



Introduction
Autoimmune diseases have a variety of systemic manifestations; the eye is frequently involved in numerous autoimmune and rheumatologic disorders. Ocular manifestations are frequently nonspecific and different diseases may affect different parts of the eye, but early recognition of symptoms can help avoid or delay both systemic and ocular sequelae.
The most common autoimmune diseases that affect the eyes can be separated into four categories:
- Rheumatologic
- Dermatologic
- Endocrine
- Vascular
This is part one of a four-part series in which we discuss autoimmune rheumatologic diseases and the eye including:
- Rheumatoid arthritis
- Sjögren's syndrome
- Seronegative spondyloarthropathies
Rheumatoid arthritis 1-5
Rheumatoid arthritis - epidemiology
- Disease
- Incidence in USA:40 per 100,000 persons
- Prevalence
- .024-1% of population
- 2:1 (women: men)
- Age: 30-50
- Eye manifestations
- 27.2% of patients with RA
Rheumatoid arthritis - mechanism
- Vasculitis
- Vascular occlusion
- Infiltration
- Fibrinoid necrosis
- Immune complex deposition
- Complement activation
- Autoantibodies
- Secretion of collagenases by macrophages and neutrophils
- Cytokine production
Rheumatoid arthritis - presentation
- General
- Symmetrical inflammatory polyarthritis
- Joint deformities
- Nodules (Proximal interphalangeal joints (PIP)>Distal interphalangeal joints (DIP))
- Constitutional symptoms
- Joint stiffness
- Fever
- Weight loss
- Symmetrical inflammatory polyarthritis
- Anterior segment more commonly affected than posterior segment
Rheumatoid arthritis presenting with keratoconjunctivitis sicca (most common)
- Mechanism
- Dysfunction of
- Meibomian gland
- Lacrimal gland
- Accessory lacrimal gland
- Goblet cells
- Dysfunction of
- Characteristics
- Foreign body sensation
- Burning
- Decreased visual acuity
- Photophobia
- Pruritis
- Complications
- Superficial punctate keratitis
- Filamentary keratitis
- Corneal ulcer
- Corneal melt
- Diagnosis
- 25% meet criteria for secondary Sjögren's Syndrome (SS)
- Schirmer’s Test
- < 5mm tear extension
- Tear break up time
- < 5 seconds
- Decreased lacrimal lake
- Staining
- Fluorescein
- Rose Bengal
- Lissamine green
- Treatment
- Lubricating drops/ointment
- Topical cyclosporine
- Oral pilocarpine
- Topical Lifitegrast
- Punctal occlusion
- Amniotic membrane
- Tarsorrhaphy
Rheumatoid arthritis presenting with episcleritis
- Mechanism
- Inflammation of episclera
- Characteristics
- 40% bilateral
- Salmon-pink eyes
- Mild pain
- Occurs in a sectoral or radial distribution
- Diagnosis
- Clinical
Below, in Figure 1, you will find an image of a patient with episcleritis.


Figure 1: episcleritis
- Treatment
- Self-limiting
- Symptom relief
- Topical corticosteroids
- Oral NSAID
Rheumatoid arthritis presenting with scleritis
- Mechanism
- Inflammation of sclera
- Vasodilation of superficial and deep episcleral vessels
- Characteristics
- Most common cause of scleritis
- Can present before onset of joint symptoms
- Bilateral in 40-50% of patients
- Anterior Scleritis
Figure 2 shows a non-necrotizing scleritis.

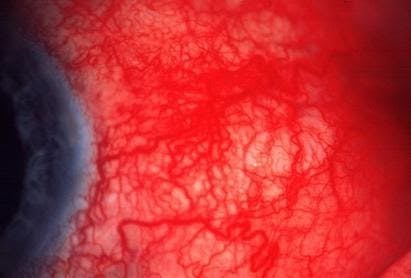
Figure 2: non-necrotizing scleritis
- Pain made worse with eye movement
- Blurry vision
- Photophobia
- Tearing
- Posterior Scleritis
- T-sign on B-scan
In Figure 3, you will find an example of T-sign with fluid in Tenon space on B-scan

