As eyecare providers, we are acutely aware that dry eye disease is one of the most common eye disorders we routinely encounter, with
nearly 16 million people in the US affected by the condition.
1 Dry eye is also a growing problem due to lifestyle changes, such as
increased screen time.
2 Additionally, we are all familiar with the fact that dry eye is a multifactorial problem, with numerous contributory factors.
3 Due to this multifactorial nature, it is vital to
listen to each dry eye patient’s individual issues stemming from the condition to help ascertain what specific factors are contributing to the patient’s dry eye complaints.
However, an oft-overlooked factor in dry eye disease is the psychological aspect of the condition. These psychological elements can be just as significant as the physical manifestations of dry eye, so they must also be addressed to completely treat a patient’s disorder.
To do so, we must provide thorough education, set expectations, address any psychological barriers, understand patients’ perceptions of their condition and treatment, and be cognizant of any potential challenges or obstacles that may prevent successful treatment.
Educating patients on dry eye disease
Addressing the psychological components of dry eye begins with education. When an established patient returns for a dry eye exam or you have a new patient coming in specifically for a dry eye evaluation, it is vital to allocate the proper amount of time in your schedule. In our clinic, we allot a significant amount of time for our dry eye exams, especially the initial evaluation.
The rationale behind these extended exam slots is to allow for ample time to talk to the patient about their individual experience, as previously mentioned, as well as time to review their test results together and thoroughly provide patient education regarding their diagnosis and treatment.
Provide an overview of the disease and potential treatment plans
As part of our evaluation, we perform meibography, noninvasive tear breakup time (NIKBUT), tear meniscus evaluation, and lipid layer thickness analysis via interferometry. We then discuss each test and its results in detail and how it pertains to their condition and symptoms.
Next, we describe each element of their treatment plan and the component of their dry eye that it addresses. By the time we have finished with the exam, the patient should know what dry eye is, exactly why they are experiencing their individual signs and symptoms, and how each part of their treatment plan is going to help. This experience leaves the patient feeling empowered and hopeful.
It is much easier to confront a problem when you understand it clearly and we see this play out routinely. It also helps tremendously with compliance, which ultimately determines outcomes.
We often hear from patients that a previous doctor prescribed a treatment, but they stopped using it because they “didn’t know what it was doing.” This illustrates how even the best treatment plans can ultimately fail if the patient education piece is missing.
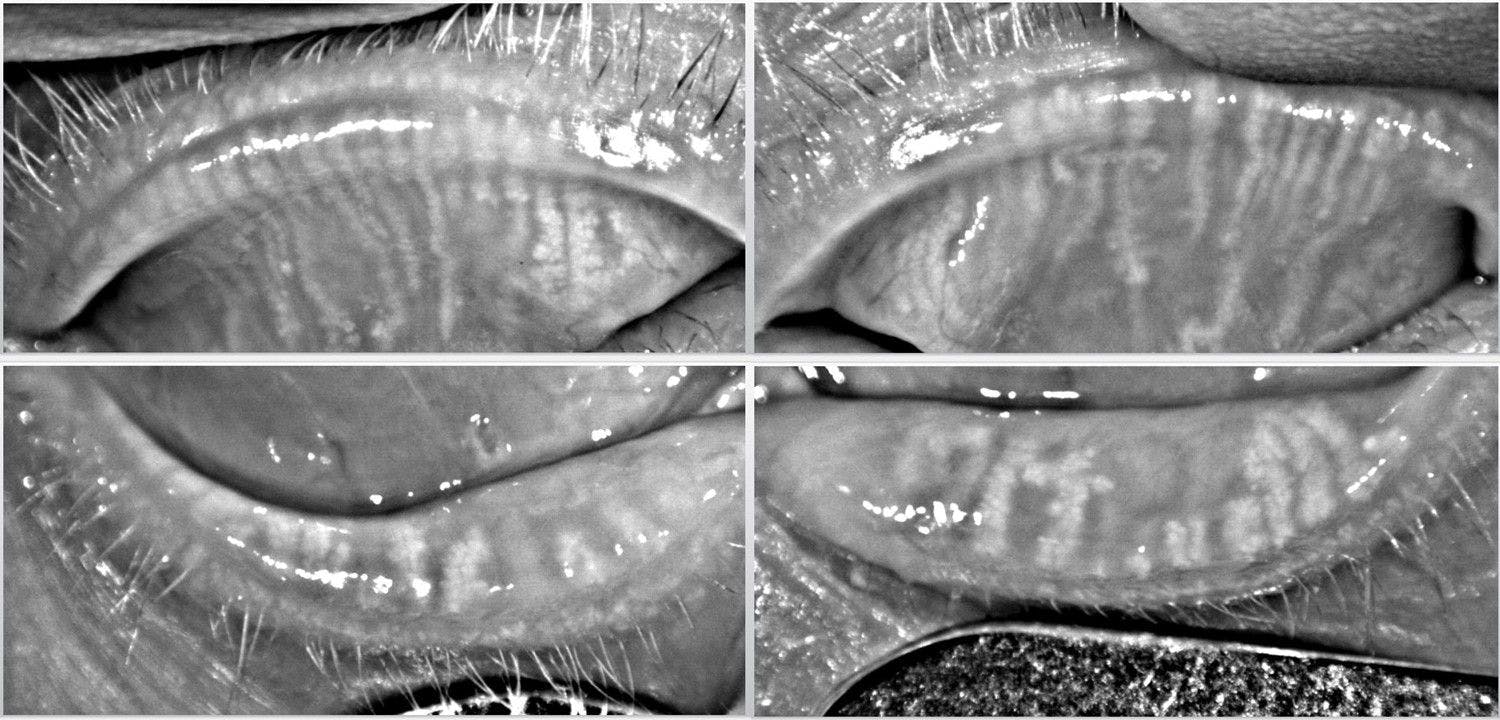
Patient education is a key component to successful dry eye treatment. Utilizing testing and imaging such as meibography to show patients their own meibomian glands can be a powerful educational tool. When a patient sees an image of their own glands, it has a much greater impact than a verbal explanation of MGD or a representative image.
Figure 1 demonstrates the Meibomian glands of a dry eye patient.
Figure 1: Image provided by Cory Lappin, OD, MS, FAOO
Scheduling time for education is key
We routinely hear our patients tell us that we have spent more time with them than any previous doctor, and they are so grateful that we took the time to listen and explain everything to them. Therefore, by providing appropriate time, not only have you provided a rare experience for the patient, but you have also established trust and a sense that you truly care for their well-being.
