metabolized at their target site, which makes them less likely to elicit the side effects more commonly observed in “harder” steroids, such as Pred Forte (prednisolone acetate ophthalmic suspension 1%, Allergan, an AbbVie Company) or Durezol (difluprednate ophthalmic emulsion 0.05%, Novartis).8-15
Additionally, when topical steroids are dosed for 2 weeks, which is often sufficient to alleviate mild DEFs, the likelihood of a significant impact on IOP is minimal.16
Using Eysuvis to treat DEFs
Personally, I prefer to use Eysuvis (loteprednol etabonate ophthalmic suspension 0.25%, Alcon) when treating DEFs due to its FDA indication for the short-term treatment of
dry eye (which also confers an additional medicolegal benefit) and its vehicle that allows for a lower concentration which further enhances its safety profile.
However, this is not always an option due to cost and
insurance coverage, so generic formulations of loteprednol or the use of another soft steroid like Flarex (fluorometholone acetate ophthalmic suspension 0.1%, Santen) can be effective alternatives.
Figure 1 is a clinical image of a mildly injected eye.
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO
Ocular surface disruption
In cases of significant ocular surface disruption, treatment becomes a bit more complex. To help simplify choosing a treatment approach, I divide these more challenging DEFs into cornea-sparing and cornea-involving cases.
As the names suggest, in cases of cornea-sparing DEFs, only the conjunctiva is affected, whereas, in cornea-involving cases, the cornea also exhibits impairment, usually in the form of superficial punctate keratitis (SPK), evolving limbal stem cell deficiency, and/or
neovascularization.
17-19Cornea-sparing dry eye flares
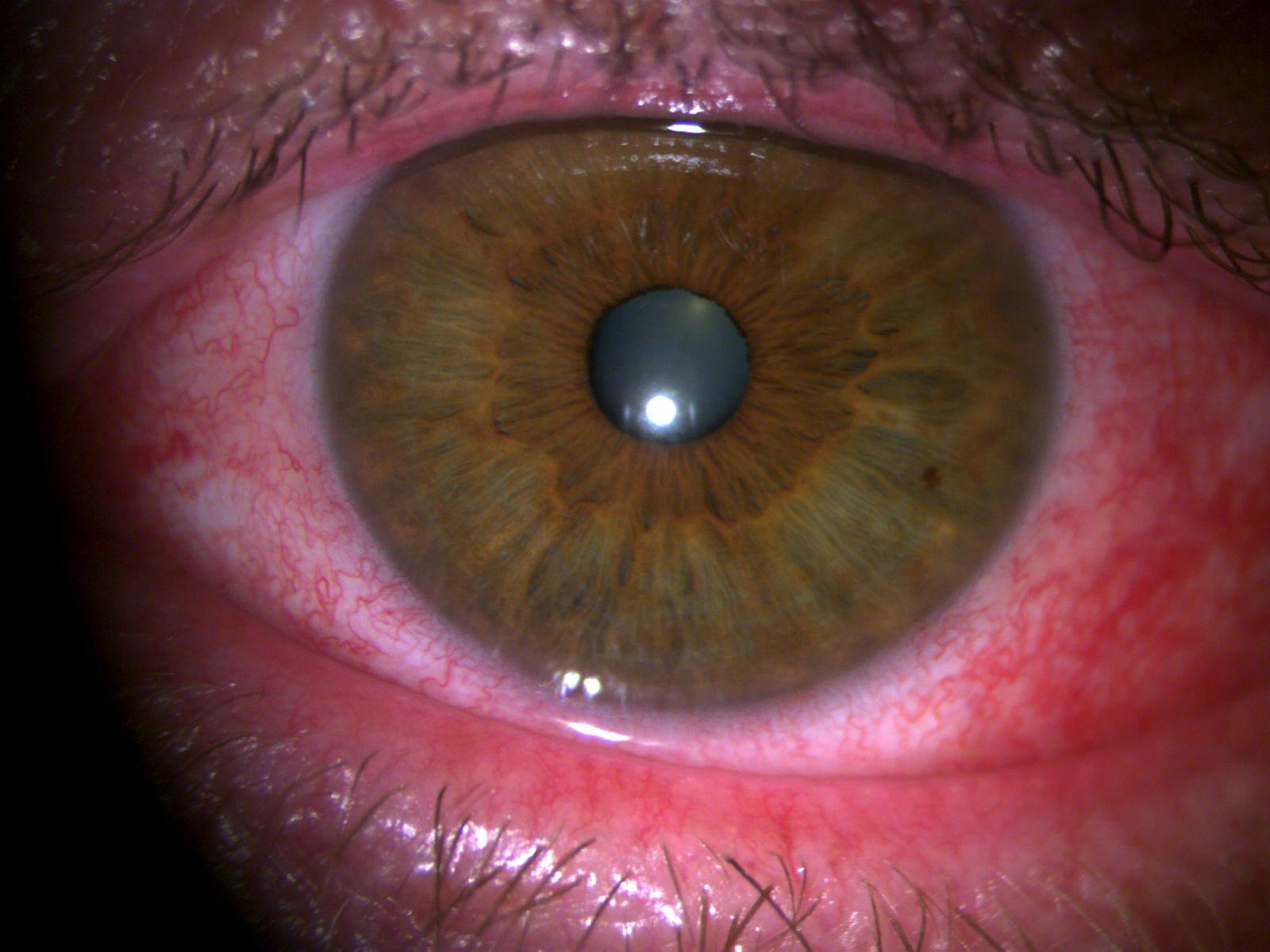
However, just because corneal-sparing DEFs are limited to the conjunctiva does not necessarily mean they are less severe, especially as rosacea conjunctivitis and immunogenic conjunctivitis associated with inflammatory and autoimmune disease can be some of the most challenging forms of dry eye to manage, such as the
ocular rosacea flare depicted in Figure 2.
