



Differentiating between a diagnosis of high myopia and high myopia with glaucoma can be confounding. Concentrating on the diagnostic norms of the highly myopic population can certainly help in accurately diagnosing glaucoma. This article will discuss these unique qualities to uncover the true diagnosis of glaucoma in high myopia.
Prevalence of high myopia in the global population
A review and meta-analysis by Holden et al. estimated that in 2020, there were 2.62 billion people with myopia, and 399 million people with high myopia. They projected that by the year 2050, the myopic population will be 5 billion, and the highly myopic 1 billion, affecting all age groups from age 10 to 79 years old. Certain regions, such as Asia and North America, had a higher prevalence of myopia and they projected regional differences would follow an overall upward trend.
The study did not take into account any myopia control interventions in their forecasted trends.1
Definition of myopia and high myopia
Currently, there is no accepted standardization regarding the classification of myopia. Different definitions of myopia and high myopia are used in studies and research, with some studies using refractive error, axial length (AL), or both. To adjust for the different degrees of myopia across the 145 studies utilized, Holden et al. defined myopia starting at a spherical equivalent of –0.50 D and a spherical equivalent of –5 D for high myopia.1
For research, clinical and health policy considerations, Flitcroft et al. proposed a standardization for myopic terminology, such as defining refractive and axial myopia, and quantifying levels of myopia. The authors suggested that low refractive myopia be specified as the spherical equivalent of –0.50 D to –6 D, and that myopia over –6 D be defined as high myopia.2 This demonstrates that there is still no consensus regarding myopia classification across academia. For clarity, this article will indicate myopia values as they pertain to each study specifically.
Association between myopia and glaucoma
Myopia has long been associated as a risk factor in glaucoma. Several large population-based studies not only confirm the association between myopia and glaucoma, but show that the correlation becomes stronger as myopia increases.3,4 In 2020, Haarmon et al. did a meta-analysis of 14 studies and found the odds ratio (OR), a statistic that quantifies the strength of the association between two values, was 1.95 for overall myopia, indicating a high correlation. In high myopia, which they defined as ≥ ─3 D, the OR was even higher at 2.92, showing that the relationship with glaucoma became even stronger as myopia increased.5
Presenting symptoms
The myopic glaucoma suspect may present just like any other glaucoma suspect patient: without any subjective complaints relating to glaucoma. The normal practice of using the objective findings in glaucoma diagnosis still apply. So if there is a known association with glaucoma, and the usual diagnostic tests are done, why is diagnosing glaucoma in a patient with high myopia so confounding?
Challenge of high myopia glaucoma suspects
Due to many factors that are specific to patients with high myopia, glaucoma is actually over-diagnosed in this population. The architecture of the myopic optic nerve head makes it difficult to evaluate. Visual field anomalies can exist in healthy myopes and if intraocular pressures are normal, the peculiarities of the highly myopic optic nerve can make a glaucoma diagnosis difficult. Understanding normative data based on high myopia diagnosis can help differentiate glaucoma and reduce errors.
Differential diagnostic factors

IOP
Even though there is a strong association between myopia and glaucoma, there is no clear evidence that intraocular pressure (IOP) alone is higher in patients with myopia; there are conflicting studies regarding this relationship. A population-based study by Wong et al. not only confirmed a cross-sectional association between myopia and glaucoma, they noted that an increasing severity of myopia was associated with progressively higher IOP by 0.85 mmHg.6(p.l214) Li et al. studied healthy high myopes and did not find any significant association between IOP, refractive error, or AL.