Setting clear expectations with your patients
Setting expectations is a critical and nuanced element of the psychological side of dry eye treatment. However, when we mention setting expectations, the default mindset is often to “pull back” on what a patient should expect from their treatment, but this is not always, nor should it always be, the case.
Many dry eye patients we encounter often harbor a defeatist mentality toward their condition and treatment. Prior experiences typically drive this mindset.
Most dry eye patients have seen multiple doctors, been on numerous treatments, and have spent large sums of money, all with modest to no improvement. These patients tell you “I have tried everything, and nothing helps.” This mindset can be incredibly detrimental to a patient’s success. They go into treatment expecting failure, and failure-in often results in failure-out.
The impact of having a hopeful mindset
This begs the question, if the patient truly believes nothing will help, then why did they come to see you? This is because, despite all their doubt, their symptoms are so disruptive to their lives that they understand they need to try something, and deep down, even at an unspoken subconscious level, they harbor some hope that you are the one who can help them. It is our job to rekindle this hope.
This does not mean we make unrealistic promises or guarantee we will fix all their problems within a week and they will never experience any eye discomfort again. Instead, it means we communicate to the patient that we understand how difficult their situation is, that we have successfully helped many patients just like them and that we will do everything in our power to improve their dry eye. And if we hit any roadblocks, we will not give up but keep trying until we can find a solution.
Doctors make a common error when treating dry eye when we use the statement “There is nothing else we can do.” This statement essentially signals to the patient you are waving the white flag of surrender—there is nothing else that can be done and they will just have to live with their dry eye. This leaves the patient with a sense of abandonment and defeat.
A much better philosophy when roadblocks occur is to openly and honestly explain to the patient that despite everything we have tried, we have not yet gotten the results we want, but we are not giving up, and we will continue to treat their condition as best we can. This turns the message from one of defeat into one of hope.
Thankfully, we are entering a “golden age” of dry eye care where
innovations, medications, and treatments are constantly being developed. So, letting these patients know there are more treatment possibilities on the horizon, that sometimes the biggest element of treatment is purely time, and that you will be with them every step of the way reassures them.
And ultimately, what many patients desire is reassurance. Giving them this peace of mind that they will not be abandoned can go a long way in providing comfort, even when going through the most difficult stretches of their condition.
Explaining the reality of treating a chronic and progressive condition
The other aspect of setting expectations falls in line with the more traditional sense of the phrase. Dry eye is a chronic and progressive condition. It develops over a long period but often presents suddenly.
It likewise requires a significant length of time to address this damage and improve signs and symptoms. Letting patients know early on in the treatment process that relief may not be immediate is vital. Disappointment often stems from unmet expectations.
Therefore, we want to ensure patients have the same treatment expectations as we do to avoid any disappointment or discouragement that may arise if expectations are not discussed and set. Also, it is equally important to set expectations for patients doing well and not experiencing any significant dryness-related issues.