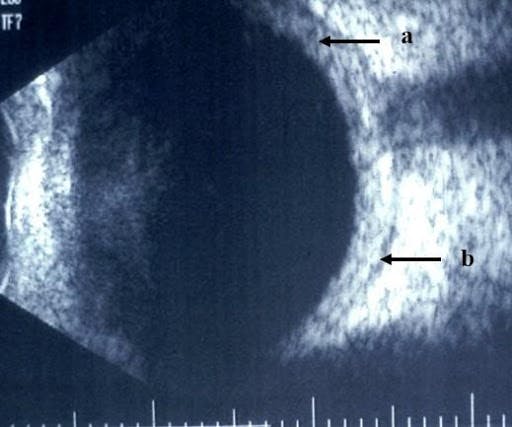
Figure 3: T-sign with fluid in Tenon space on B-scan
- Complication
- Retinal detachment
- Chorioretinal folds
- Scleromalacia Perforans
Figure 4 demonstrates scleromalacia perforans.

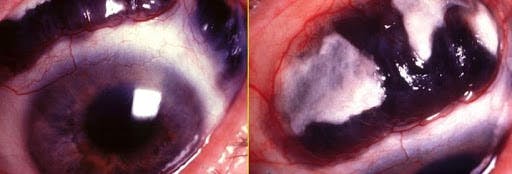
Figure 4: scleromalacia perforans
- Severe anterior necrotizing scleritis without inflammation
- Painless
- Complications
- Visual loss
- Astigmatism
- Globe perforation
- Treatment
- Topical therapy ineffective
- Need to manage systemic RA
- Medications
- Oral NSAID
- Corticosteroids
- Methotrexate
- Azathioprine
- Mycophenolate mofetil
- Cyclosporine
- Biologics (infliximab, adalimumab, rituximab, anakinra)
- **Co-management with rheumatologist is essential
- Necrotizing scleritis
- Debridement
Rheumatoid arthritis presenting with peripheral ulcerative keratitis (PUK)
- Mechanism
- Immune complexes infiltrate vascular arcades in the corneal periphery
- Characteristics
- Corneal melt
- 35% of cases occur secondary to RA
- Complication of Necrotizing scleritis
- Stromal thinning
- Secondary overlying epithelial defect
- Neovascularization of corneal periphery
- Crescent shaped juxta-limbal ulcers
- Symptoms
- Pain
- Photophobia
- Tearing
- ↓ visual acuity (induced irregular astigmatism, corneal opacity)
- Complications
- Corneal perforation
- Treatment
- Topical therapy usually ineffective as a cure
- Need to manage systemic RA
- Systemic corticosteroids best
- Ocular support
- Topical medroxyprogesterone
- Topical acetylcysteine
- Oral tetracycline
- Amniotic membrane or corneal glue in some cases
- Diagnosis
- Common Lab Findings
- ↑ Rheumatoid factor
- ↑ HLA-DR4
- ↑ Anti-cyclic citrullinated antibody (most specific)
- ↑ Cytokine Th17
- ↑ CRP
- ↑ ESR
- Common Lab Findings
- Management
- As above, based on effected segment of eye
Sjögren's syndrome1,6-13
Sjögren's syndrome - epidemiology
- Disease
- Incidence: 7 per 100,000 person-years
- Female::male: 9-14::1
- Prevalence: 42 per 100,000
- Female::male: 9::1
- Age (Average)
- 56
- Incidence: 7 per 100,000 person-years
Sjögren's syndrome - mechanism
- Chronic autoimmune inflammation characterized by diminished lacrimal and salivary gland function
Sjogren's syndrome - presentation
- General Disease
- Dry eye
- Dry mouth
- Constitutional symptoms
- Ocular
- Dry eye
- Burning
- Sandy-gritty sensation
- Ocular irritation, fatigue
- Pain
- Fluctuating blurry vision
- Pressure sensation behind the eye
- Severity
- Mild
- Dry eye
- Moderate
- Variable corneal or conjunctival staining
- Mild debris in the tear film
- ↓ tear breakup time
- ↑ tear osmolarity
- Abnormal Schirmer test (below 5mm)
- Severe
- Severe punctate corneal erosions
- Filamentary keratitis
- Significant conjunctival vital dye staining
- Low Schirmer levels (may be 0mm)
- Significantly ↑ tear osmolarity
- Mild
Sjögren's syndrome - diagnosis
ACR/EULAR Classification Criteria for Primary Sjögren's Syndrome
| Item | Weight/Score |
|---|---|
| Labial salivary gland with focal lymphocytic sialadenitis and focus score => 1 foci/mm2 | 3 |
| Anti-Ro/SSA positive | 3 |
| Ocular staining score => 5 (or van Bijsterveld score =>4) in at least one eye | 1 |
| Schirmer test => 5 mm/5 minutes in at least one eye | 1 |
| Unstimulated whole saliva flow rate <= 0.1 mL/minute | 1 |