However, they did find a positive correlation between younger age, greater central corneal thickness, and higher IOP.7 Nomura et al. looked at the relationship between IOP and refractive error, adjusting for age and central corneal thickness. Their data reported a positive significant association between IOP and advancing degrees of myopia.8
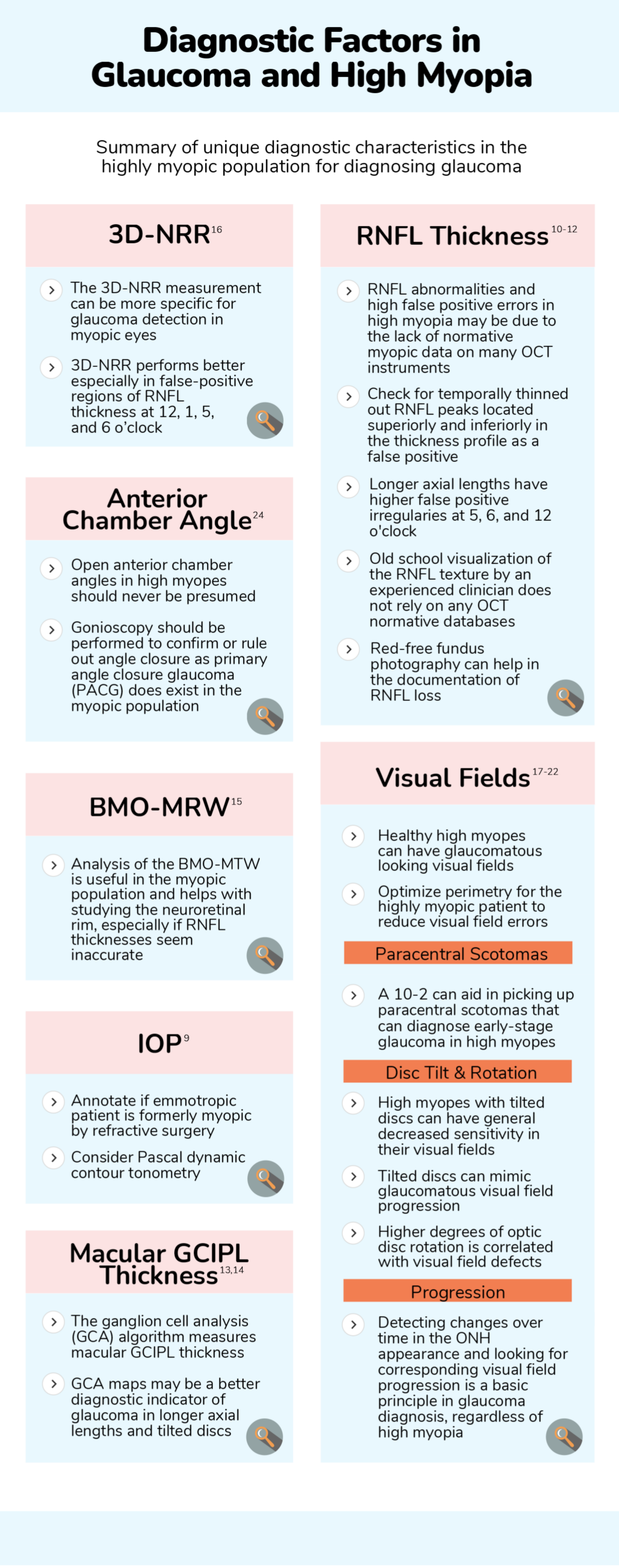
When considering IOP in a patient with high myopia, tonometry measurements may need to be annotated if the glaucoma suspect is a former patient with myopia that has had refractive surgery. Pascal dynamic contour tonometers seem to be more immune to changes in corneal biomechanics, especially after corneal refractive surgery and might be something to consider in those patients.9
RNFL thickness
Spectral-domain optical coherence tomography (SD-OCT) has become important in visualizing and quantifying the retinal nerve fiber layer (RNFL) thickness in the assessment of glaucoma, as progressive disease is characterized by loss of retinal ganglion cells and their axons in the RNFL. When compared against the normative database, highly myopic non-glaucomatous eyes have abnormally thickened RNFL temporally, but abnormally thinned out RNFL inferiorly and superiorly. This is due to superotemporal and inferotemporal RNFL bundles converging temporally with increasing degrees of myopia.
On the OCT analysis, this causes more temporally located superior and inferior peaks on the RNFL thickness profile and causes the map to be coded as “abnormal”, thus creating a false positive.10 Yamashita et al. confirmed that longer axial lengths were associated with higher rates of irregularities at 5, 6 and 12 o’clock.11
RNFL abnormalities and high false positive errors in high myopia may also be due to the lack of normative myopic data on many OCT instruments. Biswas et al. was able to import a myopic normative database into their OCT and it outperformed the normative database for detection of RNFL abnormalities in high myopes, with higher sensitivity and specificity. They felt that due to the high prevalence of myopia and false positives, that there was a definite unmet need for a myopic normative database.12
“Old school” visualization of the RNFL texture by an experienced clinician does not rely on any databases. Normal fundus examination with appreciation of striated, reflective areas, or lack thereof, can help in highly myopic eyes. Red-free fundus photography can help in the documentation of RNFL loss.
