



What is recurrent corneal erosion (RCE)?
First described in 1872, recurrent corneal erosion syndrome (RCE) is an “intermittent neuralgic vesicular keratitis.” Since then, the treatment approach has changed drastically and expanded to include advanced surgical options.
Treatment for RCE is intensive, time-consuming, and expensive for patients. It may be time to consider new approaches to therapy for this painful condition.
Identifying recurrent corneal erosion
Most people can identify a RCE based on the patient’s complaints and history. Sharp pain upon awakening is a hallmark sign of corneal erosions. Other patient symptoms may include foreign body sensation, tearing, and photophobia.
Often times, there is a history of trauma to the eye, most commonly from a fingernail scratch, paper cut, or tree branch.
The recurrence rate of epithelial erosion secondary to trauma has been found to be 1 in 150. Corneal diseases that have been associated with increased risk for RCE include: EBMD, Reis-Buckler, and Lattice/Granular/Macular dystrophy.
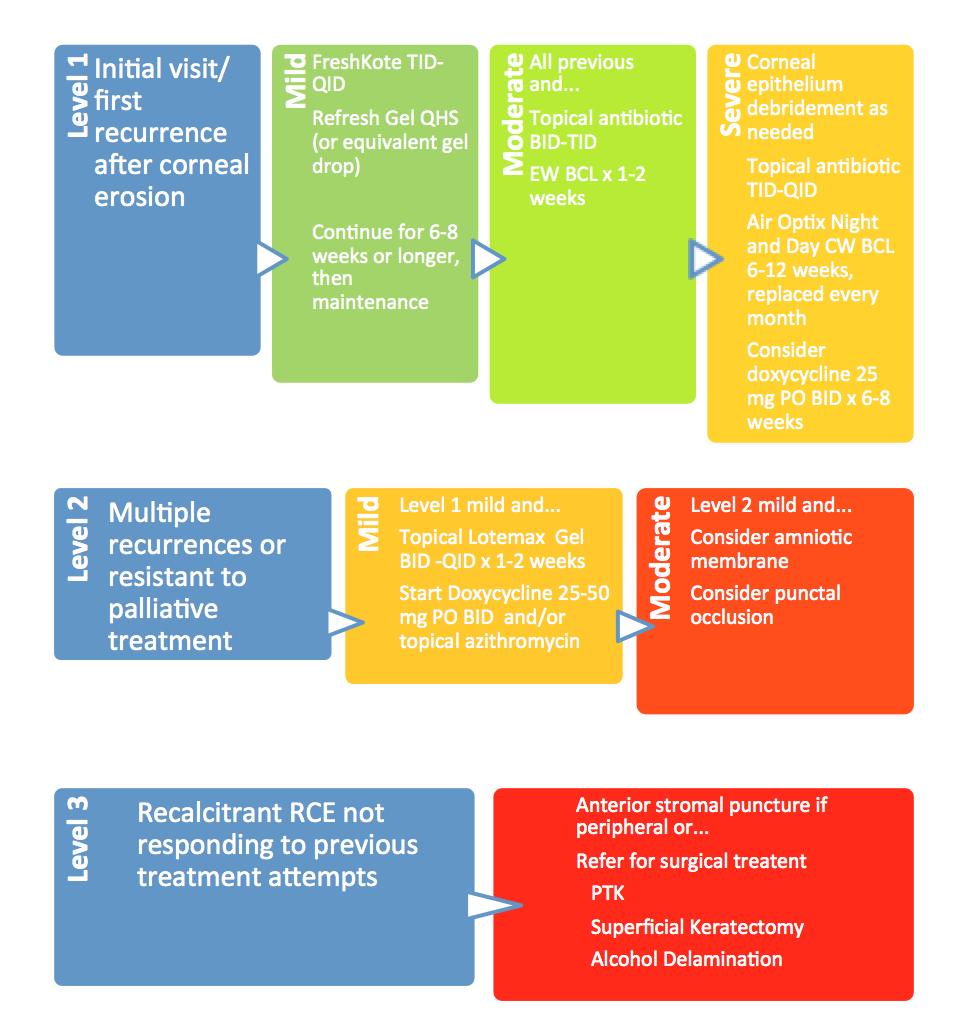
Common treatment options for RCE
The goal of treatment is to increase the strength of the hemidesmosome connection between the corneal epithelium and basement membrane (BM).