Every dry eye patient, no matter how well managed, will experience a flare in symptoms from time to time, whether due to environmental stressors like changes in weather or a self-induced flare due to a laxness in treatment. In these cases, it is helpful to pre-emptively warn patients that even though they are doing well currently, it is likely that at some point their symptoms will flare up again.
However, when this occurs, they need not panic or worry that their eyes will revert back to how they were at the start of treatment, but rather that they just will need some extra care, such as a short course of steroids, to get them through the flare and back to their improved state.
Addressing dry eye patient fears
When setting expectations, there is one specific scenario that warrants mentioning. Many dry eye patients, often more than you would expect, fear that they will eventually lose some of their sight or go completely blind.
This is especially true amongst dry eye patients who experience transient blurred vision or reduced acuity due to
tear film instability and corneal surface disruption. Knowing that it is exceedingly rare outside of the most severe cases of dry eye and ocular surface disease for significant vision loss to occur, it is easy for us as ECPs to dismiss the notion of such a concern as implausible.
But from the patient’s lived experience, their dry eye has caused a reduction in the quality of their vision, so from their perspective, it is only logical that if their condition continues to worsen, so too will their vision.
So, if you start specifically addressing this issue and asking patients if they are worried about their dry eye leading to blindness, you will be surprised by the number who admit it is something they worry about.
Most people fear blindness more than the loss of hearing, memory, speech, limb, heart disease (the leading cause of death), and even premature death itself, so it is no surprise this fear is a significant source of psychological distress.4-6 Consequently, it can be a major relief and comfort to reassure patients that their dry eye will almost certainly not lead to blindness, especially when receiving the proper care.
Guilt, stress, and depression
Dry eye, like most chronic conditions, can take a significant psychological toll. Though dry eye can be mild, in its severe forms it can completely disrupt a patient’s life.
Patients with severe dry eye may be unable to work, especially with jobs involving heavy computer or screen use, participate in hobbies they once enjoyed (like sewing or hiking), or may even experience reduced independence as they struggle with driving due to fluctuating vision or extreme discomfort when maintaining sustained visual focus.
This can have a tremendously negative impact on a patient’s quality of life. So, it is no surprise that depression is highly associated with DED.7,8 It is not unusual for dry eye patients to directly state that their condition has made them depressed. As previously noted, these patients may also feel unheard and helpless.
In our clinic, the average dry eye patient has usually seen 2 to 3 doctors specifically for their dry eye before coming to our practice. Sometimes, patients state their concerns were dismissed or downplayed, or they were given artificial tears or punctal plugs and told that was “all that could be done.”
With every subsequent failed treatment, they develop a sense of helplessness that feeds into a major psychological component of their dry eye. These patients come to expect failure, so it is critical for us as their doctors to provide hope grounded in proper diagnosis, education, and treatment.
Reassure patients that struggle with feelings of guilt
In some cases, dry eye patients may also exhibit a high degree of guilt associated with their condition. Dryness commonly arises after many ophthalmic surgeries including refractive procedures, like LASIK, or after
cataract surgery.
9,10 As these procedures are voluntary (though often necessary in the case of cataracts), patients experiencing post-operative dryness often exhibit remorse over having chosen to have the procedure performed. They carry the psychological burden that, to some extent, their dry eye was self-inflicted.
It is critical to address this mentality as part of their overall treatment. These patients need reassurance that they did nothing wrong in seeking out these procedures, as they are performed countless times every day and often without issue.
They were simply seeking to improve their vision, but unfortunately, they are experiencing
dryness as a side effect. It is helpful to openly address and acknowledge this feeling of guilt and regret, but then redirect the focus to what can be done to help them in the present.
By offering the appropriate reassurance, education, and treatment, we can help shift their thoughts from dwelling on the past to looking forward to a future where their lives are no longer controlled by their dry eye symptoms.
Stress-induced exacerbation of dry eye disease
While dry eye can induce psychological distress, the inverse is also true. Psychological stress can take a physical toll and can exacerbate pre-existing ailments, especially chronic conditions, and dry eye is no exception.11-13
Patients experiencing acute psychological stress, like the illness or loss of a loved one, may report a worsening of their dry eye symptoms. It is helpful to discuss this relationship with your dry eye patients, and it can be beneficial to suggest seeking care with a mental health professional in addition to their dry eye treatment plan to ensure all elements of their well-being are properly addressed.
Another specific scenario is pain associated with DED and ocular surface disease. While dry eye involves irritation and discomfort by nature, the pain and symptoms experienced by the patient may not be entirely attributable to their dry eye.For example,
stress-induced exacerbation, as mentioned in the previous section, may or may not respond to conventional dry eye therapy.
