



Dealing with a potential traumatic brain injury, whether in or out of the office, can be very stressful. This article will discuss how to recognize, evaluate, and promptly take action when confronted with an acute traumatic brain injury and contains a downloadable cheat sheet for reference.
What is acute traumatic brain injury (TBI)?
Traumatic brain injury (TBI) is defined as a disruption of normal brain function, occurring when cerebral neurons are damaged by an external force. The terms "concussion" and "mild traumatic brain injury" (mTBI) are often used interchangeably. Sports related concussions (SRC) are TBI’s usually caused by blunt trauma.
Types of TBI injuries
Traumatic impact injuries can be defined as blunt, penetrating, or blast.
- Blunt or nonpenetrating injuries are caused by mechanical forces that lead to a rapid acceleration or deceleration with brain impact, such as from a football or a fall.
- Penetrating injury occurs when an object pierces the skull, commonly seen in gunshot and knife wounds.1
- Blast injuries occur through a combination of physical contact and inertial forces, like acoustic waves.2
Get all the information from this article in handy graph form with the Acute TBI in Optometry Cheat Sheet.
Download the cheat sheet now!

Acute TBI in Optometry Cheat Sheet
Get red flags for emergent care and a handy list of TBI visual signs and symptoms.

Prevalence of acute TBI
According to the Centers for Disease Control and Prevention (CDC), approximately 2.8 million people acquire a TBI every year. There were approximately 223,135 TBI-related hospitalizations in 2019 and 64,362 TBI-related deaths in 2020.
Males were two times more likely to be hospitalized and three times more likely to die from a TBI than females.1 Young people aged 0-19 years and older adults aged ≥ 65 years accounted for a large proportion of TBI-related emergency room visits in 2002-2006. The highest rates of TBI hospitalization and death occurred among older adults aged 75 years and older.3 Figure 1 represents TBI-related emergency room visits and age groups.3
Figure 1 illustrated estimated average annual rates of TBI-related emergency department visits by age group in the US from 2002-2006. Young children aged 0-4 years had the highest rate of TBI-related visits, followed by older teenagers aged 15-19 and older adults over 65 years.

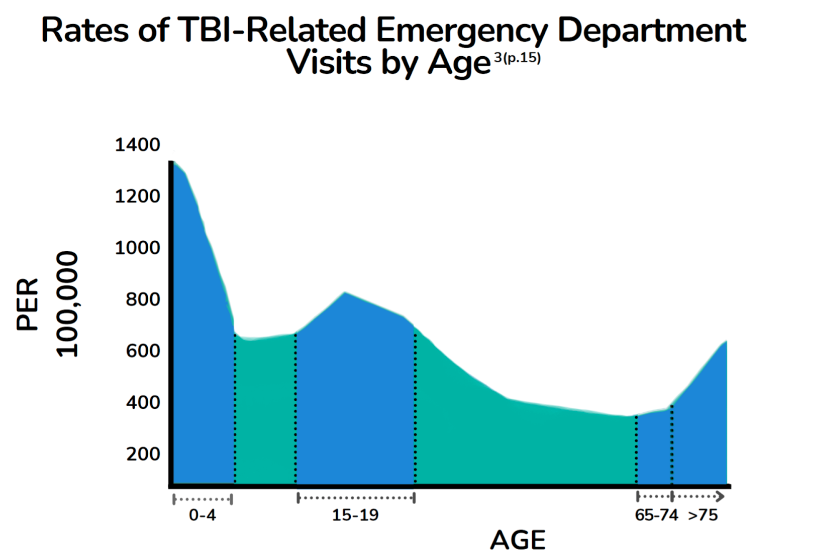
Figure 1: Adapted from Faul et al.
Causes of traumatic brain injury
CDC statistics for 2018 revealed that falling was the leading cause of TBI in the United States, followed by motor vehicle crashes, blunt impact, and assaults. In Figure 2, the CDC percentage statistics on causes of TBI in 2018 are represented.

