Optometrists handle serious ocular disease and stressful urgent cases daily. Fortunately, some patients will only have cosmetic complaints and inquire about
cosmetic eyelid surgery.
Optometrists are responsible for patient education,
making appropriate referrals, and co-management with ocular surgeons. This ensures patients avoid complications and achieve the most ideal results from cosmetic eyelid surgery.
Overview of cosmetic eyelid surgery
Blepharoplasty often comes to mind when discussing cosmetic eyelid surgery, but there are other methods that can restore fullness to the midface and eyelids for a healthy and youthful appearance.
This optometrist’s guide to cosmetic eyelid surgery will go beyond
blepharoplasty and explore adjunctive and alternate cosmetic procedures, both surgical and non-surgical, that are used today to achieve precise outcomes.
Surgical cosmetic procedures
1. Upper eyelid blepharoplasty
According to the
American Society of Plastic Surgeons, blepharoplasty was the second most common plastic surgery procedure performed in the United States in 2020.
1 Current approaches to upper eyelid blepharoplasty have evolved with more appropriate tissue removal and augmentation in restoring the eyelids to appear balanced with a youthful upper eyelid topography.
Indications for upper eyelid blepharoplasty:
- Increased laxity and/or excess skin (dermatochalasis): Loss of elastin and collagen results in skin laxity and rhytids (wrinkles), causing increased skin folding over the eyelid crease.2
- Shift of upper eyelid fat: Part of the maturing process involves the change of upper eyelid fat volume, with an increase in the nasal fat pad and an atrophy in the central fat pad.2
- Subcutaneous eyebrow fat volume loss: Eyebrow fat pad volume loss causes the eyebrow to deflate and sag, creating eyebrow ptosis.2
- Temporal eyebrow descent: The gradual loss of muscle tone of the frontalis muscle, responsible for elevating the eyebrow, and progressive bony change of the orbit causes the descent of the eyebrow, especially in the temporal region.2
- Excessive bulging in the lateral third of the upper eyelid: Excessive bulging in the lateral third of the upper eyelid may be caused by increased orbital fat and/or lacrimal gland prolapse.3
Contraindications for upper eyelid blepharoplasty
Upper eyelid ptosis
Patients with dermatochalasis can also have blepharoptosis or upper eyelid ptosis. Even after successful upper eyelid blepharoplasty, the upper eyelid will still droop from an unrecognized ptosis. Upper eyelid ptosis should be repaired at the time of upper eyelid blepharoplasty surgery.
Ruling out any ptosis not attributed to aging is essential, as blepharoplasty may not be indicated in ptosis with separate etiologies, such as neurological ptosis. Such ptosis should be referred as necessary.4
After eliminating any neurological causes for upper eyelid ptosis, the two main contraindications for upper lid blepharoplasty are systemic disease and dry eye disease (DED). However, psychiatric history, smoking, and
alcohol and drug abuse should be considered additional risk factors for complications.
5Systemic disorders
Prevention of postoperative complications, such as retrobulbar hemorrhage, includes uncovering predisposing factors of hypertension,
vascular disease, renal disease, and bleeding disorders.
3Patients should be medically cleared to discontinue Rx or over-the-counter (OTC) antiplatelet or anticoagulant medication for 2 weeks preoperatively and 1 week postoperatively.5
Dry eye concerns
Patients with preexisting
dry eye disease and inadequate Bell’s phenomenon are at risk for postoperative lagophthalmos and exposure keratopathy. Undiagnosed thyroid ophthalmopathy will present postoperatively as lid retraction and keratopathy.
4Post-laser in situ keratomileusis (LASIK) patients should wait 6 months before considering upper eyelid blepharoplasty.5
Complications of upper eyelid blepharoplasty
Chemosis
Conjunctival edema can develop in the early postoperative period as the result of incomplete eyelid closure,
ocular allergy, or surgical edema. Any keratopathy caused by chemosis is managed with standard ocular lubricants.
6Dry eyes
Upper eyelid edema and trauma disrupts tear production and blink completion, which can cause or exacerbate dry eye. Dry eye symptoms can be managed with established
dry eye protocols.
6Hematomas
Eyelid hematomas or bruising should resolve in 7 to 10 days with the use of ice compresses.6
Ptosis
Ptosis during the intermediate period, past 6 weeks, is not unusual and occurs because of edema or ecchymosis. This normally resolves over time with cold compresses.