Signs that you may be dealing with pain not directly related to the patient’s ocular surface status is a patient showing improvements in objective testing with symptoms remaining nonresponsive to treatment, especially treatments that typically provide broad relief, such as topical steroids.
Treating dry eye symptoms with psychological or nervous origins
A quick and easy way to evaluate if such pain is directly related to dry eye or some other indirect cause is to administer topical anesthetic in-office and ask the patient if they feel an improvement in their symptoms. If no improvement is noted, this suggests there is an alternative cause of their pain and discomfort as any pain rooted in ocular surface disruption should improve with the instillation of anesthetic.
For such instances, the issue may be nerve-related, such as
in the case of neuropathic pain (often described as “pain without stain” or pain of nervous origin as opposed to pain directly derived from ocular surface disruption), rather than being caused by traditional dry eye.
In these cases, co-management with a pain specialist may be helpful. Suppose the patient reports significant psychological stress or fixation on a specific issue and displays no improvement as described even with anesthesia. In that case, referral to a mental health specialist may also be beneficial.
Patients may ask you “So is the pain all in my head?” It is important to address this question appropriately by carefully explaining that just because the pain is psychological, that does not mean the pain is not “real” or that they are not experiencing it, but rather the source of the pain is not entirely caused by their dry eye.
It must also be mentioned that dry eye patients may discuss self-harm or suicidal ideation due to the disruptive nature of their disease. These are serious situations that all ECPs providing dry eye care will encounter at some point throughout their career.
These patients require interdisciplinary care and must be referred to a licensed psychiatrist, psychologist, or emergency room. In many states, physicians are legally obligated to report such cases of potential self-harm.14-16 Therefore, ECPs must be prepared to appropriately handle these situations should they arise.
Patient perception
Patient perception is another key element of the psychological component of dry eye treatment. As discussed, it is not unusual for some dry eye patients to harbor a defeatist mentality, and therefore their natural disposition is to expect failure.
In many ways, this is almost a form of self-defense for the patient, as they have had hope that previous treatments would improve their dry eye. When the treatments failed to do so, the disappointment only compounded an already difficult situation. Therefore, this expectation of failure can be a preemptive coping mechanism to protect against feelings of disappointment.
Focus on asking about specific details of the treatment plan
This presents a clinical challenge as such patients may be less likely to notice or allow themselves to notice improvement, especially when initial improvement can be subtle. Therefore, it can be helpful to
ask about specific trouble areas, such as the frequency of symptoms or artificial tear use, to allow for a more concrete assessment of how a patient is doing.
We have our techs review the patient’s previous symptoms, frequency, and intensity before we see the patient. It is not unusual for a patient to initially report that they have not seen any improvement, only to realize upon reviewing their specific symptoms and trouble areas one by one that they are reduced or improved, such as needing to use artificial tears less frequently.
So, when you hear statements like “Everything is the same,” “It’s no better,” or “Nothing is working,” it is useful to always ask about specifics, so patients can see individual areas of improvement and struggle rather than just lumping all their issues together.
Don’t shy away from highlighting the results of objective testing
Another critical component affecting the patient's perception of treatment and progress is objective testing, such as noninvasive keratography break-up time (NIKBUT) or lipid layer interferometry.
It is one thing to tell patients that their ocular surface looks better subjectively. When you can show them results that can be directly compared to previous tests, it has a much greater impact as they can objectively see the improvement. Providing this concrete data is very helpful in demonstrating progress, especially for more analytically-minded patients.
It is also not uncommon for objective testing to improve before symptoms, so you may be asked “If everything looks better, then why don’t I feel better?” In such cases, we reassure patients it is not unusual for improvements in symptoms to lag behind improvements in signs, and that their results are a positive indicator that we are headed in the right direction and that it may just
take more time or a tweak to their treatment plan to get them to where their improvement in symptoms matches their improvement in testing.
Be cautious about taking this to an extreme by over-emphasizing objective testing results while completely ignoring the patient’s perception. Taking a “Well, your numbers look better, so that’s that” stance can be detrimental to a patient’s perception of treatment because, ultimately, how the patient feels is the most important factor and objective testing is only part of the greater picture. So, acknowledge the patient’s feelings while reassuring them with exam results, but do not discredit their experience.
When taking this approach, we often hear patients ask some form of the question “So I am doing better?” when shown improvement in their objective testing results. And for many, it is almost posed in a way as though they are asking for permission to allow themselves to feel better. They have been so accustomed to treatment failure that sometimes they need to see and hear that their dry eye is improving before they finally let themselves fully believe it.
