


“Hey Doc, my eye is red! Can you send in an antibiotic for me?” is a very familiar call that optometry offices receive daily. As primary eyecare providers, optometrists need a detailed subjective history as well as a thorough in-office examination to make a timely and appropriate diagnosis for each patient with this common presentation.
At first glance, it may be difficult to determine if your patient has conjunctivitis, episcleritis, or scleritis and it may be a diagnostic conundrum at times. However, this article will help make it easier to arrive at the correct diagnosis, treatment plan, and follow-up needed to best take care of our patients who depend on us for our expertise.
Conjunctivitis overview
Conjunctivitis is defined as inflammation of the conjunctiva, the outermost mucous membrane covering the globe (bulbar conjunctiva) and the lining of the inside of the eyelids (palpebral conjunctiva).
Conjunctivitis may be infectious, arising from viruses, bacteria, fungi, or parasites. It may also be non-infectious and result from allergens, toxins, mechanical stimuli, and/or reactive inflammation from dry eye syndrome or ocular rosacea.
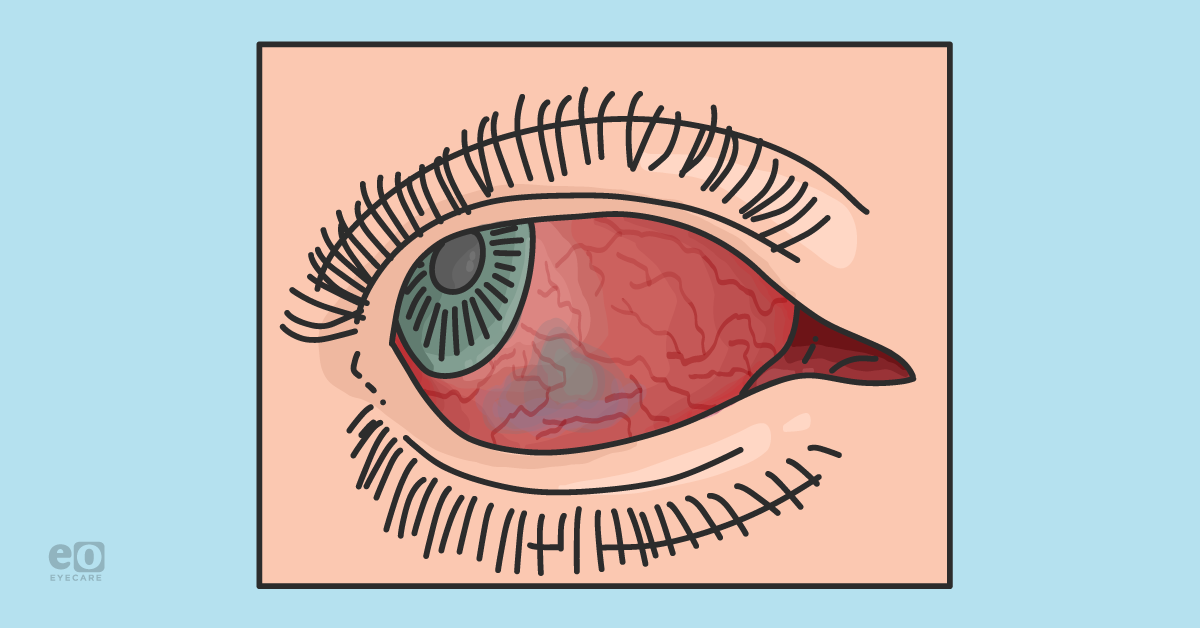
A patient who has conjunctivitis presents with unilateral or bilateral red eyes with watery, mucoid, ropy/stringy, or purulent discharge depending on the specific etiology. The entire bulbar and palpebral conjunctiva may be affected, and the patient may exhibit papillae or follicles on the palpebral conjunctiva.
Many patients also have chemosis and/or eyelid edema secondary to the increased vascular permeability.1,2 Their symptoms include irritation, itching, burning, and sometimes photophobia.
Figure 1 shows a patient with viral conjunctivitis.