6 Eyebrow ptosis
Sometimes, patients seeking blepharoplasty are affected by eyebrow ptosis more than dermatochalasis. Commonly, eyebrow droop is a minor secondary finding with primary dermatochalasis.
Using an eyebrow lift as an adjunctive procedure with blepharoplasty is advantageous to sculpt and elevate the eyebrow to balance the area aesthetically. Glabellar myoplasty, endoscopic eyebrow lift, and internal browpexy are just a few of the numerous procedures available.14
Lagophthalmos
Early lagophthalmos is treated with ocular lubrication and lid massage. Lagophthalmos of less than 2 to 3mm is expected to resolve with time.6
Incision issues
Incision issues typically show up at least 6 weeks postoperatively as a late complication.
Incision-related problems consist of the following:
- Wound dehiscence: Often arises laterally along the thicker skin when the incision is closed with a running suture. This concern can be avoided with different suturing techniques during surgery.2
- Hypertrophic scarring: Hypertrophic scarring on the upper eyelid is rare. If the incision remains raised and firm following blepharoplasty, gentle massage of the incision may help soften the scar. Intralesional injection of triamcinolone acetonide with or without 5-fluorouracil, a chemotherapy agent, is commonly used in the treatment and prevention of scars.2
- Hyperpigmentation: Temporary or post-inflammatory hyperpigmentation may occur along the incision line, especially in darker-skinned patients. Topical hydroquinone is frequently prescribed for the treatment of hyperpigmentation.2
Corneal abrasions
Abrasions can result from corneal drying or injury during surgery, and the patient will have the usual
corneal abrasion symptoms of decreased vision, pain, foreign body sensation, and light sensitivity. Treatment with antibiotic ointment should resolve most abrasions within 24 hours.
6Infection
The development of infection is uncommon, but if present, it should be treated aggressively, as infection can lead to visual loss. Any signs of infection should be referred immediately.6 Infection starts as preseptal cellulitis, affecting tissue anterior to the orbital septum. Preseptal cellulitis is identified only by swelling and redness of the eyelids. A very slight decrease in visual acuity can occur if the weight of the swollen eyelid affects the cornea.6
In comparison to preseptal cellulitis, postseptal or orbital cellulitis encompasses many possible indicators, with pain upon eye movement being the hallmark for diagnosis. Patients generally complain of extreme ocular pain and will show a marked decrease in visual acuity. In addition to redness and inflammation of the eyelid,
conjunctivitis, and chemosis is usually present, with proptosis and pupil abnormalities appearing occasionally.
6Eyelid sloughing
Eyelid sloughing, or necrosis, is a fairly rare consequence of infection after trauma, such as eyelid blepharoplasty. The eyelid tissue starts as red and inflamed skin and then evolves into bullae, which are fluid-filled bumps that can drain, and eventually, the surface turns into dark plaques.7
Meanwhile, the patient is in a significant amount of pain. Immediate treatment with intravenous antibiotics and debridement of necrotic tissue is imperative. If the infection is not managed properly or if the necrosis is widespread, reconstructive eyelid surgery would be necessary.7
Globe perforation
Serious complications can arise from globe perforation, such as:6
- Corneal perforation,
- Hypertensive or hypotensive globe
- Intraocular hemorrhage
- Retinal tear or detachment
- Traumatic cataract
Retrobulbar hemorrhage
Retrobulbar hemorrhage is most likely to occur in the first 2 to 3 hours after surgery, with 96% occurring within the first 24 hours after surgery. It is characterized by significant orbital pain or pressure, decreased visual acuity, an
afferent pupillary defect, and extraocular muscular restriction during entrance testing.
Other indicators, such as proptosis, chemosis, and subconjunctival hemorrhages, can be seen by gross visual inspection. Further testing may detect elevated intraocular pressure (IOP) and intraorbital pressure in patients with a retrobulbar hemorrhage.6
Risk factors for retrobulbar hemorrhage include:2
- Hypertension, vascular, and renal disease
- Anticoagulation/antiplatelet medication use
- Postoperative vomiting or coughing
- Physical activity
Vascular complications
Vascular events can cause catastrophic complications, such as complete and permanent vision loss. They occur from embolization following facial and periocular injection. This can cause infarction of the area leading to soft tissue necrosis or a
central retinal artery occlusion (CRAO).
11 Vascular complications occur when there is increased intraorbital pressure caused by retrobulbar hemorrhage and/or an acute angle closure crisis (AACC) causing increased IOP, which produces a central retinal artery and/or vein occlusion.