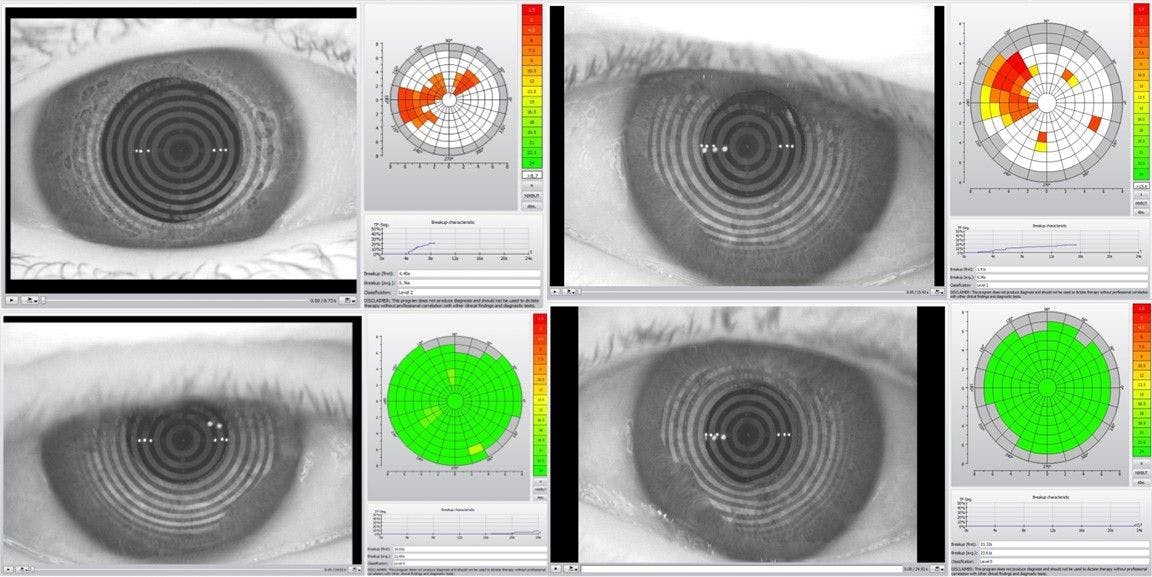
The ability to show patients objective improvements in their dry eye, such as their tear break-up times from before and after treatment, can have a profound impact on their perception of their progress. These objective measurements can help make improvements much more tangible.
Figure 2 shows NIKBUT test results from a dry eye patient.
Figure 2: Image provided by Cory Lappin, OD, MS, FAOO
Embrace asking targeted questions
From the doctor’s perspective, there is also a major psychological element to dry eye treatment as well. Dry eye can be a challenging condition to treat. When you hear from a patient that they are not improving, or treatment is not working despite your best efforts, this experience can be equally discouraging and frustrating.
However,
assessing specific areas of a patient’s symptomology, such as improvements in nocturnal dryness or epiphora, and/or looking at objective testing results helps create a clearer picture of a patient’s status. Starting with very broad questions can help create an overall picture of the patient’s condition and once you have initiated treatment, more targeted questions focusing on their individual areas of struggle often yield more useful information.
For instance, if you ask a patient broadly, “Are you feeling better?” they may respond “No.” But, if you ask, “Do your eyes feel as gritty as they used to when you wake up in the morning?” that same patient may respond that they no longer experience that symptom as frequently or intensely.
In such an example, you've gone from a patient you perceived to be failing in their treatment to one that is improving in some areas but still needs other parts of their symptomology addressed.
Taking this approach can also prevent ECPs from falling into the trap of abandoning or constantly changing treatment plans because the feedback they are receiving from a patient is that their treatments are not working. In actuality maybe all but one or two elements of the treatment regimen are providing improvement. Therefore, asking for specifics will also help make more focused and direct changes to a treatment plan, as opposed to an often-unnecessary wholesale shift in the direction of treatment.
This will also prevent the feeling that you as the doctor have “tried everything,” as you now have a more focused approach and are looking at treatments and problems as individual elements rather than one monolithic condition with an indivisible treatment plan. Additionally, always ask for clarification and discuss conditions from a relativistic reference point, especially when patients give broad or general statements.
If an established patient says “My eyes are feeling worse,” an appropriate response would be “Are they worse than the last time I saw you or worse than your first visit? And what specifically feels worse?” They may then respond by explaining that they feel much better than when they first were evaluated but not as good as the last visit, and their eyes have been burning more recently
since the weather has changed in the summer. Now you know the regression in their symptoms is relatively minor, as they are still doing better than when they started treatment.
Additionally, it is likely they are experiencing an exacerbation of symptoms due to increased environmental challenges associated with a change in weather, and, therefore, they may only need a small adjustment to their treatment plan to get them through the summer months as opposed to sweeping changes.