In most cases of DEFs involving significant inflammation that is limited to the conjunctiva, I usually implement a steroid taper, typically tapered down from QID to QD over 4 weeks. In addition to the longer dosing, I usually implement a stronger steroid, such as Pred Forte or generic prednisolone acetate ophthalmic suspension 1%, as the more severe inflammation warrants the use of a stronger steroid.
“A common mistake I have encountered in these more severe cases is the use of a ‘soft’ steroid in a pulse pattern.”
This inevitably results in a vicious cycle of discontinuing and restarting the medication because the inflammation is never fully controlled by the weaker steroid. I liken this to using a squirt gun on a house fire since the softer steroid is just not strong enough to fully quench the inflammation present.
Using strong steroids to treat cornea-sparing dry eye flares
That being said, stronger steroids carry a higher side effect profile, so this can translate to the development of side effects.13-15 Of special note, there can be an increase in IOP as 18 to 36% of the population are steroid responders, which needs to be monitored closely.7
In cases where an IOP spike occurs but the
inflammation is not yet resolved, I typically start the patient on an IOP-lowering agent, such as a fast-acting combo drop like Simbrinza (brinzolamide/brimonidine tartrate ophthalmic suspension 1%/0.2%, Alcon) or Combigan (brimonidine tartrate/timolol maleate ophthalmic solution 0.2%/0.5%, Allergan) to use BID until they are finished with the course of their steroid treatment, as immediately discontinuing the steroid would halt any progress and risk the occurrence of rebound inflammation.
I would recommend reviewing medication allergies to ensure one or more of these active ingredients is not contraindicated for treatment for these patients.
Figure 2 is a clinical image of a patient with an ocular rosacea flare.
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO
Cornea-involving dry eye flares
In cases of cornea-involving DEFs, my approach differs. While steroids are a logical choice for the treatment of DEFs, they are not the only option. Two other extremely effective treatments are soft bandage contact lenses (BCLs) and
amniotic membranes. Even though a steroid would also seem like a logical choice in these cases, and although they can be effective, I typically opt for the use of a bandage contact lens or amniotic membrane instead.
