When we think of the causes of
dry eye, we often think about meibomian gland dysfunction (MGD) or Sjögren’s syndrome—conditions that affect the meibomian glands and lacrimal glands, respectively. We may also consider bacterial overgrowth,
Demodex mite infestation, or incomplete eyelid closure leading to chronic exposure.
However, a vital component of the ocular surface that is often overlooked is the corneal nerves, which can potentially cause an even greater disruption to the ocular surface if damaged or dysfunctional.
The link between dry eye and corneal nerve function
The cornea has over 7,000 nerve endings per square millimeter, making it the most densely innervated structure in the body.
1-3 Accordingly, proper corneal nerve function is vital to maintaining
ocular surface homeostasis, as the nerves are responsible for providing sensation (including mechano-nociceptors and thermoreceptors),
1 routine epithelial cell turnover and maintenance,
4 corneal wound healing,
1 and blinking coupled with lacrimation.
5,6,7Additionally, the lacrimal gland,
8 meibomian glands,
9 and goblet cells
10-12 receive innervation from branches of the ophthalmic nerve and have all been shown to have parasympathetic innervation. This innervation is responsible for tear production from the lacrimal gland and mucin secretion from the goblet cells,
8,10-12 however, the function of this innervation in the
meibomian glands is unknown.
9Therefore, corneal and ocular surface nerve dysfunction can have a profound impact on ocular surface health, as nerve damage can disrupt normal epithelial cell turnover, impair wound healing, and alter blinking and lacrimation.
Neurotrophic keratitis
This is exactly what happens in
neurotrophic keratitis (NK), which is the result of damage to the corneal nerves, or any point along the trigeminal pathway from which the corneal nerves arise, that results in loss of nerve function.
5,13 This loss of function is characterized by reduced or absent corneal sensation, which is pathognomonic for NK and can lead to the spontaneous breakdown of the corneal surface.
13,14NK is traditionally categorized into three stages of severity:15
- Stage 1: Mild epithelial disruption (epithelial irregularity or superficial punctate keratitis), potentially corneal edema, and symptoms similar to those observed in dry eye.
- Stage 2: Recurrent and/or persistent epithelial defects (PED).
- Stage 3: Corneal ulceration with stromal involvement with eventual complications such as stromal melting and ultimately corneal perforation.
Stages 2 and 3 are relatively easy to diagnose, primarily because these stages display the classic “stain without pain” pattern indicative of NK. “Stain without pain” refers to corneal surface disruptions, such as epithelial defects or ulcers, that pick up sodium fluorescein dye, but have relatively little to no associated pain or discomfort as patients cannot feel this damage due to impaired corneal sensation.
However, Stage 1 NK is much more challenging to diagnose because the signs and symptoms are often subtle and nonspecific, might be more sectoral compared to a geographic presentation found in later stages, and mimic “textbook” findings of dry eye.
So, it is incredibly easy to overlook NK at this stage or attribute it to a more common condition, like dry eye, especially as NK is considered relatively rare.
How to screen patients for NK
It is becoming more apparent that NK is not nearly as rare as it was once thought. A major reason for this is likely due to the fact that prior to the FDA approval of
Oxervate (cenegermin-bkbj ophthalmic solution 0.002% (20 mcg/mL), Dompé) in 2018, there were no treatments specifically indicated for NK.
16 Therefore, fewer doctors may have been looking for NK, as it lacked a dedicated therapy.
“So, if Stage 1 NK can be so subtle, how do we make sure we do not miss it?”
Fortunately, screening for NK is incredibly simple; the only tool required is a cotton-tipped applicator. As I previously mentioned, the diagnostic sign of NK is reduced or absent corneal sensitivity, which is true for all stages of the disease.13,14
So, an easy way to test corneal sensation is by teasing the end of a cotton-tipped applicator to form a wisp and then touching this wisp against the patient’s cornea (in midperipheral to peripheral quadrants and centrally), which allows you to assess their corneal sensitivity, and by extension, their corneal nerve function. If you find the patient has reduced sensitivity or no sensation at all when touching the wisp against their corneal surface, it is a sign you are dealing with NK.