Objective testing data can also prevent ECPs and patients alike from becoming discouraged by a perceived lack of improvement. Many times over the course of dry eye treatment, a patient’s improvement in symptoms lags behind an improvement in signs. In such cases, if no testing data is available to show any objective improvement, it can be easy to feel as though no progress is being made.
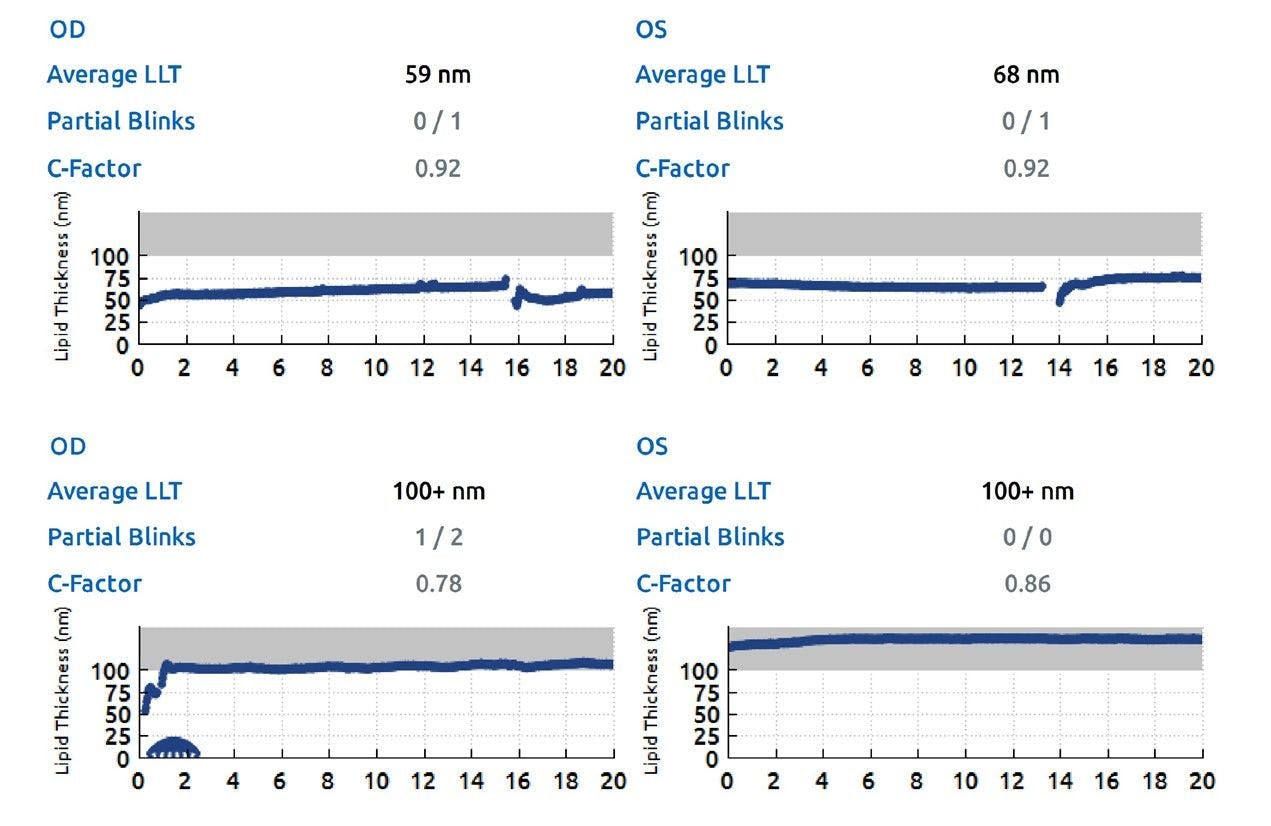
However, suppose testing, such as lipid layer interferometry, shows an increase in lipid layer thickness, for example. In that case, it can be an encouraging sign that progress is being made and further improvement may just require more time or a tweak in treatment, but the patient is on the right path.
Figure 3 illustrates the lipid layer interferometry of a dry eye patient.
Figure 3: Image provided by Cory Lappin, OD, MS, FAOO
Potential challenges
From all that has been discussed, it is readily apparent that the psychological mindset of a patient is critical to their success or failure during dry eye treatment. However, there are some mentalities that provide greater challenges than others.
Helping patients who struggle with compliance
One of these mindsets that ECPs are most familiar with is the patient who struggles with compliance. These patients will often report no improvement but at the same time will also report using few or even none of their prescribed treatments.
While the best way to improve compliance is through education, both about a patient’s condition and how each element of a treatment plan will specifically address their individual issues, in some cases these patients still struggle with compliance even with proper education. In these instances, even though it seems obvious, remind the patient that their dry eye cannot improve if they do not use their treatments.
