


Blepharoplasty surgery can be performed to improve vision or to enhance the cosmesis of the eyelids. This surgery is anatomically nuanced and requires much skill and experience for optimal results.
Various techniques may be utilized, including removing excess skin, muscle, or fat from the upper and lower lids. As with any ophthalmic surgery, it is important to follow certain key principles to ensure a successful outcome.
My top five clinical pearls for blepharoplasty:
1. Selecting patients for eyelid surgery
Patient selection is paramount; unfortunately, not all patients are good candidates for blepharoplasty. Patient goals and expectations should be realistic and appropriate before signing up for surgery. This is elucidated during the consultation process. For upper eyelid surgery, the goals for functional blepharoplasty (vision restoration) and cosmetic blepharoplasty differ. Going through before and after photos and demonstrating the anticipated appearance of the eyelid with a mirror and creaser instrument can help.
For cosmetic blepharoplasty, it is crucial to ensure that the patient is undergoing surgery for the right reasons. Patients should seek surgery for themselves rather than change or alter their appearance for a partner. Unrealistic expectations or body dysmorphia disorder should alert the surgeon that blepharoplasty may not meet the patient’s aesthetic goals.
Similarly, patients with uncontrolled pre-operative dry eye syndrome are not good surgical candidates and should be counseled that eyelid surgery can worsen their dry eye symptoms. Patients with systemic co-morbidities that would preclude elective eyelid surgery should be optimized by their primary care physicians before considering blepharoplasty.
Figures 1 through 4 highlight before and after photographs of four patients who underwent a blepharoplasty. The image on top is the before and the bottom image is of the patient following the procedure.


Figure 1: Courtesy of Anaïs Carniciu, MD

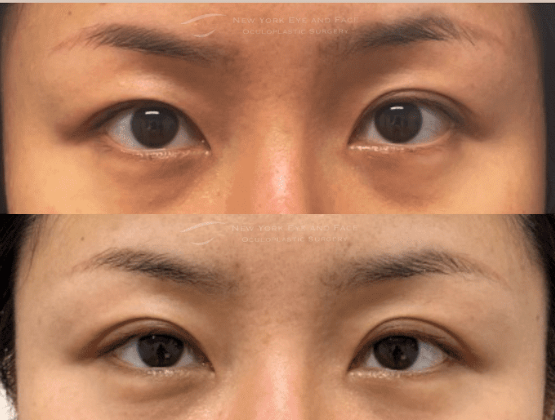
Figure 2: Courtesy of Anaïs Carniciu, MD


Figure 3: Courtesy of Anaïs Carniciu, MD


Figure 4: Courtesy of Anaïs Carniciu, MD
2. Cut once but measure twice
Measurements matter! Precise marking and measurement of the upper eyelids are crucial to achieving the desired results. Optimal results are not determined by how much skin is removed but rather by the amount of skin that remains. In general, at least 20mm of skin should remain in the upper lids to allow for proper eyelid closure and reduction of post-operative dry eye risk.
The surgeon should delineate the amount of excess skin with a surgical marker pre-operatively and verify the amount using the "pinch test" before incision. Additionally, the surgeon should measure and account for the natural height of the eyelid crease.
“Caucasian women typically have a lid crease of approximately 10mm. This value is typically less in men and in patients of Asian descent.”
The incisions for upper eyelid blepharoplasty should be placed in natural skin creases and folds to minimize scarring and should be set at an equal height bilaterally. For lower eyelid blepharoplasty, customized fat sculpting and/or repositioning should be performed as per the pre-operative measurements to avoid a hollow appearance.
3. Not all cases of ptosis can be fixed with blepharoplasty
Remember that not all “droopy lids” are equal. It is important to distinguish dermatochalasis (excess skin that can be addressed by blepharoplasty) from blepharoptosis (eyelid muscle weakness). A thorough pre-operative evaluation is necessary to determine the etiology of a “droopy” eyelid.
Check MRD1, extraocular motility, and levator muscle function in all patients undergoing blepharoplasty evaluation. Many patients have underlying blepharoptosis and require a ptosis correction procedure via levator advancement or Müllerectomy for optimal results. In a small minority of patients with blepharoptosis, identifying an underlying Horner’s syndrome or third cranial nerve (CNIII) palsy can be life-saving.
4. Avoid 2 procedures when 1 will suffice
Consider combining procedures, particularly in patients undergoing cosmetic surgery. Brow ptosis should not be confused with dermatochalasis. Temporal hooding is often due to a droopy brow rather than dermatochalasis or excess eyelid skin. In some cases, upper blepharoplasty surgery may be combined with other facial rejuvenation procedures, such as a browlift, for a more comprehensive enhancement of the upper face appearance.
Options for brow rejuvenation include stabilization procedures such as an internal browpexy, performed through the same incision as the blepharoplasty, or more robust brow lifting surgeries using direct or endoscopic techniques. Upper eyelid blepharoplasty can also be combined with the removal of herniated orbital fat from the lower eyelids (lower blepharoplasty) and/or CO2 laser resurfacing of the skin for aesthetic improvement.
5. Postoperative care is paramount to successful outcomes
Be specific about post-care instructions. Proper post-operative care is critical for ensuring a successful outcome. Provide your patients with clear written instructions on how to care for their incisions and manage any discomfort. Patients should be advised to keep the surgical area clean and avoid rubbing their eyes, swimming, or wearing makeup.
“Cold compresses and antibiotic ointments can be helpful in the immediate post-operative period for comfort and healing.”
It’s helpful to counsel patients that for the first 72 hours after surgery, the eyelids can look progressively worse from edema and ecchymoses before looking better. Providing an on-call number where patients can reach a surgeon after hours is valuable for patient reassurance and safety.
Schedule a 1-week post-operative visit as a “safety check” to ensure proper wound healing, and advise the patient that final results may take several months to be fully appreciated once post-operative edema has completely resolved.
In closing
The clinical pearls above will effectively and consistently guide ophthalmic surgeons to optimal safety and functional blepharoplasty outcomes.