Hypertension, anticoagulant use, and other cardiovascular disorders are risk factors, which is expressly why they are contraindicated in blepharoplasty surgery.12
More frequently, embolization occurs with injections of foreign substances, such as soft tissue/dermal fillers, either concurrently with blepharoplasty or alone. Injection pressure differences cause retrograde migration of a foreign substance from peripheral arterioles into the ophthalmic arterial system proximal to the central retinal artery and subsequent movement of the substance anteriorly, causing a blockage. The factors that influence this mechanism include filler type, particle size, amount of filler used, and injection location.11
Vision changes
Blurred vision is a common complaint after upper eyelid blepharoplasty. Procedures of the upper eyelid can alter the pressure on the cornea and change corneal curvature, thereby altering corneal refraction and causing blurred vision.
Studies have shown that this effect is minimal, and visually insignificant, and any mild corneal curvature changes resolve in 1 to 3 months. As a result, blurred vision is mostly attributed to temporary dry eyes and resolves with
dry eye treatment. More persistent blur is commonly due to corneal edema, which may take up to three weeks to resolve.
13Acute angle closure crisis
The development of an
acute angle closure crisis is a rare but severe complication after oculoplastic surgery that optometrists should be aware of as we are in a position to recognize patients with narrow angles and alert the surgeon to prevent AACC. Also, being able to identify the signs and symptoms of AACC allows for early treatment and minimizes the chance of permanent vision loss.
Signs and symptoms of AACC
AACC is a true ocular emergency characterized by significant ocular pain, nausea, vomiting, headaches, halos around lights, reduced vision, corneal edema, conjunctival injection, and a mid-dilated pupil.8
Surgical factors provoking AACC
The pathological mechanisms of AACC, specifically after blepharoplasty, indicate the typical AACC triggers and risk factors, such as age, Asian ethnicity, and
hyperopia. Regarding AACC after periorbital procedures, pupillary dilation is considered the most significant risk factor.
9 Surgical factors that provoke pupil dilation include pharmacological mydriasis, dark adaptation, and patient distress.
9Pharmacologically induced mydriasis results in postoperative pupillary dilation with either local or general anesthetic solution. Diffusion of local anesthetic solutions, such as epinephrine, lidocaine, and anticholinergic drugs, may increase or prolong the effect of mydriatic agents leading to prolonged pupil dilation.8
Pupil dilation occurs as dark-adapted eyes are covered under postoperative dressing, ice, and/or cold compresses.9 Anecdotally, a patient's stress or anxiety has been reported to be aggravating factors.9
AACC presentation after surgery
Most AACC cases do not present immediately after surgery, but between the first and fifth postoperative day. AACC during the immediate postoperative period, within 2 days, is likely due to the local anesthesia wearing off.8 Later presentations might be attributed to a higher anxiety state or eye coverings because of putting a cold compress on the eyes.9
Furthermore, an intermittent subacute form of
glaucoma could precede the complete anterior chamber closure. In this subacute form, the anterior chamber angle is not completely blocked; instead, the blockage is intermittent.
9AACC treatment protocol
As a quick review, the AACC treatment protocol aims to eliminate pupil block, lower IOP, reduce inflammation, and relieve patient symptoms of pain, nausea, and vomiting.10
Relieve pupil block
Pupil block can be alleviated by applying corneal indentation or having the patient lie in a supine position.10
Lower IOP
Using a cocktail of topical medications, one from each pharmacological classification can be highly efficient in lowering the IOP.10 A topical alpha-adrenergic agonist, such as apraclonidine 0.5%, lowers the IOP by inhibiting aqueous production. Apraclonidine is contraindicated in patients with cardiovascular concerns; brimonidine 0.2% can be used in its place.10
A topical beta-adrenergic antagonist, like timolol 0.5%, should be added. Timolol is contraindicated in patients with pulmonary disorders; betaxolol 0.5% is the alternative drug of choice if timolol is not advised.10 The addition of a carbonic anhydrase inhibitor (CAI), topical, oral, or IV, is the next ingredient in this recipe; brinzolamide 1%, dorzolamide 2%, acetazolamide 500mg, or methazolamide 100mg are a few options.
Note that acetazolamide and brinzolamide should be avoided in patients with sulfonamide allergies and renal or hepatic impairment. Instead, oral methazolamide can be used in patients with kidney problems.10
A topical miotic, such as
pilocarpine 1% or 2%, should be used strategically; initially, pilocarpine should not be used unless the IOP is lower than 40mmHg. It can be used later on, say 1 hour later, only if the IOP has lowered to below 40mmHg.