Macular GCIPL thickness
In addition to using OCT to evaluate the RNFL, assessment of the ganglion cell-inner plexiform layer (GCIPL) is of added vital importance. Rolle et al. confirmed that the ganglion cell complex is a better diagnostic indicator in longer axial lengths and should be used as a complementary test in the diagnosis of glaucoma in myopic eyes.13
Shin et al. looked at the RNFL and GCIPL in eyes with and without myopic tilted discs. Their study confirmed the glaucoma diagnostic accuracy of GCIPL parameters as they were unaffected my myopic tilted discs.14
Optic nerve head and neuroretinal rim
BMO-MRW
Visual assessment of the optic nerve head (ONH) and neuroretinal rim can be difficult in patients with high myopia due to ONH rim pallor, disc tilt or rotation, indistinct margins or peripapillary atrophy. Evaluation of the optic nerve alone is usually insufficient to diagnose myopic glaucoma. Thus, SD-OCT is widely used to detect structural changes to the ONH. In particular, OCT scans that reference Bruch’s membrane opening (BMO) and the internal limiting membrane (BMO-MRW) as anatomic landmarks, better assesses the neuroretinal rim in tilted optic nerves with oblique insertions seen in myopia.
Sastre-Ibanez confirmed that normative databases for BMO parameters should be modified for myopic eyes. Their study showed that analysis of BMO-MRW was useful in the myopic subpopulation. They noted that this data point could help with studying the neuroretinal rim, especially if global RNFL thickness seem inaccurate in a patient with moderate myopia of ≥ ─3 D.15
3D-NRR
The Cirrus HD-OCT can detect the minimum of a surface from the optic disc margin to the vitreoretinal interface based on three-dimension (3D) volume scan data. This is measured and supplemented with a color-coded map based on the internal normative database called the 3D-NRR thickness. This measurement is more specific for glaucoma detection in myopic eyes. A study in 2018 by Kim et al. demonstrated that the false-positive rate was significantly lower for 3D-NRR thickness than RNFL thickness when detecting glaucoma in myopic eyes. They noted that the 3D-NRR performed better especially in the regions where false-positive signs of RNFL thickness were most prevalent at 12, 1, 5, and 6 o’clock.16
Visual fields
Visual field defects in healthy myopes
Various visual field defects may mimic glaucomatous visual field changes. A study by Ding et al. looked at visual fields in a group of healthy young patients with high myopia in which the median age was 17.4 years with an average refractive error of –8 D. They found that 25.5% of the patients had enlarged blind spots, 23.4% had reduction in sensitivity, and 16.1% had glaucomatous-type fields, which included nasal step and arcuate defects. The group of patients that had glaucomatous type fields were given full glaucoma work ups, and only 2.1% were categorized as high-risk glaucoma patients while the rest were deemed lower risk.17
Paracentral scotomas
Studies show that there is a unique VF distribution profile of early glaucomatous RNFL damage in high myopia. Papillomacular bundle defects are usually the last nerve fibers lost in most glaucoma patients, but not in the case of highly myopic eyes. There is a higher frequency of superior papillomacular bundle defects characteristic of highly myopic eyes and therefore, paracentral scotomas in the inferior temporal quadrant occur more frequently in early-stage glaucoma.18
For high myopia, adding a 10-2 perimetry to the regular 24-2 perimetry protocol can aid in picking up paracentral scotomas that 24-2 cannot. Finding paracentral scotomas in high myopia can diagnose early-stage glaucoma.19
Disc tilt and rotation
Disc tilt and rotation in high myopia can cause visual field disturbances. Tay et al. noted that high myopes with tilted discs had general decreased sensitivity in their visual fields.20 Hung et al. felt that the degree of optic disc rotation was a more crucial factor than refractive error or axial length in predicting the presence of glaucomatous VF defects in myopic patients. Also the higher the degree of optic disc rotation correlated with higher probability of visual field defects.21
Providing the best optical correction during perimetry, either with trial lenses or contact lenses is recommended especially in high myopia. With tilted discs, Vuori et al. noted that tilted discs falsified or mimicked progression and by making refractive trial lens changes for perimetry may resolve visual field errors. They suggested giving the maximum most minus correction, or even adding –1 D, to specifically aid in high myopia with tilted discs in automated perimetry to get more reliable results.22
Visual field progression
Detecting changes over time in the ONH appearance and looking for corresponding visual field progression is a basic principle in glaucoma diagnosis, regardless of high myopia. A study by Doshi et al. followed a group of glaucoma patients and suspects over 7 years.