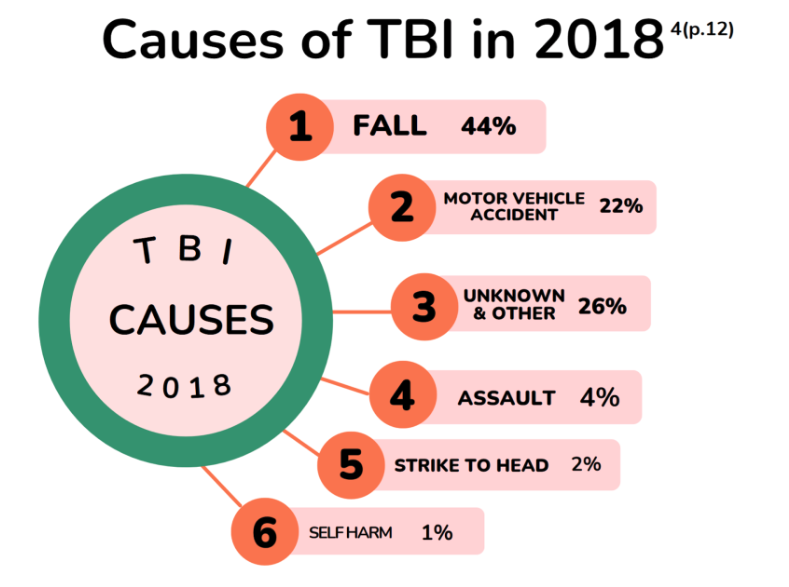
Figure 2
Motor vehicle crashes and assaults were the predominant causes of TBIs in teens and young adults aged 15–34 years.1
Severity and classification of TBI
Understanding the severity of TBI helps with prognosis and patient needs. TBI is often characterized by severity: mild, moderate and severe. Figure 3 shows a breakdown of TBI severity by percentage in 2016.5

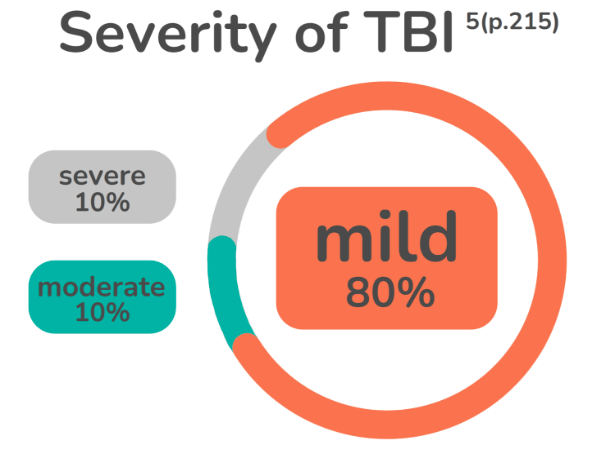
Figure 3
Most TBIs are mild; this category accounts for approximately 75% of all TBIs.
Evaluating acute TBI
Signs and symptoms
Red flags
TBI red flags are important signs or symptoms that should not be ignored. Presence of just one requires acute emergency management.
TBI Red Flags include:
- Abnormal pupils
- Alcohol/drug intoxication
- Amnesia
- Anticoagulant use
- Bleeding/clotting disorder
- Change in behavior: agitation, combativeness, restlessness
- Change or loss of consciousness
- Diplopia or blurred vision
- Drowsiness, cannot be awakened
- Focal neurologic signs
- GCS < 15
- Headaches, especially getting worse
- Increasing confusion or irritability
- Neck pain and/or limited range of neck motion
- Seizures
- Sensitivity to light or sound
- Skull fracture
- Slurred speech
- Unable to recognize people or places
- Weakness/numbness in arm or leg
- Spontaneous
- To verbal stimuli, command, speech
- To pain only (not applied to face)
- No response
Ocular signs and symptoms of TBI
Many visual abnormalities and dysfunctions follow TBI, including functions involving the pupils, accommodation, convergence, pursuits, saccades and the vestibulo-ocular reflex (VOR).8 Merezhinskaya et al. conducted a systematic review and meta-analysis to determine the prevalence rates of accommodative dysfunction, convergence insufficiency, visual field loss, and visual acuity loss in TBI patients.
They found accommodative dysfunction and convergence insufficiency to be the most prevalent, occurring in 42.8% and 36.3% of TBI patients, respectively. They did not find any increased prevalence or significant visual field or visual acuity loss.2
Capó-Aponte et al. analyzed visual dysfunctions and symptoms of war fighters with mTBI. They documented a high frequency of visual dysfunctions and associated visual symptoms at different stages and found no difference in symptoms based on time after injury or mechanism of combat injury, suggesting results would be relevant to non-military personnel.
The most common visual symptoms were:
- Subjective visual complaints (79%)
- Blurred vision at near (66%)
- Reading problems (62%)
- Eye strain (53%)
- Light sensitivity (40%)
The most common visual dysfunctions post trauma involved accommodative and vergence defects.9
Visual symptoms associated with TBI
- Aching eyes
- Color vision issues
- Diculty scanning
- Distance vision blur
- Double vision
- Eye strain*
- Glare sensitivity
- Impaired depth perception
- Photophobia
- Visual fatigue
- Visual field disturbances
Prevalence of visual symptoms associated with TBI. * = statistically significant symptoms.
A previous study by Capó-Aponte et al. listed the subjective visual complaints that were statistically significant for TBI, along with convergence insufficiency symptoms.
Convergence insufficiency symptoms associated with TBI
- Blur/difficulty focusing*
- Diplopia
- Headaches*
- Losing place while reading*
- Loss of concentration
- Need to re-read same lines of words
- Pulling around the eyes*
- Sleepiness
- Soreness of eyes*
- Tired eyes
- Uncomfortable eyes*
Prevalence of convergence insufficiency symptoms associated with TBI. * = statistically significant symptoms.
Diagnostic tests for TBI
There are currently no gold-standard objective measures for diagnosis of an acute TBI. A meta-analysis by Patricios et al. evaluated critical elements aiding sports sideline recognition of potential concussions, such as screening tools and assessment protocols in SRCs. They concluded that “an evidence-based recommendation for any individual screening test or protocol [was] not possible and that the recognition of suspected concussion is best approached using multimodal testing.”11
Glasgow coma scale
The most widely accepted criteria for assessing TBI is the Glasgow coma scale (GCS, represented in the table below; it has the advantages of measuring brain dysfunction in an objective, quick, and repeatable way.12 The GCS looks at three areas: eye opening, verbal performance and motor responsiveness. Responses are assessed and the individual scores are added to give a GCS sum score for mild, moderate, or severe TBI.13 The table below demonstrates the Glasgow Coma Scale.
Glasgow Coma Scale (GCS)
| Eye Opening | spontaneous to verbal to pain none | 4 3 2 1 |
|---|---|---|
| Verbal | oriented disoriented inappropriate incomprehensible none | 5 4 3 2 1 |
| Motor | obeys command localized to pain flexion withdrawal flexion extension no response | 6 5 4 3 2 1 |
TBI Score
| Mild | 13-15 |
|---|---|
| Moderate | 9-12 |
| Severe | 3-8 |
SCAT-5
The Concussion In Sport Group (CISG) developed the Sport Concussion Assessment Tool (SCAT)1 in 2004 to assist medical providers in evaluating SRC and is the most validated and standardized test used in sports. The most recent version, the SCAT-5, is validated for patients 13 years and older; the Child SCAT-5 is used to evaluate SRC in children 5-12 years old.
The SCAT-5 is divided into two parts, the first being a rapid screening assessment that includes red flags, observable signs, GCS, memory, and cervical spine evaluations.
The flow chart in Figure 4 demonstrates the SCAT-5 testing logic.6