Ideally, we want to catch NK at the earliest stage possible, so we can intervene before it causes significant ocular surface damage, such as the
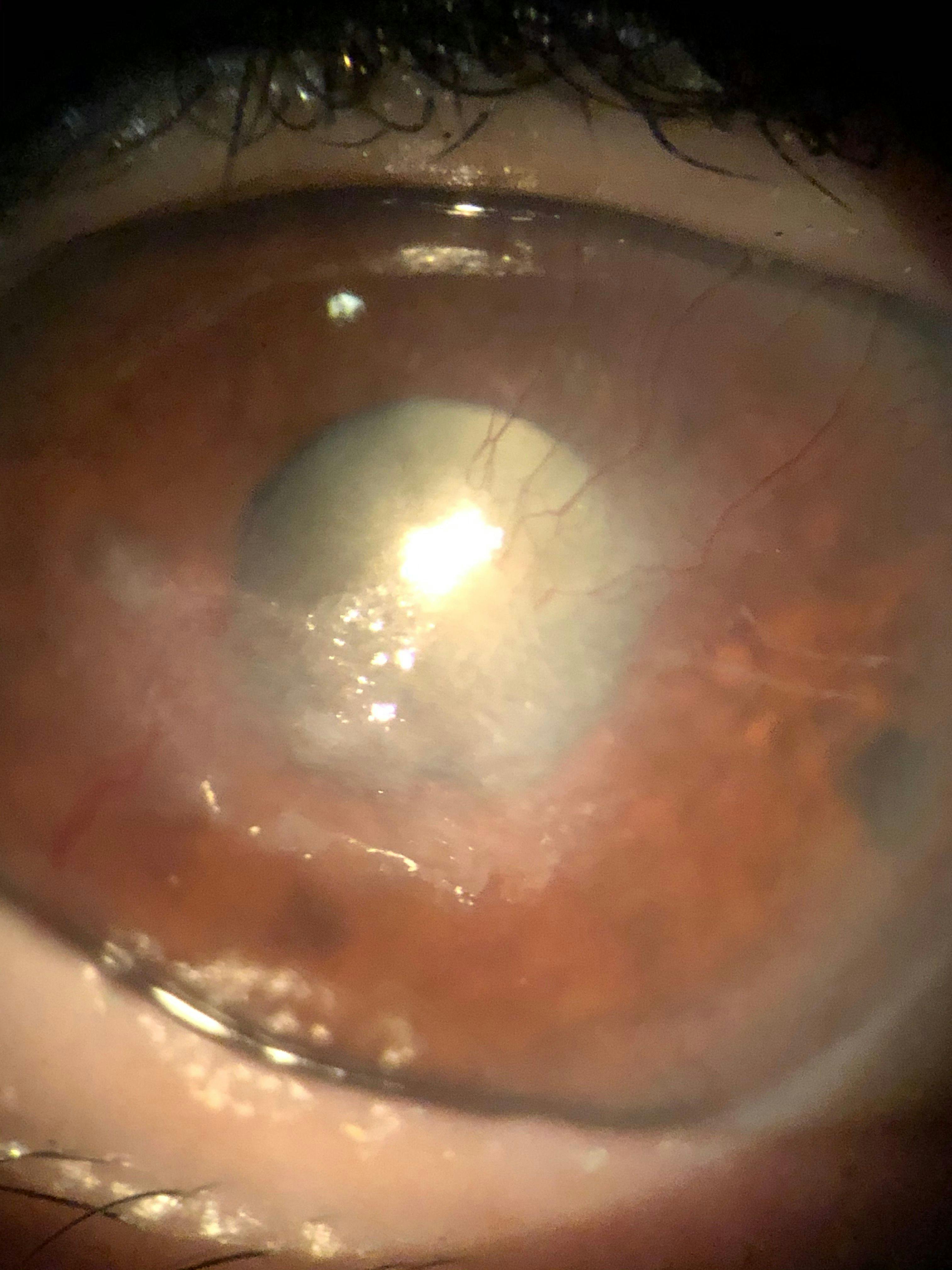
vision-threatening ulcers present in later stages, as shown in Figure 1. This is the reason I recommend checking corneal sensitivity on all dry eye patients, and even non-dry eye patients, if they have a history of herpetic infection or refractive surgery, like LASIK, as these are two routinely encountered causes of NK.