Additionally, always ask if there are any specific reasons they are not using or are unable to use their prescribed treatments, as their noncompliance may simply stem from a misunderstanding or the inability to tolerate certain therapies.
Sometimes, these patients are looking for a “silver bullet” that will fix all their symptoms at once, so the notion of being on a long-term treatment, especially multiple long-term treatments, is difficult for them to accept.
They may even tell you that it is just too much, and they feel like they shouldn’t need to be on all these treatments to get better, despite the reality of their condition. For these patients, it may be beneficial to just
focus on one or two treatments even though they will not address everything, but often something is better than nothing.
Connecting with patients who self-treat
Similar in mentality to the patient who struggles with compliance is the patient that ends up treating themself. This patient will listen carefully to the treatment plan, seemingly be on board, but when they come back in they did something entirely different. Unlike the traditionally noncompliant patient who does not utilize their therapies, self-treating patients tend to use treatments, but they are just not the ones prescribed and therefore may not be the best option for them.
A common trend among patients with this mindset is a desire to try everything or switch to something new if a prescribed treatment does not seem to be effective quickly enough. Again, education can be helpful for these patients.
Reminding them why each prescribed treatment was selected and reassuring them that it can take time for a therapy to work can help the patient stick to the prescribed plan. Also, it is helpful to explain that abruptly changing, adding, or removing treatments creates “noise” in assessing the effectiveness of their treatment regimen.
By constantly altering what they are using, it is difficult to ascertain what is actually helping and what is not. So, by adhering to the agreed-upon treatment plan, they can make it easier to accurately determine the appropriate therapies.
However, it is important to note patients will often also have a rationale for why they changed their treatment, so this is an opportunity to listen as they may describe a symptom or issue they are experiencing that you were previously unaware,
for which you may be able to provide a solution.
The pros and cons of dry eye support groups and forums
The nature of the self-treating patient segues into a specific area of note in dry eye treatment, online dry eye support groups and forums. These forums are often a double-edged sword. At best they can provide support and a sense of shared experience and community, at worst they can be a source of confusion, misinformation, frustration, and even despair.
Dry eye patients tend to be a relatively informed population in regard to their disease, as their symptoms drive them online to research and
seek out treatments that will provide relief. This often leads to these dry eye support groups. Here they will encounter numerous accounts of individual experiences involving everything from established prescription treatments to potentially harmful home remedies. And without the proper knowledge or guidance, this can send patients down a rabbit hole of misinformation.
Patients who constantly self-change their treatment often visit these forums, as the experiences of others encourage them to try something similar. However, we need to remind our patients that dry eye is multifactorial and that no two dry eye patients are exactly the same, so a treatment that works for one patient may not work for another and vice versa.
Additionally, our patients may encounter individuals posting on these forums who have given up or lament that they have “tried everything” with no relief, which can negatively impact their outlook on their own treatment prospects. Therefore, it is helpful to ask your dry eye patients if they visit these forums or groups to help them avoid the pitfalls associated with their unguided use.
Working with a combative patient
Another challenging attitude is the combative dry eye patient. A combative attitude often stems from frustration over their condition, leading the patient to challenge or question your treatment plan or even your diagnosis.
However, it is important to note this is different from an inquisitive patient. We should encourage patient questions, even challenging ones. The difference exists in the purpose and outcome of the questions. Questions posed out of curiosity or confusion lead to clarity. In contrast, questions and challenges lodged out of misdirected frustration create barriers to a successful doctor-patient relationship and can impede successful treatment.
For instance, when you are reviewing the treatments a patient has tried previously they may get quickly frustrated and state, even brusquely, “I have tried everything, and nothing works,” despite us knowing this is obviously not the case. However, if we stop there and just take the statement at face value because we do not want to risk aggravating the patient, we will likely miss vital information for successful treatment.
Trying to establish common ground is the best approach in these scenarios, even when it is difficult. Verbally acknowledging their frustration can ease the situation, as this goes back to the feeling many dry eye patients have of being unheard.
Also, sometimes you must remind these patients that
you are there to help them, but you can only help them if they let you. Again, a combative stance often arises from a sense of frustration over their dry eye, so listening to the patient and acknowledging their frustrations can go a long way in overcoming this challenge.
Communicating with patients about financial concerns
Financial concerns will always arise when treating dry eye and ocular surface disease, given the predominantly self-pay nature of many therapies. Often we encounter two mindsets when it comes to the financial aspect of dry eye treatment—the patient that desires to do whatever they can to treat their condition but simply cannot afford some of the recommended therapies, and the patient who can afford treatment but is reluctant to do so because cost has become the primary driver of their decision making.