10Finally, an oral or IV hyperosmotic agent should be administered if available. Oral glycerol or isosorbide and IV mannitol are a few hyperosmotic agents that can be used to lower the IOP. Diabetic patients should be given isosorbide instead of glycerol, while mannitol should be avoided in patients with renal failure, heart failure, pulmonary problems, or severe dehydration.10
Reduce inflammation
Optometrists can prescribe
topical corticosteroids, for example, prednisolone 1% or loteprednol 0.5%, for patients to reduce inflammation.
10Relieve symptoms of pain, nausea, and vomiting
To relieve symptoms of pain, nausea, and vomiting in patients with AACC, optometrists can use oral analgesics and antiemetics.10
2. Lower eyelid blepharoplasty
The current philosophy of
lower eyelid blepharoplasty concentrates on eyelid shaping, periorbital contouring, and blending the lid-cheek junction so that the lower eyelids appear fuller and more natural. For that reason, discussing lower eyelid blepharoplasty must involve the midface, which is the lower lid/cheek complex.
15Indications for lower eyelid blepharoplasty
- Lower eyelid dermatochalasis: Develops over time with excess and wrinkled skin that is loose and saggy.15
- Orbital fat prolapse: Orbital fat prolapse or herniation of the orbital fat in the lower eyelids, orbital fat deflation, separation, and protrusion of different fat compartments creates depressions and folds.16
- Laxity of the lateral canthus: Leads to a vertically elongated lower eyelid and the appearance of downturned eyes.15
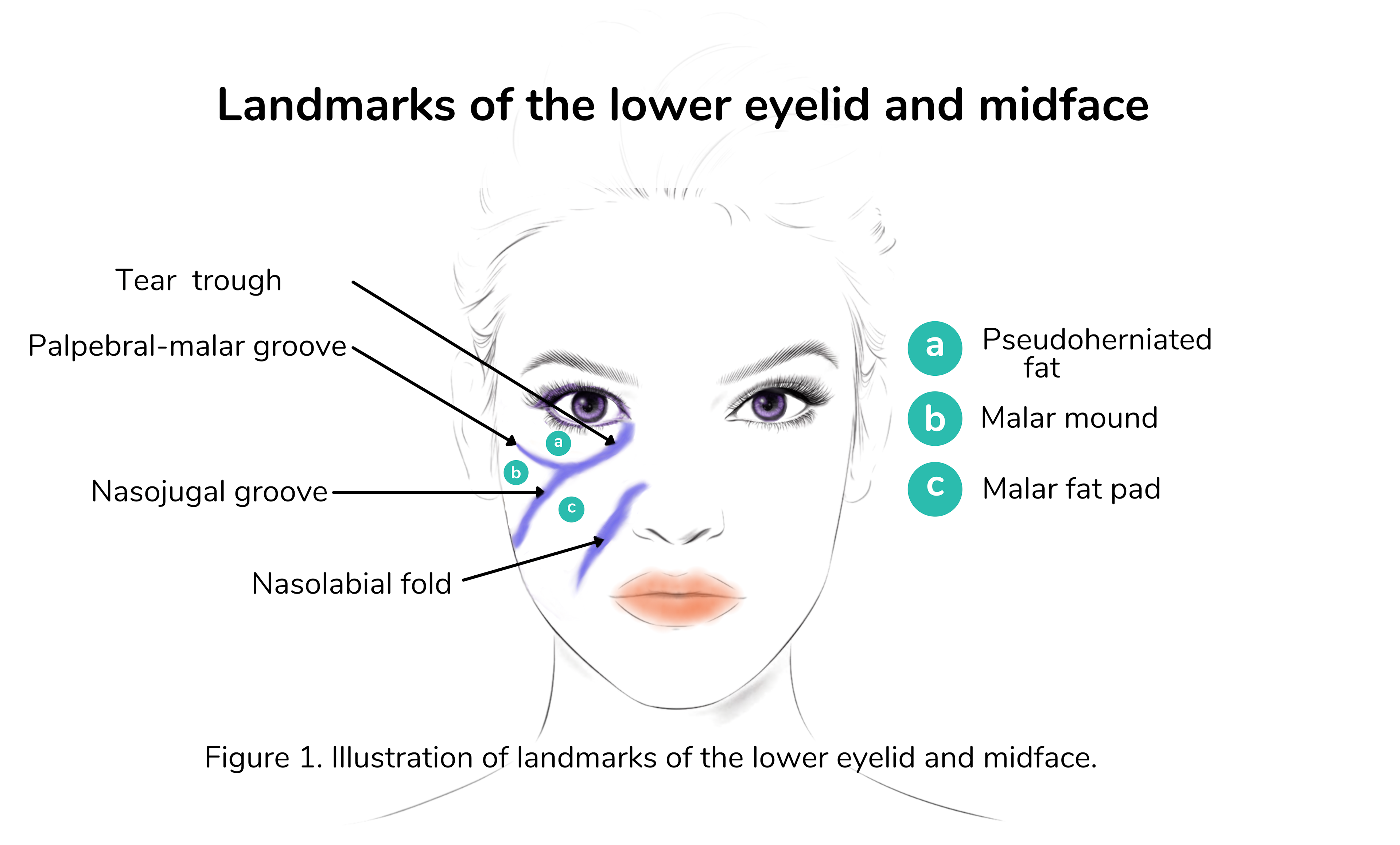
- Midface descent: The cheek or malar region descends, the infraorbital and malar area loses volume, and the nasojugal groove becomes pronounced with aging, culminating in the development of the look of “bags under our eyes.”16
Figure 1 highlights an illustration of landmarks of the lower eyelid and midface.16
Figure 1: Courtesy of Cindy Hui, OD.
Lower eyelid blepharoplasty contraindications
It is critical to identify patients with predisposing factors that put them at risk for lower eyelid retraction, namely, globe proptosis, high myopia,
thyroid ophthalmopathy, horizontal eyelid laxity, and hypoplasia of the malar eminence (upper cheekbone). Otherwise, the usual contraindications in upper eyelid blepharoplasty are identical to lower eyelid blepharoplasty.
6Lower eyelid blepharoplasty complications
Problems are similar to those in upper eyelid blepharoplasty, but the most significant visual complication specific to lower lid blepharoplasty is strabismus.