The rationale behind this treatment approach is that the corneal surface has been compromised, resulting in SPK and/or neovascularization, such as the case in Figure 3; therefore, stabilizing the cornea arguably has the greatest therapeutic benefit. Additionally, the inflammation present in cases such as these is more often a result of the
ocular surface disruption rather than the cause of it, so the use of a topical steroid would be directed at the symptoms rather than the underlying cause of the DEF.
In most cases, a soft bandage contact lens paired with a prophylactic antibiotic, such as moxifloxacin 0.5% TID, will successfully reestablish the integrity of the corneal surface after 1 to 2 weeks (with the BCL switched out weekly).
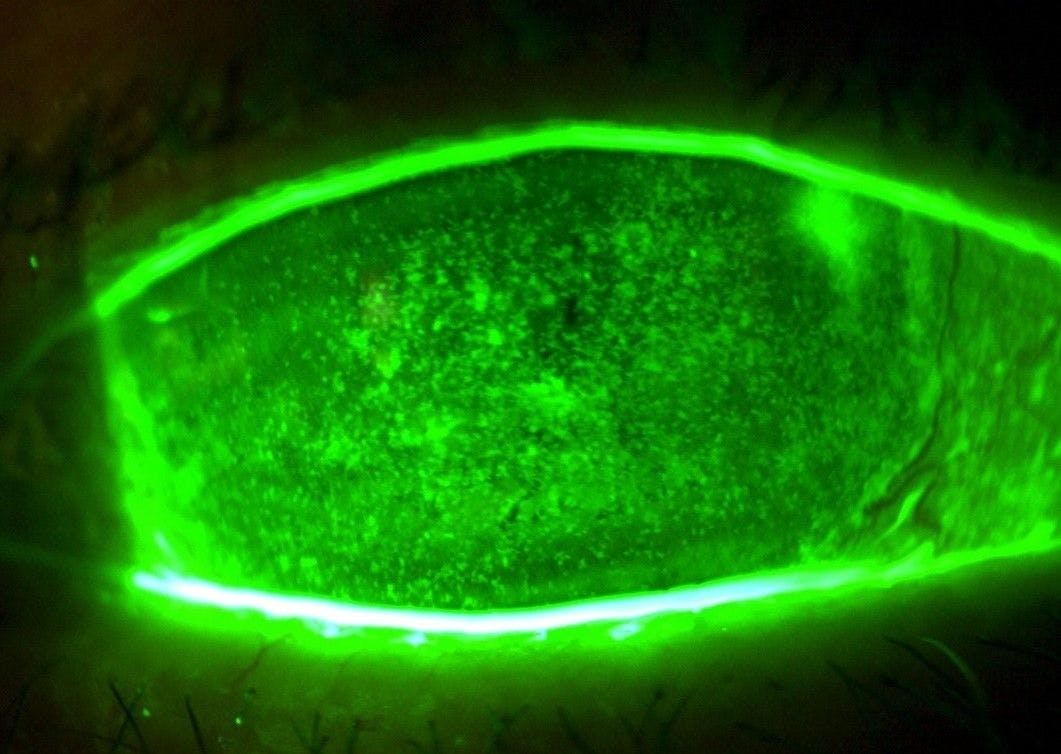
However, in cases where there is a significant corneal disruption or where neovascularization is also involved, like that shown in Figure 4, with the added risk for visually significant scarring, I use amniotic membranes due to their anti-inflammatory, anti-angiogenic, anti-fibrotic, and regenerative properties.20-25
Figure 3 shows a compromised corneal surface resulting in SPK and/or neovascularization.
Figure 3: Courtesy of Cory Lappin, OD, MS, FAAO
Using amniotic membranes to treat cornea-involving dry eye flares
While I will sometimes use a dehydrated amniotic membrane such as AcellFX (acellular amniotic membrane, Théa Pharma), Aril (acellular amniotic membrane, Seed Biotech), or XcellerEYES (lyophilized amniotic membrane, Oculus Biologics), especially if I suspect a patient will not be able to tolerate the plastic carrier ring used in cryopreserved amniotic membranes.