17,18Figure 1 is a clinical image of vision-threatening ulcers in a patient with neurotrophic keratitis that has progressed to later stages.
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO
Pearls for measuring corneal nerve function to identify NK
Another key point to note when screening for NK in its early stages is that it is still possible for these patients to experience ocular discomfort. Even though reduced or absent corneal sensitivity is the hallmark sign of NK, that does not necessarily mean a patient will be entirely asymptomatic in regard to ocular irritation.
These patients often still retain some degree of nerve function, albeit diminished or isolated to one region, and can experience nerve damage that is localized to one area of the cornea rather than the entire surface.
19 This is a crucial concept, as a common mistake made by many eyecare providers is the belief that if a patient has any irritation or discomfort associated with a corneal disruption, then it cannot be
neurotrophic keratitis due to its classic description of “stain without pain,” which yet again leads to an underdiagnosis of Stage 1 NK.
Therefore, when testing corneal sensitivity, it is recommended that sensation be assessed in four quadrants rather than just centrally, in case the nerve damage is limited to only one portion of the cornea.19 Once you start routinely testing corneal sensitivity, you may be surprised how many dry eye patients actually display some degree of desensitization and nerve dysfunction, even in those you would not typically expect.
When I started implementing corneal sensitivity testing as part of my standard dry eye workup, I was astounded by how often patients displayed reduced sensation. To me, this suggests that nerve dysfunction likely plays a much larger role in dry eye and ocular surface disease than previously thought.
Understanding the impact of corneal nerves on dry eye
This implication goes beyond NK. The corneal nerves are capable of sensing more than just mechanical sensation, as they can sense other stimuli, such as temperature and inflammation as well.1,20,21 Homeostasis, the underlying mechanism that allows our ocular surface to function, is a feedback-dependent and self-regulated system that occurs subconsciously, which means it relies on sensory feedback to operate.22
“Therefore, the corneal nerves’ function as the primary sensors of the ocular surface is vital to ocular surface homeostasis.”
Thus, it is likely that the corneal nerves are sensing and providing feedback on stimuli we are not even aware of yet. This would be fitting given the cornea’s extremely high degree of innervation that far exceeds what would be necessary for merely providing sensation. Consequently, nerve dysfunction of any degree causes a significant disruption to the
ocular surface, even beyond just the loss of sensation that is associated with NK.
Overview of neurogenic dry eye
Therefore, NK is just one form of nerve dysfunction on a spectrum of corneal and ocular surface neuropathies, and nerve dysfunction is likely a contributing factor to dry eye more broadly. This concept of nerve dysfunction-related dry eye is recognized in clinical research as
cenegermin, the recombinant form of human nerve growth factor (NGF) used to treat NK, currently being investigated as a treatment for dry eye in general.
23Due to this wide-ranging impact of the corneal nerves on ocular surface health, I have begun referring to cases of dry eye that display nerve dysfunction as neurogenic dry eye (NDE). If we use the classic dry eye divisions as either evaporative or aqueous deficient, neurogenic dry eye would be the third category.
NDE refers to dry eye emanating from nervous system impairment leading to eventual nerve dysfunction or deficit. The role of nerve dysfunction in dry eye has been well established, as neurosensory abnormalities are listed as one of the factors contributing to dry eye in the
TFOS DEWS II definition of dry eye.
24However, these “neurosensory abnormalities” have often been treated as separate, isolated entities, whereas the concept of NDE unifies these conditions under a single category due to their shared nature as ocular surface neuropathies. For instance, I have already discussed NK, which would fall into the category of NDE, but there is also the opposite end of the spectrum in the form of neuropathic corneal pain.
What are some examples of nde?
While NK is a loss of sensation of the corneal nerves,
neuropathic corneal pain, also referred to as neuropathic ocular pain (NOP), is a hypersensitization of the corneal nerves.
