As eyecare providers (ECPs), it is guaranteed that we will encounter
Demodex mites during the course of routine patient care, the reason being that Demodex are part of our skin’s natural microfauna, so we will all display signs of Demodex at some point in our lives.
1-5Demodex: we all have it
Demodex are ectoparasitic mites that inhabit our hair follicles and oil glands, including the eyelash follicles and meibomian glands of the eyelids, with each of these niches being occupied by a specific species of Demodex mite—the larger Demodex folliculorum in the lash follicles, and the smaller Demodex brevis in the meibomian glands.2,5-11
Demodex are present in males and females of all races and ethnicities, and though it may be more common as we age, Demodex can be seen in all ages, including pediatric populations.
1-5,12-19 In fact, it is estimated that 55 to 58% of all patients presenting for eyecare have
Demodex blepharitis (DB), representing a potential 25 million cases.
20-22When Demodex becomes a problem: Diagnosing DB
While it is normal for all of us to display Demodex, if our resident Demodex population overgrows this, homeostatic balance is lost. This is when issues such as eyelid itching, dryness, irritation, foreign body sensation, epiphora, redness, inflammation, and even lash loss can occur as the mites begin causing mechanical damage by feeding on epithelial cells and sebum.
In turn, this stimulates inflammation by regurgitating digestive enzymes and waste on the ocular surface, harboring bacteria,
physically obstructing the meibomian gland orifices and lash follicles, and altering meibum composition.
1,2,5-7,11,22-33 At this point, we have transitioned beyond a normal Demodex population and into demodicosis and Demodex blepharitis.
However, it is worth noting that while these signs and symptoms are concerning, they are not particularly specific and can be observed in numerous ocular surface diseases, such as dry eye and ocular allergy. So, how do we know we are dealing with DB and not some other ocular surface disease?
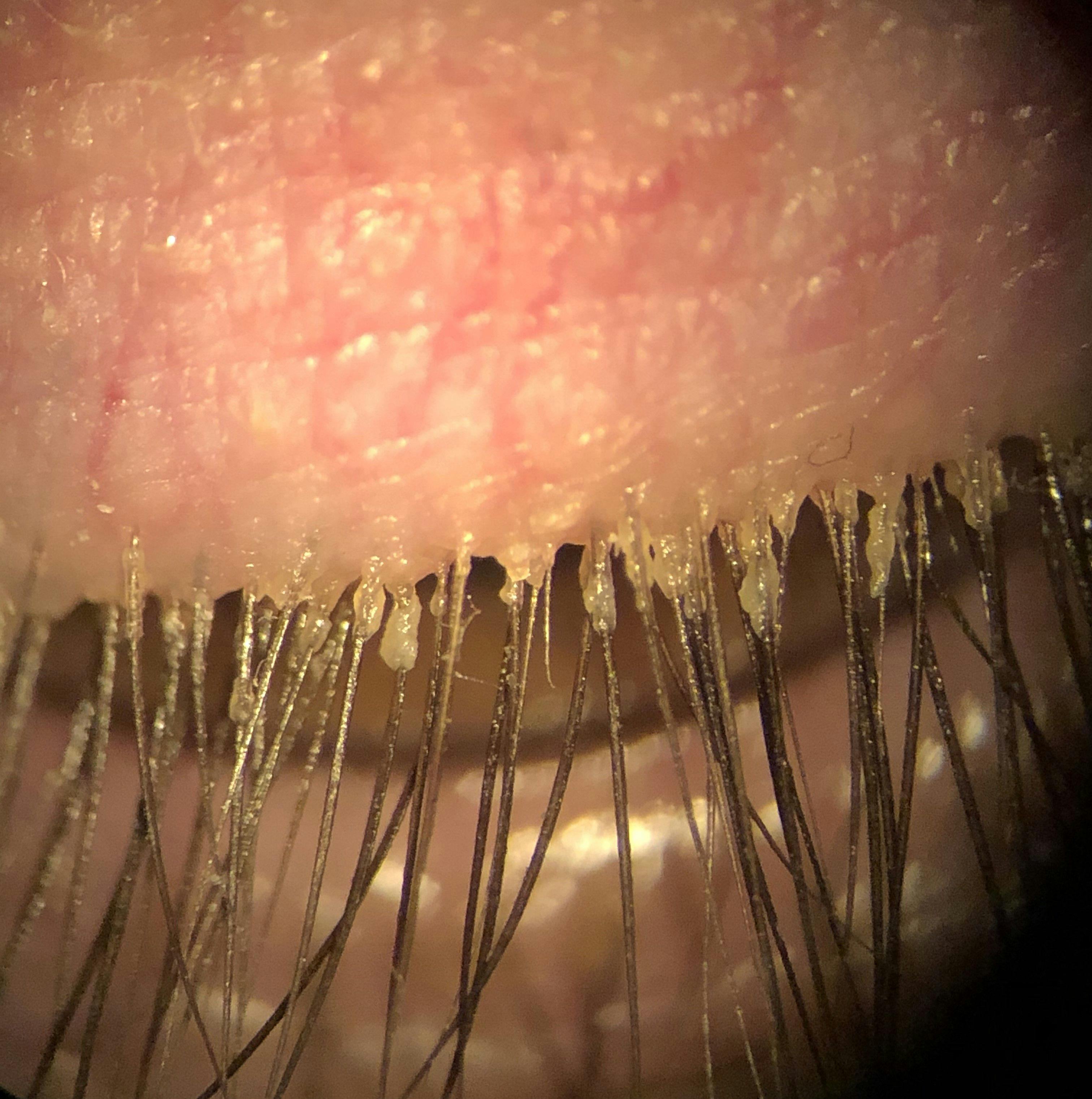
Fortunately, DB is associated with a telltale sign in the form of lash collarettes. Collarettes are a waxy buildup of debris that encircles the base of the lashes, as seen in Figure 1, and consist of Demodex waste, eggs, and regurgitated material, including digestive enzymes, epithelial cells, and keratin.5,6,25-27,34,35 Collarettes are considered pathognomonic for Demodex, so diagnosis is relatively easy and straightforward.25,27,34,36
The best way to look for collarettes is to have your patient look down behind the slit lamp and then scan the bases of the lashes, as this will bring the collarettes directly into view. Having the patients look down is an important step, because it can be easy to miss collarettes, especially those that are subtle when the patient is looking straight ahead.
Figure 1 is a closeup image of a patient with lash collarettes, a telltale sign of Demodex blepharitis.
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO.
Talking to your patients about Demodex blepharitis
Due to this straightforward diagnosis, identifying DB is not the point of difficulty for most ECPs, but rather the ensuing conversation is the primary source of apprehension. So now that you have seen the collarettes, and know your patient has DB, or they ask you about it directly, how do you handle that conversation?
