From November 18 to 20, 2022, eyecare practitioners from around the world gathered online for Eyes On 2023, a 3 day educational summit offering up to 9 hours of COPE-accredited CE and CME providing the latest innovations in the ophthalmic industry.
Enjoy this presentation from Jacob Lang, OD, FAAO, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
Recent innovations in treating
thyroid eye disease (TED) have caused a shift from a “wait and see” mindset to eyecare practitioners (ECPs) adopting a more interventional approach. It’s important to note that TED and thyroid dysfunction are associated; however, they often require different treatments to manage symptoms.
This article will review how to differentiate between systemic and ocular thyroid disease and outline how to identify, diagnose, and treat patients with thyroid eye disease.
Watch the full lecture on thyroid eye disease!
Sign up for our newsletter to watch the full recording and to register for more Eyes On events.
Graves’ disease vs. thyroid eye disease
Graves' disease likely comes to mind when people think of thyroid eye disease, as it is the most common cause of hyperthyroidism.
Graves’ disease is an autoimmune condition caused by thyroid dysregulation, as autoantibodies bind to thyroid stimulating hormone receptors (TSHR), which triggers excessive production of thyroid hormones. Orbitopathy is the most prevalent and prominent manifestation of Graves’ disease, besides thyroid hormonal dysfunction.
When an endocrinologist sees a patient with Graves’ disease, the treatment aims to inhibit the production of thyroid hormones. Potential treatment options include radioactive iodine (RAI) therapy, medications to regulate thyroid production as necessary, and surgery to remove a portion of the thyroid. It has been noted that up to 50% of patients with Graves’ disease will develop TED.
Thyroid eye disease pathophysiology
Although TED often occurs in patients with hyperthyroidism, it is a distinct disease, and treating the underlying systemic thyroid dysfunction often does not resolve the ocular signs and symptoms. For example, using
Synthroid (levothyroxine sodium) to treat Graves’ disease will not resolve all of the ocular signs and symptoms.
At the root of this condition’s pathophysiology is the activation of orbital fibroblasts by autoantibodies, which leads to orbital inflammation early on in the disease and subsequent fibrosis. It’s important for eyecare practitioners to note that common dry eye disease (DED) symptoms and signs might be related to autoimmune ocular inflammation caused by TED.
The downstream effects of TED can cause subsequent ocular pathologies:
- Dry eye
- Exposure/proptosis
- Eyelid retraction: Found in 91% of TED patients
- Lagophthalmos
- Blink dynamics/frictional forces
- Ocular inflammation
- Autoimmune conditions
- Optic nerve compression
- Inflammation and fibrosis inside a confined space
- Proptosis: Found in 62% of TED patients
- Diplopia: Found in 51% of TED patients
- Extraocular muscle infiltration, inflammation, and fibrosis
Signs of thyroid eye disease
As shown above, TED can result in many symptoms that may present similarly to ocular surface disease. TED patients will likely have a resultant
dry eye because the condition is an autoimmune inflammatory disease. Symptoms ECPs should look for to determine whether the patient has ocular surface disease or TED include orbital congestion and allergic conjunctivitis without any papillary reaction that doesn’t improve with allergy drops.
Also, if unexplained changes in vision that are inconsistent with corneal changes from dryness or other pathologies are noted, this could be caused by low-grade chronic compressive optic neuropathy.
Resistance to retropulsion, an unsatisfactory response to a careful motility check, and lid lag on down-gaze can help with this diagnosis. Additionally,
optic nerve imaging with OCT and visual field testing can be helpful in these cases. Lastly, ECPs should check for temporal chemosis with injection overlying the extraocular muscles.
Thyroid eye disease risk factors
Generally, women are at higher risk than men, but men tend to have an elevated risk for more severe TED. There are two peaks of incidence for
thyroid eye disease that occur in patients between the ages of 40 to 49 and 60 to 69. Smoking increases the risk of developing TED by two- to eightfold.
The odds of developing TED increase by 17% with each decade of age progression, and thyroid reactive antibodies (TRAb) levels may correlate with prognosis. There is also a 20% risk of new or worsening TED after RAI treatment, so follow-up with patients after an RAI treatment is necessary to minimize this risk.
TED clinical activity score
Similar to the ocular surface disease index, the clinical activity score (CAS) system helps measure TED patients' symptom severity. In this system, one point is given for the presence of each of the parameters assessed, and the sum of all points defines clinical activity.