Figure 1: Image provided by Cory Lappin, OD, MS, FAOO
Patients with infectious conjunctivitis most likely have a known recent history of direct contact with another individual with conjunctivitis or other infectious exposure, or a personal history of a recent upper respiratory infection.
In non-infectious cases, the patient may have had exposure to a known or novel allergen, toxic substance or foreign body, or they may have a history of ocular rosacea, blepharitis, or dry eye syndrome.
Conjunctivitis does not typically have any serious systemic associations, although there are some exceptions. These include chlamydia, gonorrhea, herpes simplex, herpes zoster, rosacea, thyroid dysfunction, and sleep apnea (linked to floppy eyelid syndrome). Even less frequent are tuberculosis, cat scratch disease, and Lyme disease.1,2
Diagnosing conjunctivitis
A diagnosis of conjunctivitis is primarily made via a detailed subjective history and observing patient symptoms, as well as a thorough slit lamp examination. A clinician may decide to culture the conjunctiva to confirm or rule out certain pathogens, especially if the patient is not responding to the initial treatment.
Additionally, if the optometrist wants an in-office confirmation of a viral versus bacterial infection, in an effort to reduce unnecessary topical antibiotics, they can use the Quickvue adenoviral conjunctivitis test (Quidel), which gives rapid results in 10 minutes and has a 90% sensitivity and 96% specificity for adenoviral conjunctivitis.3
Get the cheat sheet!

Conjunctivitis, Episcleritis, & Scleritis Differential Diagnosis Cheat Sheet
Use this cheat sheet as a guide for diagnosing and treating conjunctivitis, episcleritis, and scleritis.

Treatment for conjunctivitis
The treatment for conjunctivitis depends on the specific etiology.
Bacterial conjunctivitis
Bacterial conjunctivitis is most likely due to one of the following pathogens: Haemophilus influenzae, Streptococcus pneumoniae, Staphylococcus aureus, and Staphylococcus epidermidis.4-6 The best choice for a topical antibiotic would be one that is broad-spectrum with low resistance, and these typically include fluoroquinolones.
This class of antibiotics includes the second-generation ciprofloxacin 0.3% and ofloxacin 0.3%, which are typically dosed every 2 hours for 2 days then four times daily for the next 5 days. Gatifloxacin is a fourth-generation fluoroquinolone that has two formulations with concentrations of 0.3% and 0.5% and is dosed at four times a day for 7 days.
The other fourth-generation fluoroquinolones, moxifloxacin 0.5% and besifloxacin 0.6%, are both dosed three times a day for 7 days. Besifloxacin is unique as it is an ophthalmic suspension and has strong MRSA coverage. Another great choice would be polymyxin B/trimethoprim due to its spectacular MRSA coverage and relative low cost compared to besifloxacin.
Azithromycin 1% has a very simple dosing schedule with the recommended dose of two times daily for 2 days, and then once daily for the following 5 days. This makes it attractive for the pediatric population or those with barriers to a more frequent dose schedule, but has high indices of resistance to the common pathogens.
Tobramycin 0.3% is another great inexpensive alternative, however it may cause corneal toxicity. In severe infections, it is also helpful to have a nighttime antibiotic ointment (ciprofloxacin or bacitracin/polymyxin B) for extra coverage.
Chlamydial and gonococcal conjunctivitis
If chlamydial conjunctivitis is suspected, patients can be prescribed a single dose of 1g oral azithromycin. Alternatively, a 7 to 14 day course of doxycycline 100mg BID is a good choice, and treatment can be augmented with erythromycin ointment as well. Gonococcal conjunctivitis typically requires hospital admission and IM or IV penicillin or ceftriaxone.
Viral conjunctivitis
Viral conjunctivitis is typically treated using supportive therapy with refrigerated artificial tears and cold compresses. If subepithelial infiltrates are present with epidemic keratoconjunctivitis (EKC) and visual acuity is reduced, then topical steroids, such as loteprednol etabonate 0.5% QID, are recommended.