Sign Up To Keep Reading
Grab the remaining study guide notes on Sjogren syndrome and seronegative arthropathies by signing up for free!

Check out the other study guides in this series!
References
- Schwartz T, Keenan R, Daluvoy M. Ocular Involvement in Rheumatoid Arthritis. American Academy of Ophthalmology. https://www.aao.org/eyenet/article/ocular-involvement-in-rheumatoid-arthritis. Published November 17, 2016. Accessed April 11, 2021.
- Kemeny-Beke A, Szodoray P. Ocular manifestations of rheumatic diseases. Int Ophthalmol. 2020;40(2):503-510. doi:10.1007/s10792-019-01183-9
- Cross M, Smith E, Hoy D, et al. The global burden of rheumatoid arthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1316-1322. doi:10.1136/annrheumdis-2013-204627
- Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE. Is the incidence of rheumatoid arthritis rising?: results from Olmsted County, Minnesota, 1955-2007. Arthritis Rheum. 2010;62(6):1576-1582. doi:10.1002/art.27425
- Hunter TM, Boytsov NN, Zhang X, Schroeder K, Michaud K, Araujo AB. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004-2014. Rheumatol Int. 2017;37(9):1551-1557. doi:10.1007/s00296-017-3726-1
- Hunter TM, Boytsov NN, Zhang X, Schroeder K, Michaud K, Araujo AB. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004-2014. Rheumatol Int. 2017;37(9):1551-1557. doi:10.1007/s00296-017-3726-1
- Qin B, Wang J, Yang Z, et al. Epidemiology of primary Sjögren's syndrome: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74(11):1983-1989. doi:10.1136/annrheumdis-2014-205375
- Shiboski SC, Shiboski CH, Criswell L, et al. American College of Rheumatology classification criteria for Sjögren's syndrome: a data-driven, expert consensus approach in the Sjögren's International Collaborative Clinical Alliance cohort. Arthritis Care Res (Hoboken). 2012;64(4):475-487. doi:10.1002/acr.21591
- Hernández-Molina G, Nuñez-Alvarez C, Avila-Casado C, et al. Usefulness of IgA Anti-α-fodrin Antibodies in Combination with Rheumatoid Factor and/or Antinuclear Antibodies as Substitute Immunological Criterion in Sjögren's Syndrome with Negative Anti-SSA/SSB Antibodies. J Rheumatol. 2016;43(10):1852-1857. doi:10.3899/jrheum.151315
- Daniels TE, Cox D, Shiboski CH, et al. Associations between salivary gland histopathologic diagnoses and phenotypic features of Sjögren's syndrome among 1,726 registry participants. Arthritis Rheum 2011; 63:2021.
- Whitcher JP, Shiboski CH, Shiboski SC, et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren's Syndrome International Registry. Am J Ophthalmol 2010; 149:405.
- Van Bijsterveld OP. Diagnostic tests in the Sicca syndrome. Arch Ophthalmol 1969; 82:10.
- Navazesh M, Kumar SK, University of Southern California School of Dentistry. Measuring salivary flow: Challenges and opportunities. J Am Dent Assoc 2008; 139 Suppl:35S.
- Jhaj G, Kopplin LJ. Ocular features of the HLA-B27-positive seronegative spondyloarthropathies. Curr Opin Ophthalmol. 2018;29(6):552-557. doi:10.1097/ICU.0000000000000525
Zagora SL, McCluskey P. Ocular manifestations of seronegative spondyloarthropathies. Curr Opin Ophthalmol. 2014;25(6):495-501. doi:10.1097/ICU.0000000000000098