For initial consultation:
- Spontaneous orbital pain
- Gaze-evoked orbital pain
- Eyelid swelling associated with active Graves’ ophthalmopathy
- Eyelid erythema
- Conjunctival redness associated with active Graves’ ophthalmopathy
- Chemosis
- Inflammation of caruncle or plica
At the 1 to 2-month follow-up:
- Increase of >2mm proptosis
- Decrease in uniocular ocular excursion in any one direction of >8 degrees
- Decrease of visual acuity equivalent to 1 Snellen line
Labs to order to test for TED
While ECPs may instinctually lean towards ordering thyroid-stimulating hormone (TSH), triiodothyronine (T3), and thyroxine (T4) labs when a patient presents with symptoms of TED, they should check the levels of the thyroid-stimulating immunoglobulin (TSI) and thyroid-receptor antibody (TRAb).
Teprotumumab to treat TED
In January 2020, the FDA approved teprotumumab (
Tepezza, Horizon Therapeutics) for patients with active TED. It is an antigen-specific therapy designed to block insulin-like growth factor 1 receptors (IGF-1R) and halt the signaling pathway. By blocking IGF-1R, the inflammatory proliferative process associated with Graves’ ophthalmopathy may be diminished.
A
study showed that after receiving teprotumumab, patients experienced an increase in lacrimal gland volume and tear production, meaning that this treatment helps with both TED and alleviating symptoms of dry eye.
Teprotumumab Phase 3 clinical trial results
A
Phase 3 multicenter trial found that teprotumumab could significantly reduce both proptosis and diplopia in patients with active and moderate-to-severe TED. The primary endpoint was achieving a reduction of proptosis of 2mm or more, and at Week 24, 83% of patients (10% of controls) experienced a reduction in proptosis. The secondary outcomes of clinical activity score, diplopia, and quality of life score also showed significant improvement with teprotumumab, compared to the placebo.
Patients were partnered with local infusion centers and received teprotumumab with an IV. The treatment schedule included 8 total infusions with 3 weeks between each infusion, for a total treatment length of 24 weeks.
The infusion schedule was as follows:
- Infusion 1: 90 minutes, ½ dose
- Infusion 2: 90 minutes, full dose
- Infusions 3 to 8: 60 minutes, full dose
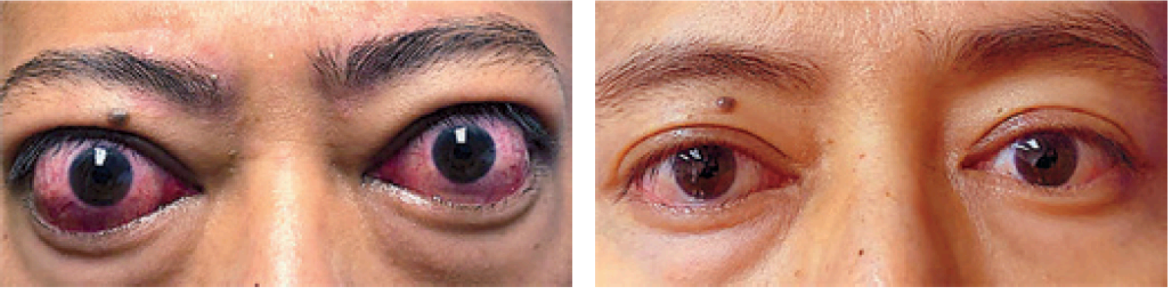
Figure 1 comprises two clinical photographs of a patient in the phase 3 teprotumumab group at baseline (left) and at 24 weeks after the initial dose (right).
Treating chronic TED with teprotumumab
A
study showed that teprotumumab was also helpful for chronic TED patients. Despite the dormant appearance of chronic TED, orbital fibroblasts continually turnover hyaluronic acid and other extracellular matrix macromolecules once a week to maintain tissue integrity. Therefore, interrupting the IGF-1R pathway may reduce the downstream signaling that leads to tissue expansion in chronic TED patients.
Side effects of teprotumumab
The most common adverse events included muscle spasms, alopecia, nausea, and fatigue, most of which were mild in severity and resolved after treatment.
Adverse effects of special interest included hyperglycemia in two patients, worsening inflammatory bowel disease symptoms, and hearing impairment in five patients in the teprotumumab group, all of which resolved without treatment. These auditory adverse events could indicate to ECPs that it would be a good idea to measure a patient’s hearing before starting teprotumumab treatment to have a baseline.
Final thoughts
The development of teprotumumab shows how disruptive innovation can dynamically shift how ocular conditions are treated. This treatment shatters the “watch and wait” mentality and challenges practitioners to be actively on the lookout for this disease so it can be treated earlier and more effectively than before. If you or a patient is interested, there is currently a lot of active research and opportunities for recruiting TED patients for clinical trials investigating teprotumumab.
TED patients can be comforted by the fact that this treatment has been shown to alter the course of their disease and improve their overall quality of life.
Overall, treating thyroid eye disease is a long journey for the patient that requires having multiple healthcare providers on the team. To help with the treatment process, it’s worth
building a referral network within your community of healthcare providers and becoming a resource for primary care physicians and endocrinologists.