Acknowledging the financial costs of treating dry eye disease
The latter mindset can be particularly challenging as these patients often become preoccupied with how much they have previously invested in treatment, and cost becomes the lens through which they view all their treatment options.
These patients will often respond with a statement such as “But I have spent so much on my eyes already” when presented with a new treatment option. Again, this is often rooted in disappointment in the outcomes of previous treatments that did not provide the level of improvement they were hoping for.
Additionally, this mindset can impact the perceived effectiveness of a patient’s treatment as their focus is shifted away from improvement in their dry eye symptoms to how much it costs to achieve this progress. Therefore, the likelihood that they will be satisfied with their treatment outcomes will be lower.
In such cases, it is helpful to openly acknowledge that dry eye can be an expensive condition and that you realize that fact and you will try your best to help find treatments that work for them both clinically and financially, however sometimes it may be unavoidable that a treatment will be costly.
For patients that frequently bring up what they have already spent, you can be empathetic but also explain that
the focus needs to be on how their eyes are doing in the present. This does not mean we should be unsympathetic or callous towards the financial situation of our patients, it just means we need to maintain our focus on offering the best treatment options available regardless of cost and letting the patient make the final decision if they wish to pursue them. However, it is crucial to never push patients into a treatment they are uncomfortable getting, especially if cost is the reason.
For self-pay treatments like IPL, we will explain to patients why the treatment makes sense for them from a clinical perspective, but reinforce that ultimately the choice to pursue the treatment is their own. This avoids the patient feeling they were “sold” a treatment rather than genuinely needing it.
In fact, we will often tell patients that we want them to wait on undergoing a treatment if they are not 100% comfortable with the decision, because we want everyone completely on board. Also, let patients know that it is okay if they need more time to think before making a decision. This again removes any pressure from the decision-making process which can help the patient become more confident in the choice they ultimately make.
Finding a balance between treatment and costs
Dealing with the financial aspect of dry eye treatment is often an area of struggle for many doctors as well, as having financial discussions with patients can be outside of their comfort zone.
Although it can be uncomfortable at first, we have found having straightforward, honest, and open conversations about the costs associated with treatment, while reminding patients that the choice to pursue any particular therapy is ultimately their own, is a successful way to navigate this challenging area.
Again, this is not to disregard the financial realities that many patients face and the fact that treating dry eye can be expensive. However, it is our responsibility to care for our patients, so we need to at least offer the treatments we believe are in their best interest, regardless of cost, and ultimately let the patient decide if they wish to pursue them.
Sometimes, patients will defer to you as the doctor, and ask if you think a treatment is necessary. In these cases, answer honestly—an approach we usually take is from the perspective of a family member, such as “If you were a member of my family, then I would recommend this treatment.”
Other times the necessity of a particular treatment is not as clear-cut, and you should communicate that as well. In these scenarios, it can be helpful to explain that it is okay to hold off on a treatment for the time being, but you will let the patient know in the future if their condition reaches the point where you think they really need it. This can help ease a patient’s mind knowing that this is not a decision they must make at this very moment.
So,
by educating our patients and providing them with all the options available, while avoiding any unnecessary pressure, we help empower them to take control of their condition and make the choice that is ultimately right for them. This can be a very helpful approach, especially when dealing with the psychological concerns that are associated with the financial aspects of dry eye treatment.
Summary
Dry eye is a common problem all ECPs encounter
day in and day out in clinical practice. However, while DED is common, it can be extremely disruptive in the lives of many. The complex nature of dry eye and ocular surface disease and how it impacts the quality of life of those affected creates a strong psychological component to the condition.
In our experience treating these patients as part of our dedicated dry eye clinic, we have found that treating the psychological aspects of DED is often just as important as addressing the physical manifestations. However, to do so successfully requires time and an ability to address the patient from a holistic perspective.
Therefore, we need to take the time to listen carefully to our patient’s individual experiences with dry eye, thoroughly examine and diagnose their specific issues, provide education, and then create an individualized treatment plan.
In addition to this fundamental treatment structure, we must also assess the patient’s psychological state to recognize any potential barriers to successful treatment, such as beliefs that their case is hopeless, that they are in some way responsible for their dry eye after undergoing elective treatment, or they have unrealistic expectations.
We must be aware of times when a patient needs interdisciplinary care, such as in cases of depression or when patients harbor thoughts of self-harm. In these instances, we must be prepared to direct these patients to the appropriate mental health professionals to ensure their entire well-being is addressed.
Conclusion
Dry eye can be a challenging and disruptive disease for our patients. However, we can provide a source of hope by delivering the appropriate care grounded not only in the proper recognition, diagnosis, education, and treatment of the condition, but also in
empathy and sincere concern for each patient’s physical, mental, and emotional well-being.