25 And just as NK is referred to as “stain without pain,” NOP is referred to as “pain without stain,” as patients often report significant discomfort even though the cornea is otherwise undisturbed.
26Traumatic brain injury (TBI) patients, including those with post-concussion syndrome, also often report dry eye-like symptoms,
27-29 as do those afflicted by a myriad of other potentially nerve-damaging conditions listed below.
Therefore, dry eye-like symptoms associated with these conditions would too be classified as NDE. The causes of NDE are essentially any pathology that can lead to damage of the corneal nerves or the trigeminal pathway from which ocular surface innervation originates.5,25 Thus, there are numerous infectious, traumatic, systemic, genetic, and medication-related causes.
Underlying causes of neurogenic dry eye include:
- Infectious: Herpes simplex,30-32 herpes zoster,33-35 leprosy,36 acanthamoeba keratitis,37,38 and fungal keratitis.37
- Ocular Surface Disease: Chronic dry eye/ocular surface disease,39-44 chronic exposure (lid malposition, lagophthalmos, Bell’s palsy, or Parkinson’s disease),45-47 corneal dystrophies (lattice, granular),14,13 recurrent corneal erosion,48 and chronic corneal pain with blepharospasm.48
- Ocular Surgery: Refractive surgery (LASIK,18,49-51 PRK44,52-54), retinal surgery (PRP/laser,55-57 retinal detachment repair/scleral buckle58-60), glaucoma surgery (micropulse transscleral cyclophotocoagulation [MP-TCP]61-63), corneal incisions (cataract surgery42,48,64), corneal transplantation (keratoplasty: penetrating keratoplasty [PK] and deep anterior lamellar keratoplasty [DALK]),48,64-66 corneal collagen crosslinking (CXL),67 and blepharoplasty.48
- Neurosurgery: Ablative procedures for trigeminal neuralgia68-71 and tumor resection.5,72
- Compressive Lesions/Neoplasms: Tumors (acoustic neuroma,73,74 schwannoma,75 meningioma,75 orbital neoplasm,64 metastatic tumors,76,77 aneurysm,78 and ocular surface neoplasm).48
- Systemic Disease: Diabetes,41,55,79-81 stroke,13,15,64 multiple sclerosis,64,75 vitamin A deficiency,78 amyloidosis,19 degenerative disorders of the central nervous system (Alzheimer’s disease, Parkinson’s disease19), fibromyalgia,41,43 small-fiber polyneuropathy,41,43 trigeminal neuralgia,42 oculofacial pain,42 autoimmune disease (Sjögren’s syndrome, systemic lupus erythematosus [SLE], psoriatic arthritis, inflammatory bowel disease inclusive of ulcerative colitis variants and Crohn's disease, sarcoidosis, and celiac disease).41
- Iatrogenic: Topical timolol and betaxolol,82 topical NSAIDs,83,84 chronic preservative (benzalkonium chloride [BAK]) exposure,85,86 toxic keratopathy,48 abuse of topical anesthetics,87,88 sulfacetamide 30%,89 trifluridine,75 long-term use of oral systemic antihistamines,4,64 long-term use of systemic antipsychotics and neuroleptics,4,64 chemotherapy,25,90 and radiation therapy.48,91
- Traumatic: Corneal chemical burn/injury,5,13,14,48 corneal thermal burn,13 physical corneal trauma,5,13,41,64 facial trauma,92 and traumatic brain injury/concussion.27-29
- Genetic: Congenital corneal hypoesthesia,93,94 Riley-Day Syndrome,95 Goldenhar-Gorlin Syndrome,96 Mobius Syndrome,94 Familial Corneal Hypoesthesia,97 and congenital insensitivity to pain with anhidrosis.98
- Other: Contact lens wear,99 aging,78 dark eye color,78 Adie’s syndrome,100 and dihydroxypyrimidine dehydrogenase (DHPD) deficiency.101
While this list is extensive, the key takeaway is to carefully review a patient’s health history, and if any potentially nerve-damaging condition is present, then NDE should be on your radar.