Some optometrists who use an in-office and off-label 5% betadine wash to reduce the viral load and reduce the duration of symptoms in those with suspected or confirmed adenoviral conjunctivitis, but the utility of this is not universally accepted.7,8
If the viral pathogen is suspected to be herpes simplex or herpes zoster, then oral antivirals should be prescribed. Typically, topical ganciclovir is not required in cases of herpetic conjunctivitis.
Fungal and parasitic conjuctivitis
Fungal conjunctivitis is treated with topical natamycin 5%, compounded amphotericin B, or voriconazole. Acanthamoeba conjunctivitis requires a long duration of treatment with compounded PHMB or chlorhexidine and brolene.
Allergic conjuctivitis
Allergic conjunctivitis is often treated with topical antihistamine/mast cell stabilizers, such as ketotifen, olopatadine, alcaftadine, or cetirizine. Patients with more severe symptoms of chemosis and eyelid edema may benefit from topical steroids as well.
Loteprednol 0.2% or 0.5%, or fluorometholone 0.1% are great choices due to their efficacy on the ocular surface and their safety profile. Ketorolac 0.5% is a topical NSAID with FDA approval for allergic conjunctivitis, but it is not commonly used in practice due to the more effective alternatives previously discussed.
Dry eye
Conjunctivitis secondary to tear film instability from dry eye syndrome and ocular rosacea may be treated with protocols including artificial tears, cyclosporine 0.05% or 0.09%, lifitegrast 5%, topical steroids, and sometimes oral doxycycline.
Eyelid therapy is also recommended, including at-home therapies with warm compresses, eyelid massage, hypochlorous acid solutions, and in-office therapies such as LipiFlow, iLux, and intense pulsed light therapy.9
Follow-up care for conjunctivitis depends on the etiology and severity of the presentation. Patients should be educated on warning signs and directed to call the office for an urgent appointment if they experience any of the following: increased or new redness, pain, light sensitivity, or worsening vision.
Depending on the type of conjunctivitis, most patients with acute conjunctivitis should experience improvement within a few days, but more chronic cases may take several weeks.
Episcleritis
Episcleritis is inflammation of the episclera, the thin layer of loose connective tissue between the conjunctiva and the sclera. Episcleritis is most often idiopathic, but, like conjunctivitis, may have an identified infectious or noninfectious etiology.10
Patients with episcleritis present with an acute onset of unilateral or bilateral red eyes with mild discomfort or pain, but they characteristically do not have any discharge or photophobia, contrary to most types of conjunctivitis.
During the clinical examination, the episcleral vessels will be dilated and engorged. The pattern of hyperemia may be diffuse, involving the entire bulbar conjunctiva, or it may be sectoral and involve only the nasal or temporal quadrant.
Figure 2 demonstrates a patient with episcleritis.


Figure 2: Image provided by Alanna Nattis, DO, FAOO
The hyperemic tissue may be flat or have a raised nodule and is differentiated into simple episcleritis or nodular episcleritis respectively. To help differentiate between episcleritis and scleritis (to be discussed in the next section), topical phenylephrine 2.5% to 10% can be used to evaluate the layer of tissue involved.
If the vessels involved are episcleral, they will blanch after about 10 to 15 minutes and the eye will be relatively white and quiet. Scleral vessels do not blanch with phenylephrine and the eye will remain significantly hyperemic if this deeper layer of vessels is involved.
Conditions concomitant with episcleritis
About 30% of patients with episcleritis have an associated collagen-vascular disease or autoimmune disorder, such as rheumatoid arthritis, Crohn’s disease or ulcerative colitis, psoriatic arthritis, systemic lupus erythematosus, and others.10,11 Rarely, episcleritis has an infectious etiology, but it may be caused by Lyme disease, cat scratch disease, syphilis, or herpes simplex/herpes zoster.
There are no laboratory or radiographic imaging tests to diagnose episcleritis, but a clinician may want to order laboratory testing if a systemic disorder or infectious disease is suspected based on a review of systems.