I have found that many doctors are hesitant to discuss DB with their patients for two primary reasons: 1) they aren’t entirely confident in discussing DB as a disease state, or 2) they don’t want to open a can of worms (or should I say a can of mites) by bringing up a topic that could potentially derail an exam and take up valuable chair time due to the understandably visceral response that is often elicited when you tell someone they have parasitic mites on their eyelids.
However, this conversation does not have to be complicated or overly lengthy—in fact, the way I present DB to patients typically takes 1 to 3 minutes or less.
Below is the script I routinely use when discussing DB with patients:
“When I was looking at your eyelids, I saw a little bit of debris on the eyelashes that we refer to as collarettes. These collarettes are caused by tiny mites that live on our lids and lashes called Demodex. Now, it is completely normal to have these Demodex mites because they are a natural part of our skin’s ecosystem, so we all have them. But if they overpopulate, they can cause eye irritation, including itching, redness, and dryness. Do you ever experience any of these symptoms?”
This is a great way to start the conversation and it only takes about 30 seconds, which will then segue nicely into a discussion about treatment. A key concept to understand about DB is that we do not know at what exact point a Demodex population goes from being normal to an overpopulation, however, if a patient has more than 10 collarettes, it is more likely they will have a significant Demodex infestation.1,6,27
Explaining the signs and symptoms of DB to patients
However, I like to simplify diagnosis even further by thinking about DB in terms of signs and symptoms. If a patient is completely comfortable and has no
eyelid redness or inflammation, then I explain we have two options: we can treat the mites before any problems develop, or we can observe for the time being and encourage them to let me know if symptoms ever arise in case treatment is needed in the future.
But, if the patients have any of the aforementioned signs and/or symptoms in the presence of lash collarettes, then it is very likely the mites are causing or contributing to this ocular surface disruption. At this point, I will strongly recommend treatment as they have now transitioned from a normal Demodex population to demodicosis and DB.
My philosophy with discussing DB with patients is if you see something, say something. What I mean by this is I always educate patients about DB, even if they only have mild collarettes, because we have all had a patient say, “Why didn’t my last doctor tell me I had that?” You never want to be the “last doctor” in this scenario.
In fact, even if you don’t end up treating the patient, they still often credit the doctor who first mentions a condition, as we have all also been told upon discussing a clinical finding, “Oh yeah, my last doctor mentioned that!” Therefore, if you see that a patient has collarettes, whether mild or severe, I strongly recommend having a conversation about DB.
Discussing DB treatments with patients
One scenario I like to discuss regarding DB treatment is addressing asymptomatic Demodex blepharitis. Ideally, we would treat all patients with DB, even asymptomatic patients. This would allow us to treat the condition before the patient ever develops any symptoms, and I recommend doing so whenever possible.