Diplopia is a rare but potentially disabling complication of lower blepharoplasty. Cyclotropia and hyperopia may arise due to extraocular muscle injuries, which ordinarily appear early on, immediately to 1 week after surgery. Additionally, patients can experience intermittent diplopia, secondary to an abnormal tear film, muscle contusion, or hematoma typically.
6The inferior oblique muscle separates the medial and central fat pads, and if the muscle is injured or trapped by the fat pads during surgical manipulation, torsional diplopia results. If injury results from damage to the inferior rectus or its attachments, hypotropia occurs.6
The hope is that the diplopia will resolve without the need for surgical intervention; therefore conservative care, such as stick-on prisms, is recommended for up to 6 weeks postoperatively.
6 Usual
prismatic corrections are inadequate in torsional situations, and occlusion treatment might be one of the last non-surgical options. Otherwise, past 6 weeks, persistent diplopia, particularly torsional cases, requires careful surgical intervention.
6Other complications of lower eyelid blepharoplasty involve:
- Eyelid malpositions causing corneal exposure: Postoperative lower lid malposition is the most prevalent eyelid displacement concern as results can vary, ranging from mild inferior scleral show to severe cicatricial ectropion.6
- Lacrimal system dysfunction: Epiphora can result secondary to dry eye, exposure keratopathy, or an impaired lacrimal pump.6
Non-surgical periorbital procedure: Injectables
1. Botulinum neurotoxin injections
Injectable Botulinum neurotoxin (BoNT) has been used for esthetic purposes for over 20 years, with serotype A being the most potent and popular BoNT type used commercially. BoNT’s mechanism of action is based on blocking the release of acetylcholine from the presynaptic nerve terminals, which interferes with muscle contraction.
BoNT begins to take effect within 24 to 72 hours and reaches maximum effect within 7 to 14 days. Its effect on striated muscle for facial wrinkles lasts about 3 to 4 months.17
Indications for BoNT
BoNT injection is approved for the treatment of wrinkles in certain areas such as the forehead, glabella (often referred to as #11 lines), lateral canthus (crow’s feet), eyebrow, nasal sidewall, and the infralid region.18
Contraindications for BoNT
BoNT injections are absolutely contraindicated in
pregnant and breastfeeding mothers, as well as children under 12 years old. Patients with coagulopathies and neuromuscular disorders such as myasthenia gravis, Eaton-Lambert syndrome, and amyotrophic lateral sclerosis are not good candidates for BoNT injections.