These tests comprise a general workup, including: a complete blood count, erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, antinuclear antibody, anti-cyclic citrullinated peptide, HLA-B27, antineutrophil cytoplasmic antibody, as well as disease-specific testing when indicated.10-14
Treatment for episcleritis
Episcleritis is self-limited and will resolve within 2 to 3 weeks. Optometrists can recommend supportive treatment with refrigerated artificial tears. If symptoms are significant, then patients may benefit from a topical steroid such as fluorometholone 0.1%, loteprednol etabonate 0.5%, or prednisolone acetate 1% QID for 1 to 2 weeks, then tapered down.
The inflammation associated with episcleritis should not require topical difluprednate 0.05% or oral steroids. Oral NSAIDs such as ibuprofen (600 to 800mg BID-QID) or naproxen (250 to 500mg BID-TID) may be a useful adjunctive therapy, or an alternative to topical steroids if contraindicated. Topical NSAIDs are not typically useful in the treatment of episcleritis.
Patients with episcleritis should follow up with their optometrist within 1 to 2 weeks to evaluate for resolution and monitor intraocular pressure if they are on topical steroid therapy.
Episcleritis itself does not produce enough inflammation to cause any long-term ocular or systemic effects. However, patients on topical steroids need to be educated on the potential for increased IOP and cataract formation. Patients on oral NSAIDS should be cautious of gastrointestinal upset and gastric ulcers and should take an antacid as prevention.
If the episcleritis is secondary to a collagen vascular disease or autoimmune condition, then those patients need to have scheduled follow-up care with their rheumatologist to closely monitor their systemic health.
Scleritis
Scleritis is inflammation of the sclera and is classified as anterior or posterior scleritis depending on if the inflamed tissue is anterior or posterior to the insertion of the extraocular recti muscles. Anterior scleritis can be diffuse, nodular, or necrotizing and is more common than posterior scleritis, which is either diffuse or nodular.
Scleritis is most commonly non-infectious and secondary to autoimmune disease-related inflammation, but may also be secondary to infection, ocular surgery (especially when MMC is used), a side effect of medication, or be idiopathic in nature.10
Patients with anterior scleritis describe a gradual onset of severe redness and deep boring pain that may radiate to the ear or jaw, often awakening them from sleep. It may occur unilaterally or bilaterally. These patients likely have pain with eye movement, photophobia, tearing, and may even have reduced visual acuity.
On exam, they present with such a robust redness to their sclera that it often has a violet-blue hue. This is usually easier to appreciate in normal room illumination instead of behind the slit lamp and may involve the entire sclera or a localized sector. Nodular scleritis is characterized by multiple nodules within the inflamed tissue, while necrotizing scleritis involves scleral thinning with possible choroidal exposure.
Figure 3 features a non-necrotizing scleritis.

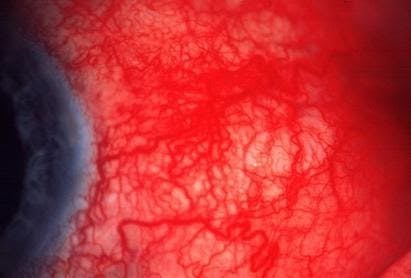
Figure 3: Image provided by Alanna Nattis, DO, FAOO
As previously discussed, the engorged and dilated vessels do not blanch with topical 2.5% or 10% phenylephrine compared to the vessels that do blanch in episcleritis. Moderate or severe cases of scleritis may also exhibit varying degrees of corneal edema and/or an anterior chamber reaction.
A very rare form of necrotizing anterior scleritis called scleromalacia perforans is diagnosed when the patient is asymptomatic but has severe progressive scleral thinning. Posterior scleritis presents alone or with anterior scleritis and may be associated with reduced visual acuity. It is possible to see serous retinal detachments, choroidal folds, an optic disc edema, vasculitis, and cotton wool spots.10-14
Figure 4 illustrates a patient with scleromalacia perforans.