So, if a patient has DB and is asymptomatic but wishes to address the disease, the situation is straightforward and they should begin treatment. However, things become a bit more nuanced if a patient has collarettes but is asymptomatic and hesitant to undergo treatment because they are not experiencing any problems.
Factoring in the symptom-drive psychology of patients
While some may disagree, I personally do not push asymptomatic patients toward treatment if they seem hesitant or resistant, and there are a couple of reasons I take this approach. First is
patient psychology. Most of us, by nature, are symptom-driven. We often do not seek care unless something is causing a problem, whether it is pain or loss of function.
The perfect example is
glaucoma—how many of our glaucoma patients are non-compliant with their drops because they are not experiencing any perceivable effects of the disease even though it could lead to permanent vision loss? Similarly, many patients do not want to undergo treatment if they do not feel like they are experiencing a tangible problem.
That being said, I discuss DB with any patient that has collarettes and recommend treatment, regardless if they are symptomatic or asymptomatic because it is my responsibility as their doctor to educate them about their clinical findings and provide all available therapeutic options for any treatable conditions. But ultimately, the choice to pursue treatment is up to them. Some may be thinking, “But if you don’t treat them now, what if the condition gets worse and they never get treated?”
Planting the seed of awareness for DB symptoms
This leads to my second point, which is patients are, again, symptom-driven. Even if a patient is asymptomatic in the present, that doesn’t mean they will remain that way. Therefore, if they desire to observe rather than treat their condition, I explain the signs and symptoms associated with DB and advise them to let me know if any of these issues ever develop in the future. I call this “planting a seed.”
Now that patients know they have Demodex, and the issues they can cause, they will specifically be looking for these signs and symptoms, and they almost always come back for treatment eventually. For instance, a patient with some of the heaviest lash collarettes I have ever seen was completely asymptomatic and elected to monitor his DB after we discussed treatment.
But the next year, when he returned for his comprehensive exam, even though he claimed he was still largely asymptomatic, he wanted to pursue treatment. The seed had sprouted. And sometimes, patients actually are symptomatic and they just don’t realize it, and it takes time to come to this realization. Therefore, my recommendation is if a patient is hesitant to pursue treatment, educate them on what to look for between the present exam and their next visit, and they will almost always return if there is a problem.
Scripts for discussing treatments with symptomatic and asymptomatic DB patients
However, I will say even asymptomatic DB patients tend to elect for treatment at higher rates than other ocular surface conditions, even
dry eye, because of the innate, visceral reaction many have to being told they have mites living on their lids and lashes. Therefore, many patients will want to “get rid of them” regardless of symptoms or lack thereof.
Below is an example of how I convey this treatment philosophy to patients based on whether or not they are symptomatic.
You can present an asymptomatic patient with two courses of action to gauge their interest in treatment:
“It's great that the Demodex are not currently causing any issues. At this point, we have two options: we can start treatment and get rid of the mites before they create any problems, or we can keep a close watch on the condition, and you can let me know if you start to develop any eye irritation or redness, and then we can start treatment at that time. Do you have a strong preference for either option?”
Now, if the asymptomatic patient elects for treatment or the patient reports symptoms from the beginning, the conversation may look like this:
“As I mentioned, it is normal for you to have these mites but it looks like they have overpopulated and are causing significant disruption of your ocular surface, and that is why you are experiencing eye irritation. At this point, I would recommend treatment to help you feel better and prevent the problem from getting worse.
In the past, we would primarily treat the mites with an eyelid hygiene routine using things like tea tree oil cleansers; however, now we have an FDA-approved eye drop specifically for the treatment of Demodex blepharitis called Xdemvy. You will use the Xdemvy drops two times per day for 6 weeks, and this will do an excellent job of eliminating the mites, and then afterward, we can use a lid hygiene routine for maintenance.”
Patient education tools available to ECPs
At this point, you will have successfully covered most of your bases in regards to DB education, from what DB is, what causes it, and what can be done to treat it. And again, this should only take a few minutes. If the patient is still curious, has additional questions, or would just like some more information you can direct them to several excellent additional resources.
One of these resources is the “
Miteaverse,” a clinical augmented reality experience created by Tarsus Pharmaceuticals as an educational platform that provides the patient with more in-depth, but still accessible, information about DB, its pathogenesis, symptoms, diagnosis, and impact on patients, which can be accessed via its web address or by scanning a QR code present on Tarsus’ educational Demodex model.
37Additional resources that can also be beneficial include models, like those in Figure 2, of Demodex mites that allow the patient to better visualize and tangibly interact with Demodex mites, as well as clinical photos of their own collarettes, or example images if slit lamp photography is not available, which helps them to see how DB manifests clinically. I have utilized all three of these resources with excellent patient responses, so they are great educational tools to keep at the ready.