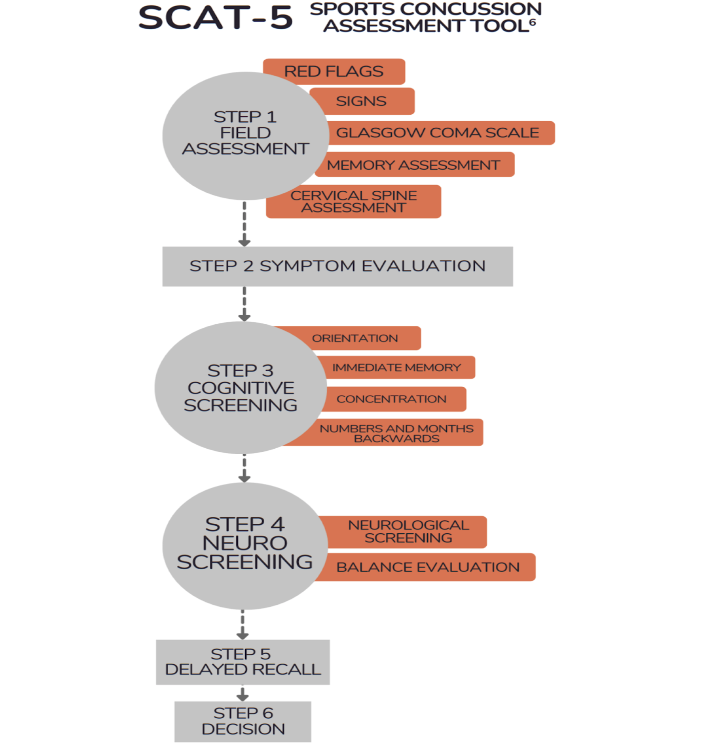
Figure 4
This preliminary quick screening addresses important signs that may need emergency medical treatment. The second part of the SCAT-5 is a more thorough "locker room" assessment that includes a symptoms list, cognitive test, neurological screening, and memory recall assessment.14
King-Devick and MULES
Rapid automatized naming (RAN) tasks study visual perception and reading which require attention, language, and eye-movement control. Because RAN tasks reflect brainstem, cerebellar, and cerebral cortex function, they have been adapted in TBI testing to detect SRC. The King-Devick Test is the most widely used in SRC and requires subjects to make horizontal saccades between numbers as quickly as possible.
Figure 5 shows demonstration and test cards for the King-Devick test, in which patients are asked to read the numbers quickly without any errors. The test is times and scored taking errors into account.16