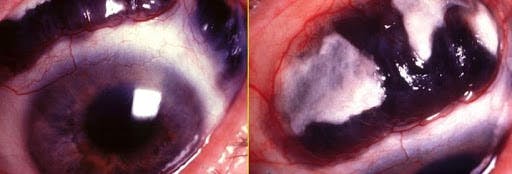
Figure 4: Image provided by Alanna Nattis, DO, FAOO
It is estimated that about 50% of patients with scleritis have a coexisting autoimmune or collagen vascular disease—most often rheumatoid arthritis. Others include polyangiitis with granulomatosis, relapsing polychondritis, polyarteritis nodosa, sarcoidosis, and systemic lupus erythematosus.10-14
B-scan ultrasonography can be utilized in the office to confirm posterior scleritis with the pathognomonic T-sign. This refers to the appearance of a thickened posterior sclera and fluid in Tenon’s capsule surrounding the optic nerve.
Laboratory and radiographic imaging studies should be ordered to evaluate for an associated systemic disease when indicated. These tests and studies include those discussed for episcleritis, but may also require ELISA for Lyme disease and PPD, a chest X-ray for tuberculosis, and RPR and FTA-ABS for syphilis.
Figure 5 shows B-scan ultrasonography to confirm posterior scleritis. Note the pathognomonic T-sign.

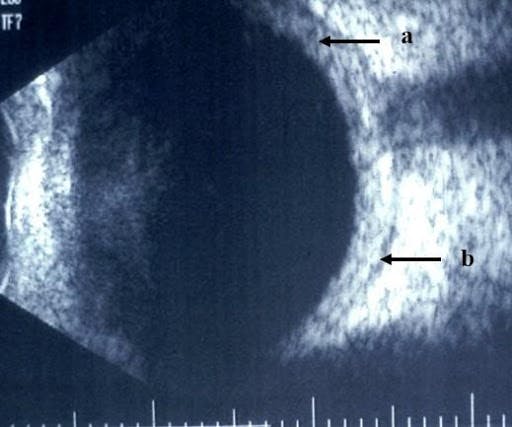
Figure 5: Image provided by Alanna Nattis, DO, FAOO
Treatment for scleritis
Treatment for scleritis is tiered according to severity, progression, and contraindications. Topical steroids such as prednisolone acetate 1% and difluprednate 0.05% are of limited use, but may be helpful in mild cases of anterior scleritis or if there is concurrent corneal edema or iritis.
Oral NSAIDs are typically the first line of treatment. Common dosages and frequencies are indomethacin 50mg PO TID, ibuprofen 600 to 800mg TID-QID (maximum daily dose 3200mg) or naproxen 500mg BID-TID (maximum daily dose 1500mg).
If oral NSAIDs are contraindicated or ineffective to quiet the inflammation, then treatment with oral prednisone (1mg/kg/day) is initiated and then tapered as the condition improves. Subconjunctival steroid injections or IV methylprednisolone may also be considered.
If oral steroids are contraindicated or ineffective, then the patient may require treatment with immunosuppressants such as methotrexate, cyclophosphamide, mycophenolate, or biologics, such as infliximab and rituximab.
Patients undergoing treatment for scleritis require frequent follow-up care with their eyecare provider to ensure clinical improvement and to monitor for treatment side effects. These patients also need to be under the care of a rheumatologist due to the high likelihood of an associated systemic disease to prevent other significant comorbidities or even mortality.
Don't forget to download the Conjunctivitis, Episcleritis, & Scleritis Differential Diagnosis Cheat Sheet!
Conclusion
Through reading this article, you now are aware of the similarities and differences between conjunctivitis, episcleritis, and scleritis, and it is clear what the key components are to an effective differential diagnosis:
- Detailed history, including a review of systems.
- Careful slit lamp examination.
- Utilize clinical tools available in the clinic, such as the Quickvue adenoviral conjunctivitis test (Quidel), 2.5% to 10% phenylephrine, B-scan ultrasonography, and viewing the patient’s ocular surface under normal room illumination.
Optometrists may be the first-line clinicians to see a patient with an acute red eye, or they may be a second or third opinion after failure to improve after treatment from an urgent care or primary care provider. To make an efficient and accurate diagnosis, prescribe the correct treatment, and by doing so, healing your patients will promote trust in you and generate plenty of referrals.