Neuropathic ocular pain
Besides reduced corneal sensitivity demonstrated with a cotton wisp or Cochet-Bonnet aesthesiometer, what are some other indicators you could be dealing with NDE, specifically NOP?
While the use of in vivo confocal microscopy (IVCM) is particularly useful in identifying nerve abnormalities indicative of NDE, most clinicians do not have access to this technology.25,19 Fortunately, there are a few key signs and simple tests that suggest a patient may have NOP-related neurogenic dry eye.
Symptoms of neuropathic ocular pain
Hallmark symptoms of NOP are allodynia,102 photoallodynia,43 and hyperalgesia,44 which are a hypersensitivity to normal stimuli, hypersensitivity to light, and an elevated sensitivity and extreme response to pain, respectively.
These patients will also often report an inability to tolerate the use of topical eye drops, especially those that contain preservatives, but in some cases, they are even unable to use preservative-free artificial tears due to the hypersensitized nature of their ocular surface.
Additionally, these patients will often report significant discomfort with even the gentlest breeze or very dim lighting. So, if a patient mentions avoidance of certain environments, like a drafty office or grocery stores with bright fluorescent lighting, or they ask to keep the lights off during their exam, these are signs you may be dealing with NOP.
Testing for neuropathic ocular pain
As far as testing goes for NOP, the most straightforward is the anesthetization test. Simply instill a drop of topical anesthetic, such as proparacaine hydrochloride 0.5%, onto the eye and ask the patient if they feel better. If they report an improvement in their symptoms, then you know their irritation stems from a disruption of the ocular surface directly.
If they report no improvement in their symptoms and still feel the surface irritation even with the anesthetic, this indicates the pain is coming from a higher central level other than the ocular surface directly, as peripheral sensation is blocked.48
However, NOP can be classified as peripheral, central, or mixed/combined, depending on the source of the pain.25 While central NOP can be identified by pain that persists even after the instillation of topical anesthetic, peripheral NOP can be harder to differentiate from traditional dry eye as both will improve with anesthetic use.
Therefore, a key sign that a patient has peripheral neuropathic pain rather than traditional dry eye is a nonresponse to conventional dry eye therapies, especially symptomatically.
What to look for in patients with neuropathic ocular pain