The mainstay and widely accepted initial treatment for RCE includes copious lubrication and sodium chloride (Muro-128) ointment at night. Recent clinical evidence has surfaced ideas that Muro-128 ointment may actually cause corneal epithelium to become loose and mushy and hinder the strength and time of healing between the epithelium and BM. More research is needed to prove this; however, a randomized study of 117 patients showed no difference in treatment success rate when comparing ophthalmic lubrication and hypertonic saline at night.
This has swayed me into using a regimen of FreshKote tears TID to QID during the day, for their advanced lubricating and increased surface regularity properties, with an ophthalmic lubricating gel at night.
A smooth, regular ocular surface is crucial for proper healing of the corneal epithelium, thus it is important to debride any loose epithelium with a moist cotton tip applicator, forceps, or medical sponge stick (Weck-Cel).
If the corneal erosion is large in size or especially painful, consider starting with a bandage contact lens at the initial visit with antibiotic drop coverage. An Air Optix Night and Day works excellent for this purpose because of its FDA approved monthly continuous wear use.
What to do in cases of severe RCE
For severe RCE, a bandage contact lens may be needed for up to three months, requiring the patient to return monthly for replacement of the Air Optix Night and Day contact.
At the follow-up visit, it is imperative that the contact lenses be floated before careful removal with forceps.
It is critical to understand that the BM heals over weeks to months and not within hours to days, as with the epithelium.
That is why these basic regimens should be maintained a minimum of 6-8 weeks with proper lubrication chronically after that.
Lubrication is key to healing; therefore, temporary punctal occlusion is an option to keep the ocular surface moist. However, I do not typically consider this unless other lubrication methods fail or the patient is non-compliant. If punctal occlusions is to be done, make sure that the inflammatory factors are under control first. Lacriserts are another option for the patient who is not compliant with lubricating drops.
The next level of treatment in a ladder approach therapy would be oral tetracyclines for their anti-inflammatory properties and MMP downregulation.
Studies have shown that there is an increase in neutrophils and MMP-9 and MMP-2 activity in RCE, which hinders the formation of the hemidesmosomes. Doxycyline 25-50mg BID works well for treatment of RCE.
Again, this should be maintained for at least 6-8 weeks for moderate cases and possible low-dose chronically for recalcitrant RCE. Topical azithromycin has also been shown to be effective at downregulating MMP activity on the ocular surface and can be used alone or in conjunction with tetracyclines.
Other medications that may be applied include topical corticosteroids and NSAIDs. Another option to acknowledge before considering surgical procedures would be the placement of a sutureless amniotic membrane (Prokera, AmbioDisk). Amniotic tissue is excellent at decreasing inflammation, promoting healing and lessening scarring and hazing. Doctors should strive to achieve a minimum of seven days with the amniotic membrane before removal, with a longer duration desirable based on patient acceptance.
Surgical options when other approaches fail
If previous treatment approaches have failed, referring for surgical options must strongly be considered.
With the advances in medical technology and procedures, we have many surgical tools in our belt to treat RCE. These include phototherapeutic keratectomy (PTK), superficial keratectomy with or without diamond bur polishing, alcohol delamination and anterior stromal puncture (peripheral corneal RCE only).
Patients should be warned that a small prescription change is possible with PTK.
As doctors we must remember that RCE is a painful condition that decreases the quality of life for our patients. Repeated visits to the doctor’s office can be time consuming and financially debilitating.
A combination of treatments has been shown to be the most effective method of management of RCE, with successful surgical options available if previous treatments fail.
It is important to stay up to date with the clinically proven methods of RCE treatment and refer as necessary for a surgical approach.

Disclaimer: I have no financial interest in any of the companies, brands, or products mentioned in this article.
References:
Foster, C. Stephen, Azar, Dimitri T., and Dohlman, Claes H.. Smolin and Thoft’s The Cornea : Scientific Foundations and Clinical Practice (4th Edition). Philadelphia, PA, USA: Wolters Kluwer, 2004. ProQuest ebrary. Web. 11 March 2016.
Mencucci, R, Favuzza, E. Management of recurrent corneal erosions: are we getting better? British Journal of Ophthalmology. 2014;98(2):150–151. Available at: http://bjo.bmj.com.proxy.lib.pacificu.edu:2048/content/98/2/150.full. Accessed March 11, 2016.
Sowka, JW, Gurwood, AS, Kabat, AG. The Handbook of Ocular Disease Management. Supplement to: Review of Optometry. 2013;150(6):34A–38A.