Of the total study population, 43% of the patients had more than –6 D of myopia. Irrespective of any IOP-lowering therapy, over the seven years, the visual fields of these patients did not progress and there were no changes in the ONH. They concluded that these patients had glaucomatous looking nerves and visual fields due to myopia alone.23
Anterior chamber angle
Open anterior chamber angles in high myopes should never be presumed. Gonioscopy should be performed to confirm or rule out angle closure as primary angle closure glaucoma (PACG) Yong et al. studied the occurrence of myopia with angle closure, which included PACG patients, primary angle closure suspects, primary angle closure, and patients with a history of acute angle closure. They discovered that 25% of the study population had myopia, of which, 29% had myopia between –2 D and –5 D, and 11% had high myopia ≥–5 D. They found that most of the patients with myopia had longer axial lengths, but anterior chamber depths were similar to the emmetropia and hyperopia groups.24
Final thoughts
Detecting glaucoma can be complicated, especially in patients with high myopia. Focusing on the diagnostic norms of the highly myopic population detailed in this article will help with precisely diagnosing glaucoma.
References
- Holden BA, Fricke TR, Wilson DA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042. doi:10.1016/j.ophtha.2016.01.006
- Flitcroft DI, He M, Jonas JB, et al. IMI - Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20-M30. doi:10.1167/iovs.18-25957
- Mitchell P, Hourihan F, Sandbach J, Wang JJ. The relationship between glaucoma and myopia: the Blue Mountains Eye Study. Ophthalmology. 1999;106(10):2010-2015. doi:10.1016/s0161-6420(99)90416-5
- Marcus MW, de Vries MM, Junoy Montolio FG, Jansonius NM. Myopia as a risk factor for open-angle glaucoma: a systematic review and meta-analysis. Ophthalmology. 2011;118(10):1989-1994.e2. doi:10.1016/j.ophtha.2011.03.012
- Haarman AEG, Enthoven CA, Tideman JWL, Tedja MS, Verhoeven VJM, Klaver CCW. The Complications of Myopia: A Review and Meta-Analysis. Invest Ophthalmol Vis Sci. 2020;61(4):49. doi:10.1167/iovs.61.4.49
- Wong TY, Klein BE, Klein R, Knudtson M, Lee KE. Refractive errors, intraocular pressure, and glaucoma in a white population. Ophthalmology. 2003;110(1):211-217. doi:10.1016/s0161-6420(02)01260-5
- Li Z, Li S, Liu R, et al. Distribution of intraocular pressure and related risk factors in a highly myopic Chinese population: an observational, cross-sectional study. Clin Exp Optom. 2021;104(7):767-772. doi:10.1080/08164622.2021.1878817
- Nomura H, Ando F, Niino N, Shimokata H, Miyake Y. The relationship between intraocular pressure and refractive error adjusting for age and central corneal thickness. Ophthalmic Physiol Opt. 2004;24(1):41-45. doi:10.1046/j.1475-1313.2003.00158.x
- Pepose JS, Feigenbaum SK, Qazi MA, Sanderson JP, Roberts CJ. Changes in corneal biomechanics and intraocular pressure following LASIK using static, dynamic, and noncontact tonometry. Am J Ophthalmol. 2007;143(1):39-47. doi:10.1016/j.ajo.2006.09.036
- Leung CK, Yu M, Weinreb RN, et al. Retinal nerve fiber layer imaging with spectral-domain optical coherence tomography: interpreting the RNFL maps in healthy myopic eyes. Invest Ophthalmol Vis Sci. 2012;53(11):7194-7200. Published 2012 Oct 17. doi:10.1167/iovs.12-9726