What I typically observe in patients with NOP who use a standard dry eye treatment regimen is an improvement in their objective testing results, such as increased tear breakup time (TBUT) or improved lipid layer thickness, yet they still report no subjective improvement in their symptoms.
This suggests that the driving force behind their discomfort may be the nerves themselves, as the other elements of the ocular surface have improved but have not provided any significant relief. So, a nonresponse to traditional
dry eye therapies or improvement that is limited to objective testing measures only with no subjective symptomatic relief, especially in the context of nerve damage, such as a history of LASIK or herpetic infection, is highly suggestive of NOP.
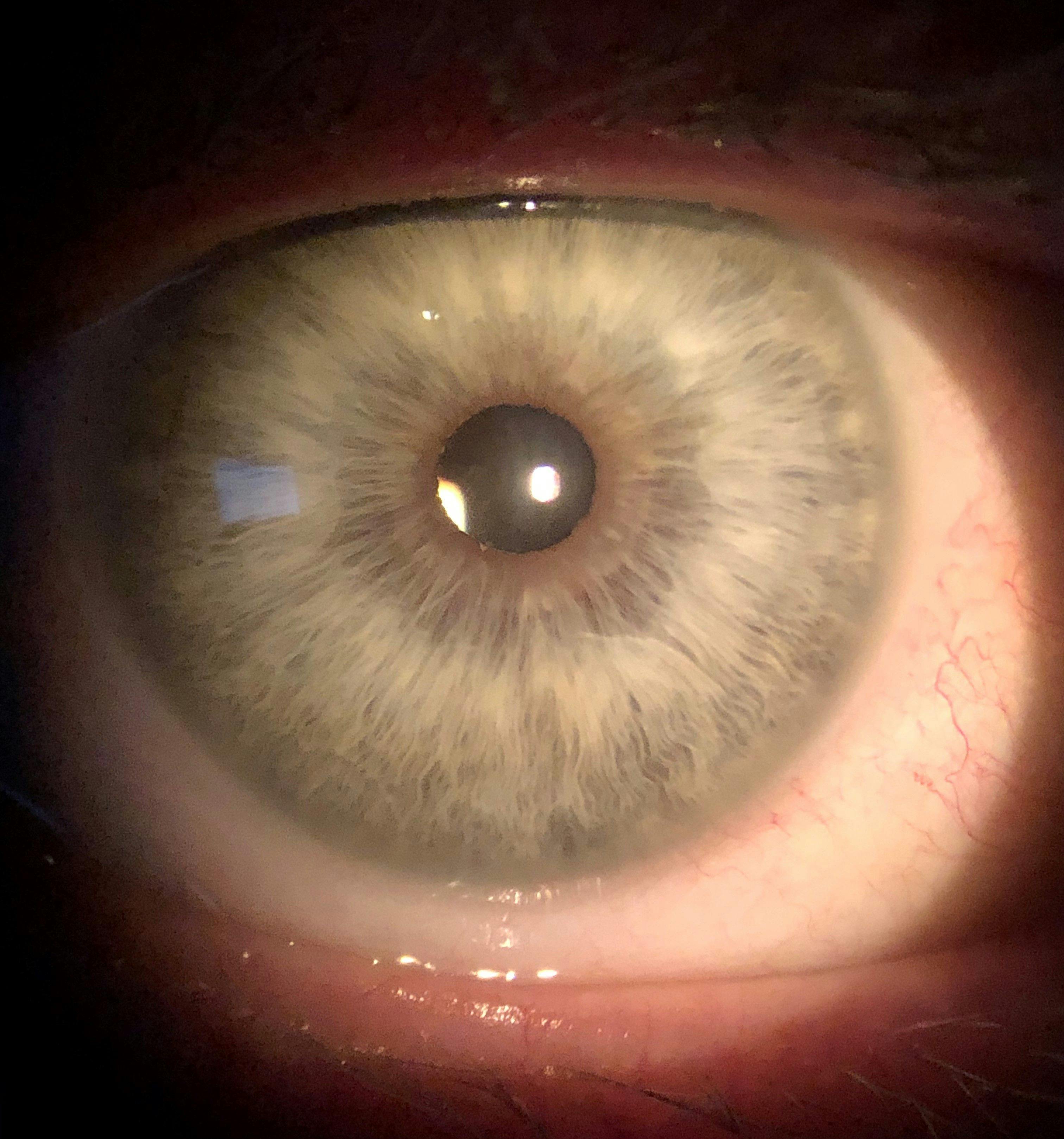
It is worth noting again that it is not unusual for these patients to have a relatively healthy appearance to their ocular surface, like in Figure 2, at the same time they are experiencing significant pain, as this pain can be entirely nervous in nature.25
Figure 2 is a clinical image of a patient with a healthy-looking ocular surface who experienced significant neuropathic ocular pain.
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO
Managing neurogenic dry eye
Once NDE has been diagnosed, how is it managed? By its very nature, NDE is particularly challenging to treat. For instance, with NK we are attempting to heal a cornea that has essentially lost the ability to do so.
As the nerves are responsible for wound healing and epithelial cell maintenance, any treatment that does not restore near function will likely ultimately fail or regress once treatment is discontinued, as sustained healing is often not possible without proper nerve function. Additionally, because blinking and lacrimation are disrupted in NK, this can lead to an unstable tear film creating an environment that is not conducive to healing.
Available treatments for neurogenic dry eye
Although there are many supportive therapies like the use of aggressive lubrication with
artificial tears, or a bandage contact lens to stabilize the corneal surface, or even surgical procedures, such as tarsorrhaphy or the use of a conjunctival flap,
5,75 the best options for treating NK are those that address the root cause by repairing the damaged corneal nerves directly.
Amniotic membranes
This is perhaps best achieved using human nerve growth factor (NGF), which is capable of corneal nerve restoration.
4,103 Amniotic membranes, specifically cryopreserved forms, such as PROKERA (BioTissue Ocular), contain NGF and have been shown to improve NK, especially at early stages.