17In addition, a thorough medication history must be taken with patients considering BoNT, as several are contraindicatory. Neurotoxins should be administered with caution in patients taking medications, such as aminoglycosides, tetracyclines, polymyxins, penicillamine, anticholinesterases, and calcium channel blockers.
These medications can theoretically alter conduction at the neuromuscular junction.17 The use of anticoagulants, aspirin, vitamin E, and NSAIDs should be discontinued 2 weeks prior to injection.17
Complications of BoNT
Some common side effects of BoNT injections include ecchymosis, erythema, edema, pain related to the injection, and headache. BoNT injections can produce muscular weakening, which can lead to localized facial paralysis. For example, injections of the lateral canthal lines that are overly aggressive can result in drooping at the corner of the mouth.
Dry eyes, allergic reactions, and distal spread causing botulism are possible complications. The duration of these undesirable outcomes is limited since its effects wear off after 12 weeks.
17 Providers should also be aware of biofilm formation. This is the accumulation of microorganisms that are stuck to each other and/or a surface. Infection from biofilm is an unusual complication that can develop.
19 2. Soft tissue/dermal fillers
Soft tissue or dermal fillers have become a popular non-surgical treatment option for the periocular area. Dermal fillers add volume and support, filling and lifting deficient areas such as the upper cheekbone area that deflates and descends with age.
Facial wrinkles and scars can be smoothed out with fillers, and contouring of smaller sites, such as the lips or the eyebrow, can enhance features to bring back more balance and proportion to the mature face.20 The pliability, amount of lift, durability, and resistance to heat or enzymes can be adjusted by modifying the type and amount of the dermal agent used.
Hyaluronic acid fillers are most widely used in the periocular region due to their ease of injection with smaller needles, favorable safety profile, and reversibility with hyaluronidase, if necessary.20 Calcium hydroxylapatite (CaHA), autologous fat, polymethyl methacrylate (PMMA), poly-L-lactic acid (PLLA), collagen, fibroblasts, and platelet-rich plasma (PRP) are other types of injectable fillers.21
Indications for soft tissue or dermal fillers
Common targets of fillers include the nasojugal folds, temporal region of the face, lateral temporal cheek, periorbital hollows, malar, inferior malar, and zygomatic areas. The eyebrow area is a favorite site for injection, as filler can lift the lateral edge of the eyebrow tail, and enhance overall eyebrow contour and volume.21
Contraindications for soft tissue or dermal fillers
Both systemic and ocular diseases can serve as contraindications. Dermal fillers should not be used in patients with
active autoimmune diseases, including rheumatologic and thyroid disease. Acne, rosacea, and other infectious or inflammatory skin conditions that compromise the epithelial skin barrier may promote infectious or biofilm reactions to dermal fillers.
A history of herpes simplex virus (HSV) outbreaks may mandate pre and post-treatment with antiviral prophylaxis. Finally, usual care and management should be taken with patients on anticoagulant therapy as this will increase the risk of bleeding and hematoma formation.11
Certain procedures, such as dental cleaning and immunizations, should be separated by a period of time from dermal injection if they have the potential to disrupt the epithelial barrier. Some practitioners verify with patients that certain procedures be performed no less than 1 week prior to treatment.11
Complications of soft tissue or dermal fillers
Edema/fluid build-up
Due to the hydrophilic nature of HA filler, patients can experience swollen eyelids for 2 to 3 weeks after the procedure. Ecchymosis and hematoma formation are not uncommon.21
Infection/biofilm
Biofilms can cause delayed nodule formation and infection. Persistent inflammation, increasing pain, erythema, or fluctuance should prompt
antibiotic therapy and drainage.
21Tyndall effect
Visible material associated with a gray or blue color, called the Tyndall effect, may be detected at the injection site. Since this effect is prevalent with most fillers, clinicians can decrease the incidence of the Tyndall effect by adjusting injection depth, varying particle sizes, or considering different products.19
Nodules
Noninflammatory nodules can develop and resolve with time. Some particles of different HA formulations, such as PMMA beads, do not resorb, and chronic nodules must be surgically excised.11
Allergic reactions/hypersensitivity/inflammatory reactions
Redness and abnormal swelling can occur immediately or may appear weeks, months, or years after treatment.
11 Most acute responses can be alleviated with oral antihistamines and oral steroids if the former is not effective. Delayed hypersensitivity reactions to HA require extensive management.