I more frequently utilize a cryopreserved membrane, such as PROKERA Slim (BioTissue Ocular), due to the enhanced efficacy and greater retention of anti-inflammatory and growth factors afforded by the cryopreservation process.
26 Additionally, the effects of the
amniotic membrane can persist for months after its use.
27In both cases, I may also incorporate the use of low-dose doxycycline (20 to 50mg QD-BID) as an adjunct oral treatment due to its anti-inflammatory and anti-angiogenic properties. Be aware doxycycline should not be used in
pregnant or nursing mothers or in children under 12 years old.
28-30 I also routinely start patients displaying neovascularization on Lumify (brimonidine tartrate ophthalmic solution 0.025%, Bausch + Lomb) BID.
This is not so much for its cosmetic benefit (although it does improve redness dramatically) but rather for its action as an α-2 adrenergic receptor agonist, which may reduce inflammation through its vasoconstrictive effects by reducing vascular permeability and the subsequent leakage of proinflammatory factors onto the ocular surface.31-33
Additionally, brimonidine has been shown to reduce vascular endothelial growth factor (VEGF) production,34 and may potentially hinder the development of neovascularization.35
In Figure 4, the patient has significant corneal disruption with neovascularization.
Figure 4: Courtesy of Cory Lappin, OD, MS, FAAO
Treating DEFs and allergic conjunctivitis
A separate but potentially confounding condition that warrants specific mention in the context of DEF management is
allergic conjunctivitis. Ocular allergies pose two challenges: one is that an allergy flare presents similarly to a DEF, and the second is that a flare in allergies can also cause a DEF, so the two conditions can be present simultaneously. Additionally, it is known that both allergies and dry eye tend to worsen in the spring months.
36,37Thankfully, an allergic component is easily identified by the presence of itching, which typically worsens upon rubbing the eyes, versus the itching in dry eye that often improves with eye rubbing,38-40 conjunctival papillae, and stringy or ropey discharge.
If any of these signs or symptoms are present during a flare, the use of a mast cell stabilizer-antihistamine combo such as Pataday Once Daily Relief Extra Strength (olopatadine hydrochloride ophthalmic solution 0.7%, Alcon) or Lastacaft (alcaftadine ophthalmic solution 0.25%, Allergan) can effectively address an allergic component of the DEF.
Final thoughts on treating dry eye flares
In summary, DEFs are acute episodes of
dry eye exacerbation with a relatively quick onset, so they should be managed with fast-acting treatments, such as topical steroids, bandage contact lenses, or amniotic membranes.
Consequently, this means they should respond quickly as well, so only a short duration of treatment should be necessary. Therefore, if you find that the condition has shown little to no improvement after about 4 weeks of treatment, or the patient experiences rapid regression of their signs or symptoms once the treatment has been discontinued, this indicates the patient is likely dealing with an actual progression in their disease state rather than a temporary flare.
“In this case, employ treatments that are more appropriate for long-term use.”
Appropriate long-term treatments include the addition of an
immunomodulator like Xiidra (lifitegrast ophthalmic solution 5%, Novartis), Cequa (cyclosporine ophthalmic solution 0.09%, Sun Pharmaceuticals), or Restasis (cyclosporine ophthalmic emulsion 0.05%, Allergan), or a chemical neurostimulator, like Tyrvaya (varenicline solution nasal spray 0.03mg, Viatris) may be warranted as these treatments do not carry the same side effects as steroids, and are well-tolerated for long-term use.
However, the use of these long-term agents is indefinite and usually lifelong, so it is best to avoid making a significant change to a patient’s base treatment regimen unless you are certain that the worsening of their condition is not a temporary exacerbation, as DEFs only require a short course of treatment rather than the addition of a long-term therapy.
DEFs can cause significant disruption to the everyday lives of our patients, but by managing these troublesome exacerbations, we not only provide much-needed relief but potentially improve their quality of life as well.