104 Whereas Oxervate is a recombinant form of human NGF, and is the only FDA-approved therapy specifically indicated for the treatment of NK.16,105 Further, it may be advantageous to apply a ‘one-two punch’ with an amniotic membrane followed by Oxervate thereafter for these patients.
Similar to the recurrent nature of other corneal diseases (i.e., recurrent corneal erosion, Stage 2 NK, herpetic keratitis, etc.), patients might need repeated dosing of Oxervate or combinations thereof to maintain some level of stability to possibly reduce or halt NK progression.
Adeno-associated virus vectors
The potential to use adeno-associated virus vectors (OC-101 AAV-NGF, Viatris) to introduce the genes responsible for NGF production via an intralacrimal gland injection in an attempt to increase the NGF levels produced in tears is in preclinical research.
106 An alternative to NGF that is also being researched is a deleted form of
hepatocyte growth factor (CSB-001, Claris Biotherapeutics), which has neurotrophic, antifibrotic, and anti-inflammatory properties, and also enhances corneal wound healing.
107-110RGN-259 (RegeneRx), a topical form of thymosin beta-4 is also being evaluated as a treatment for NK, as it promotes tissue healing and regeneration through enhanced cell migration and anti-inflammatory properties.
111,112 In cases where other therapies fail, corneal neurotization surgery, where a donor nerve is transplanted to the cornea to restore sensation to the tissue, can be performed.
113-118 Optimizing the ocular surface
In addition to treatments specifically targeting the nerves, the ocular surface should also be optimized when managing NK by treating any concomitant
meibomian gland dysfunction or blepharitis to help create an ocular surface environment conducive to healing.
5,25Managing neuropathic ocular pain
Managing NOP can be equally, if not more, challenging than NK. The hypersensitive nature of the nerves in these patients makes their cases some of the most difficult to treat, as they often do not respond to traditional therapies.25
Determining if the patient has peripheral, central, or mixed NOP is critical to determining the appropriate treatment, as peripheral NOP is due to hypersensitization of the corneal nerves.
Whereas central NOP occurs when nerves of the central nervous system, such as the brainstem and brain, become hypersensitized and can cause the sensation of pain even when no stimulus is present.25,41,48 Consequently, peripheral NOP may improve with topical treatments directed at the ocular surface, whereas central NOP will likely require the use of systemic therapies, and mixed/combined NOP may require both.25
Available treatments for neuropathic ocular pain
Commonly utilized treatments for patients with peripheral NOP include autologous serum tears,
platelet-rich plasma, and
amniotic membranes, all of which are aimed at healing the nerves.
25 Just like in NK, NGF has been shown to improve neuropathic pain, so treatments utilizing NGF are well-suited for the management of NOP also.
25,119,120Topical steroids and the ocular surface
Topical steroids (typically a “soft” steroid such as loteprednol) have also been implemented to address any inflammatory irritation to the nerves and are usually tapered slowly, with the patient eventually being transitioned to a topical immunomodulator such as Xiidra (lifitegrast ophthalmic solution 5%, Novartis), Cequa (cyclosporine ophthalmic solution 0.09%, Sun Pharmaceuticals), or Restasis (cyclosporine ophthalmic emulsion 0.05%, Allergan, An AbbVie Company) for long-term inflammation management.
25 Additionally, any concomitant ocular surface diseases, such as MGD, should also be addressed to prevent exacerbation of the condition.
Contact lenses
The use of soft bandage and scleral contact lenses has been beneficial for some NOP patients, although others have found that the use of contact lenses exacerbates their hypersensitivity.
25 Sealed spectacle frames, such as Ziena dry eye frames (Moisture Chamber Collection, Ziena Eyewear), can help protect the eye from environmental stressors, like air conditioning or ceiling fans, which can be particularly irritating to the patient’s hypersensitive surface.