Oral steroids and oral antibiotics that have anti-inflammatory actions (doxycycline or tetracycline) are considered standard protocol. Intralesional steroid and hyaluronidase injections can be used on patients who do not respond to oral therapy, but they come with their own set of potential side effects, such as skin atrophy. To rule out other etiologies, such as sarcoidosis or infection, delayed-onset nodules or lesions should be biopsied by a specialist.22
Migration
The filler may travel immediately, months, and even years after injection. Hyaluronidase injections are extremely beneficial in situations when filler migration results in a magnification of unanticipated effects.11
Vascular events
Embolism from the soft tissue injection can create vascular events leading to infarction/soft tissue necrosis and
CRAO-related vision loss. The single most significant factor in preventing vascular complications is proper injection technique, which involves using smaller gauge needles, digital pressure, needle tip positioning, and a slower injection rate. Once identified, vascular compromise should be treated urgently with unexpired materials from an emergency filler complication kit.
19Non-surgical periorbital procedures: Resurfacing treatments
1. Dermabrasion/microdermabrasion
The technique of dermabrasion/microdermabrasion entails mechanically removing layers of skin using abrasives. It is a superficial treatment and results in less discomfort, risk, and recovery time than other procedures, such as laser resurfacing.23
Indications for dermabrasion
Dermabrasion/microdermabrasion can be used to smooth out acne scars, fine lines, and wrinkles. Skin changes due to sun exposure and hyperpigmentation can also be improved.23
Contraindications for dermabrasion
Dermabrasion/microdermabrasion should be avoided in patients with active acne,
rosacea, and active use of isotretinoin. Patients with unstable diabetes,
autoimmune disorders, or a recent HSV outbreak should refrain from this procedure.
23Complications of dermabrasion
Complications are usually secondary to irritation caused by the aluminum oxide abrasive crystals, the most common being eye irritation. The crystals can adhere to the corneal epithelium, causing superficial punctate keratitis, chemosis, injection, photophobia, and tearing.23
2. Chemical peeling/resurfacing
Chemical peels expose younger skin beneath by removing layers of skin using chemicals such as glycolic acid, trichloroacetic acid (TCA), salicylic acid, lactic acid, and phenol in varying concentrations. The most commonly used peels for the periorbital region are TCA 30%. TCA peels are commonly performed intraoperatively after lower lid blepharoplasty.24
Indications for chemical peels
Chemical peels are used to treat acne, acne scars, actinic keratosis, melasma, and wrinkles. Chemical peels can be used in the periorbital region to provide significant improvement in skin texture and tightening and in the infraorbital region to treat under-eye darkening.24
Contraindications for chemical peels
- Chemical peels are contraindicated in pregnant individuals.24
- Immunosuppressed patients, patients with a current or recent HSV, bacterial, or fungal infection should avoid chemical peels.24
- Patients with a history of hypertrophic or keloid scars, post-inflammatory hyperpigmentation, poor wound healing, and regular indoor or outdoor tanning are not good candidates for chemical peel procedures.24
- Current use of minocycline, nicotine, oral contraceptives, and oral isotretinoin is contraindicated.24
- Phenol-based peels are contraindicated in patients with cardiac, renal, or hepatic disease.24
Complications of chemical peels
Chemical peels can cause erythema, infections, peeling, and transient hyperpigmentation. Stronger peels cause prolonged redness, delayed wound healing, scarring, ectropion, and hypo- or hyperpigmentation. HSV can also be reactivated.24
3. Fully ablative laser resurfacing
Fully ablative lasers, such as CO2, Er:YAG, and plasma, vaporize the entire epidermis as well as a portion of the dermis, resulting in clinical improvement of periocular wrinkles and skin tightening. It can be used in conjunction with blepharoplasty or by itself. Fully ablative resurfacing provides significant improvement following one single treatment.
25 Indications for fully ablative laser resurfacing
Photoaging, such as pigmentation and actinic keratoses, can be treated with fully ablative laser resurfacing. Laser resurfacing is very effective for periorbital wrinkles and fine wrinkles in the cheek area. Skin laxity and deeper creases can be greatly improved secondary to the general tightening effect of the laser.25
Contraindications for fully ablative laser resurfacing
Fitzpatrick skin phototypes IV to VI are not recommended for fully ablative laser resurfacing because they are susceptible to dyspigmentation afterward. Fitzpatrick skin phototype IV is skin that rarely burns and tans more than average. Skin phototype V is brown skin, and phototype VI is Black skin.26
Fully ablative laser resurfacing is contraindicated in patients with a history of keloids, connective tissue diseases, such as rheumatoid arthritis,
lupus, and scleroderma, and diseases with koebnerization, (the appearance of new skin lesions on previously unaffected skin secondary to trauma), such as psoriasis or vitiligo.