Figure 2 highlights plush and plastic models of Demodex mites, which can be used as educational tools for DB patients.
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO.
Comparing current DB treatments on the market
I would also like to briefly review the treatment of DB in light of the recent Food and Drug Administration (FDA)-approval of Xdemvy ((lotilaner ophthalmic solution 0.25%, Tarsus Pharmaceuticals)), and the fact that treatment options are another potential source of questions for patients.
Tea tree oil cleansers
Traditionally, DB has been treated with lid hygiene, specifically,
tea tree oil (TTO), as it has demodicidal properties.
38-42 TTO is usually dosed QD to BID for a minimum of 6 weeks, as this corresponds to roughly two life cycles of the mites.
5,26 However, there is no established dosing criteria, with some ECPs electing to do a 6-week course and others having patients use the cleanser indefinitely for maintenance.
While TTO-based cleansers can be helpful in managing DB, they are imperfect treatments. One major downside to TTO is that it is, by necessity, a relatively harsh treatment as Demodex are quite resilient, so the use of TTO itself can result in irritation to the eyelid and ocular surface, including ocular discomfort, contact dermatitis, and allergic reactions.43
Additionally, the standard 2 to 5% TTO concentrations most commonly used for DB treatment are much lower than the concentrations that are typically suggested for optimal mite eradication due to the potentially irritating side effects of TTO, which are more pronounced at these higher concentrations.1,43,44 Also, despite its widespread use, a systematic literature review of the use of TTO for short-term treatment of DB determined that its efficacy in this context cannot be stated conclusively.45
Now, this is not to say that TTO-based cleansers and other hygiene-based treatments don’t have a place in DB management, as lid hygiene will always be a part of supporting ocular surface health, but with the advent of Xdemvy, we now have a better first-line treatment option.
Xdemvy
So, what is
Xdemvy? Xdemvy is lotilaner ophthalmic solution, which inhibits parasite-specific GABA-Cl channels, resulting in mite paralysis and death.
46-48 And because lotilaner has high lipophilicity, it can be readily absorbed into the eyelash follicles and meibomian glands, where the mites reside, and target them directly.
49In two pivotal studies, Xdemvy use (when dosed BID for 6 weeks) has been shown to significantly alleviate DB symptoms, such as:50-52
- Mite eradication: 60% of patients achieved complete mite eradication, defined as 0 mites per lash
- Collarette reduction: 50% of patients achieved complete collarette cure, defined as ≤2 collarettes on the upper lid, while clinically meaningful collarette cure, defined as ≤10 collarettes, was observed in 85% of patients
- Improvement in lid erythema: 25% of patients displayed erythema cure defined as grade 0 or no lid margin erythema on a 0 to 3 scale corresponding to no erythema, mild, moderate, and severe erythema, respectively when dosed BID for 6 weeks.
Xdemvy is generally well-tolerated, with 90% of patients reporting the drop to be neutral to very comfortable when used, and the most common side effect being stinging and burning upon instillation, which is usually mild and transient, and is experienced by 10% of patients.50-52 Given its robust efficacy, high tolerability, and status as the first and only FDA-approved treatment indicated for DB, Xdemvy now gives us a definitive-first line therapy for DB.53
The shifting DB treatment paradigm
Going forward, I foresee Xdemvy and traditional eyelid hygiene treatments being used in conjunction, with Xdemvy being the primary treatment and TTO cleansers, like EyeEco’s Advanced Formula 2% Tea Tree Eyelid & Facial Cleanser foam (PRN Vision Group), or okra-based cleansers, like ZocuFoam Eyelid Cleanser and Moisturizer (Zocular), being utilized as maintenance treatments after and/or between courses of Xdemvy as needed.
Additionally, for patients that experience heavy collarettes or general lid margin debris and biofilm buildup, adjunct in-office lid debridement procedures, such as NuLids PRO (NuLids) or BlephEx (BlephEx) could be beneficial,
44,54,55 as could
intense pulsed light (IPL) therapy, which has also been shown to have demodicidal capabilities.
56,57Although this represents a major shift in the treatment paradigm of DB, it will likely lead to far better outcomes than what we have been able to achieve previously with lid hygiene alone.
Bringing it all together
Although the idea of discussing the impact of a parasitic mite on ocular surface health with a patient may seem like a daunting task, educating your patients on DB doesn’t have to be some arduous or time-consuming conversation.
By providing a brief and easy-to-understand description of what Demodex mites are, how they can cause eye irritation, and how DB can be treated, we can provide effective patient education and formulate a DB treatment plan in just a few minutes.