25Systemic treatments and lifestyle changes
Cases of central NOP often require management beyond topical ocular therapies, such as systemic medications.25 Treatment options for these patients include: tricyclic antidepressants (nortriptyline and desipramine—first-line agents), anticonvulsants (carbamazepine—first-line agent, gabapentin and pregabalin—third-line agents), opioids (low-dose naltrexone and tramadol—second-line agents), serotonin-noradrenaline reuptake inhibitors (duloxetine—third-line agent), and sodium channel blockers (mexiletine—third-line agent).25
Additionally,
lifestyle changes such as regular exercise
121-124 and meditation can be beneficial
25 in managing neuropathic pain, as can dietary considerations like the use of omega-3 fatty acid supplements
125,126 or a gluten-free diet
127,128 if a patient has a gluten sensitivity. Alternative therapies, including acupuncture, have also been shown to help alleviate neuropathic pain.
129Given the systemic nature of the treatments often involved in NOP management, it is best to co-manage these patients with their primary care physician, neurologist, psychiatrist, and/or a pain management specialist, as these patients often require multidisciplinary care.
Additionally, NOP patients also have a strong psychological component to their condition, with depression,44,130 anxiety,44 and post-traumatic stress disorder (PTSD)44 all being common comorbidities that should be addressed with a mental-health professional.
Treating concurrent TBI and neuropathic ocular pain
Patients suffering from dry eye-like symptoms related to a TBI also present unique challenges. In addition to many of the treatments already mentioned, the use of an omega-3 supplement that is high in docosahexaenoic acid (DHA), specifically, may be beneficial in these patients.
While
omega-3 fatty acids, in general, have been shown to potentially improve nerve-related dryness symptoms, a high DHA supplement may be particularly helpful as DHA is the primary omega-3 fatty acid present in the brain, and supplementation has been shown to accelerate nerve repair.
131-134The use of nūretin (PRN Physician Recommended Nutriceuticals), even though it is intended to support retinal health, is a good supplement option in this scenario, as it has a high-DHA formulation.
Available and upcoming neurostimulatory treatments
The importance of the nerves as a target of dry eye treatment is also starting to be recognized, as we now have an entire class of therapeutics dedicated to neurostimulatory treatment.
Tyrvaya (varenicline solution nasal spray 0.03mg, Viatris) and the
iTEAR100 device target the trigeminal nerve to stimulate parasympathetic innervation of the lacrimal gland in an effort to promote natural tear secretion, which contains anti-inflammatory and growth factors lacking in artificial tears.
135-138One of the growth factors secreted in natural tears is NGF, which, as mentioned previously, can be beneficial in treating NDE.4,25,103,119,120,139,140 For this reason, the use of varenicline nasal spray (OC-01, Viatris) is currently being investigated as a potential treatment option for Stage 1 NK,106 as the increased natural tear production may promote healing of the nerves due to the trophic factors present in the tears.
Tyrvaya and iTEAR100 can be particularly useful in treating NOP, as they are dropless options and therefore bypass the need to apply any medication directly to the hypersensitized ocular surface, and therefore may be more easily tolerated.
Another neurostimulatory treatment in the pipeline is
AR-15512 (Aerie/Alcon), which is a TRPM8 agonist that stimulates the thermoreceptors of the corneal nerves, which results in a cooling sensation that can reduce ocular irritation.
141,142Final thoughts on NDE and NOP
While traditionally not as emphasized as evaporative or aqueous deficient dry eye, nerve dysfunction is becoming more widely recognized as a significant contributor to dry eye disease. There are several reasons for the underdiagnosis of this pathology, including its subtlety in signs and symptoms which are often indistinguishable from traditional
dry eye at first glance, as well as the lack of a unifying classification category for these nerve dysfunctions.
However, due to the significant negative impact of nerve dysfunction on the ocular surface and the subsequent burden it places on the patients it afflicts, we cannot afford to miss or ignore these conditions that are likely more common than once thought.
For this reason, it is extremely valuable from both a conceptual and clinical awareness standpoint to consider NDE as a third category of dry eye. Accordingly, it is of paramount importance to screen our patients for nerve dysfunction, whether it be neuropathic keratitis, neuropathic ocular pain, TBI-associated dry eye, or any other form of neurogenic dry eye because if we fail to do so, we are missing a crucial piece of the puzzle in our efforts to care for this particularly challenging subset of
dry eye patients.