Also, patients who have had radiation therapy, a facelift, blepharoplasty, or other surgical procedure that undermines the skin, should wait at least 6 months before considering fully ablative laser surgery. It is generally recommended that patients who have had oral isotretinoin therapy wait for 1 year before undergoing a fully ablative laser procedure. Previous oral isotretinoin therapy has been associated with atypical scarring even after 1 year of isotretinoin cessation.25
It is now standard practice to use antiviral prophylaxis in all patients undergoing laser resurfacing, regardless of HSV history.25
Complications of fully ablative laser resurfacing
The most common complications from fully ablative laser resurfacing are:
- Acneiform eruptions25
- Dyspigmentation and post inflammatory hyperpigmentation25
- Eczematous dermatitis25
- Edema and erythema25
- Infections25
- Scarring25
4. Microfocused ultrasound
Microfocused ultrasound (MFU) devices (Ultherapy, Ulthera, Mesa, Arizona) are another non-invasive modality utilized for lifting and tightening the periorbital area. MFUs act by depositing points of micro thermocoagulation at specific depths into the dermis, creating discrete points of skin contraction, promoting skin tightening and improving wrinkles. Improvement may not be observed until 12 to 24 weeks post-treatment. and the full effect of lifting and tightening may take up to 6 months to occur.
27 MFU with visualization
MFU with visualization (MFU-V; Ultherapy Merz North America, Raleigh, NC) enables real-time imaging of tissue layers allowing the clinician to confirm appropriate depth of treatment, avoid treatment of non-target tissue, and tailor the focal depth and energy of the emitted ultrasound therapy for individual patients.28
Indications for microfocused ultrasound
MFU is approved for lifting the eyebrow, neck, chin, and the treatment of lines and wrinkles of the décolletage. MFU treatments are beneficial to patients prone to post-inflammatory hyperpigmentation and mild-to-moderate skin laxity with normal wound healing responses.
MFU-V has also been used off-label as an effective procedure for improving infraorbital skin laxity.
27Contraindications for microfocused ultrasound
Metallic implants, such as pacemakers or defibrillators, should not be near the treatment area.27 Precautions should be taken when using MFUs directly over keloids, implants, and permanent dermal fillers.27
Pregnant women should be managed with caution.
29 Also, patients with active infections, active or severe cystic acne, and any open skin lesions should be rescheduled.
27 Complications of microfocused ultrasound
Normally, initial pain subsides after treatment, with tenderness in the area and possible bruising afterward. Redness and dermal edema are typical and mostly decrease after a few days; however complete resolution can take up to 4 weeks. Thermal damage can produce complications such as burns, blisters, welts, and grid lines on the skin, which can later result in scabbing, scarring, or post-inflammatory hyperpigmentation.27
Neural injuries with heat can cause burning, stinging, paresis, or numbness. In addition, severe ocular damage from heat can produce iris injury, zonular damage, cataract, and acute increases in IOP, if applied improperly.30
Ocular protection during periocular procedures
It goes without saying that ocular protection should be used during periocular procedures. Having patients close their eyes during minimally invasive cosmetic procedures fails to supply the necessary standards of protection.31
Ocular shields, constructed to fit properly over the patient’s eyes, should be worn during dermabrasion/microdermabrasion sessions to prevent the exfoliating crystals from entering the eyes and during chemical peels to prevent inadvertent splashing of fluid.31
The use of laser-impenetrable and wavelength-specific eyewear ocular shields is one of the fundamental methods of preventing the absorption of damaging light/laser. Corneal shields, much like
contact lenses, are designed to fit correctly under the eyelids. When using nonablative fractional lasers, laser aids (disposable adhesive eye protectors) are an alternative that protect the periocular region while still allowing access to the brow and infraorbital area.
31In closing
There are numerous approaches to blepharoplasty in cosmetic eyelid surgery, with many alternatives that allow for tailor-made protocols for each individual patient.
Optometrists are in the position to educate patients about cosmetic eyelid surgery and
collaborate with surgeons to deliver the highest quality of care.