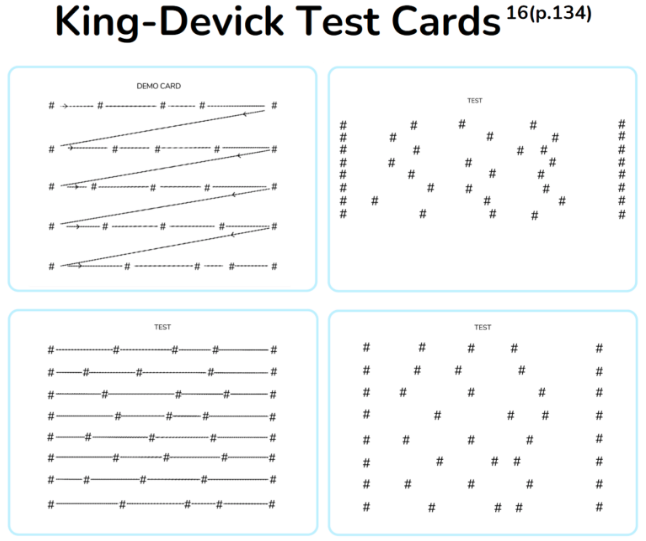
Figure 5
The Mobile Universal Lexicon Evaluation System (MULES) rapid picture-naming test, seen Figure 6, uses color photographs instead of numbers.

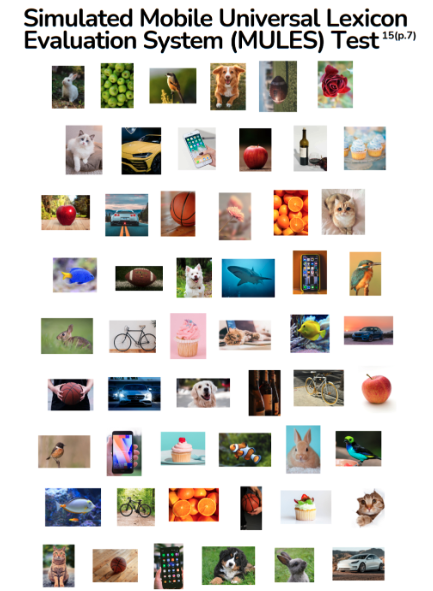
Figure 6
Akhand et al. showed that these RAN tests had the capacity to identify concussed athletes, but warned that learning effects be accounted for to reliably interpret results.15
The CDC ACE tool
The CDC developed the Acute Concussion Evaluation (ACE) tool as an evidence-based protocol for clinicians to conduct an initial evaluation and diagnosis of suspected mTBI. It allows documentation in areas of importance regarding injury characteristics, symptoms, red flags, risk factors, and even lists common ICD diagnostic codes for mTBI.
Figure 7 illustrates the areas addressed by the ACE tool.17

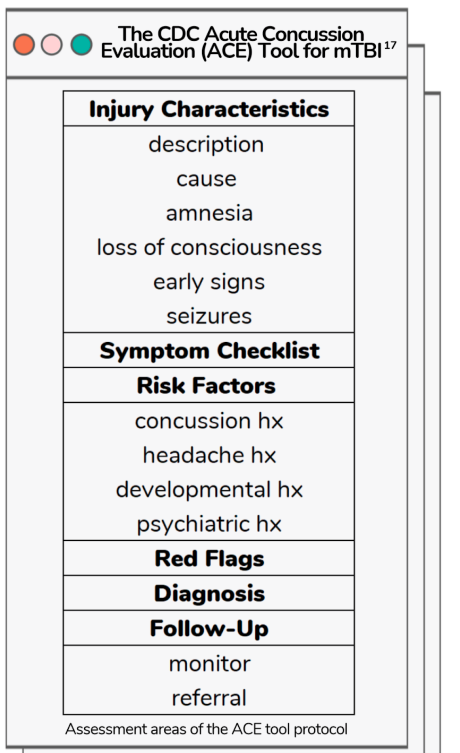
Figure 7
The ACE tool does not make any recommendations regarding scores and does not mention assessments regarding moderate or severe TBI.17
Vestibular Ocular Motor Screening (VOMS)
The vestibular ocular system provides body position information critical for retinal stability and accurate eye movements via neurological pathways in the brain. The Vestibular Ocular Motor Screening (VOMS) evaluates impairments in smooth pursuits, horizontal and vertical saccades, convergence, the horizontal vestibular ocular reflex (VOR), and visual motion sensitivity (VMS).
The VOMS, as seen below in Figure 8, relies on patient-reported symptoms relating to headache, dizziness, nausea, and fogginess, compared to baseline.

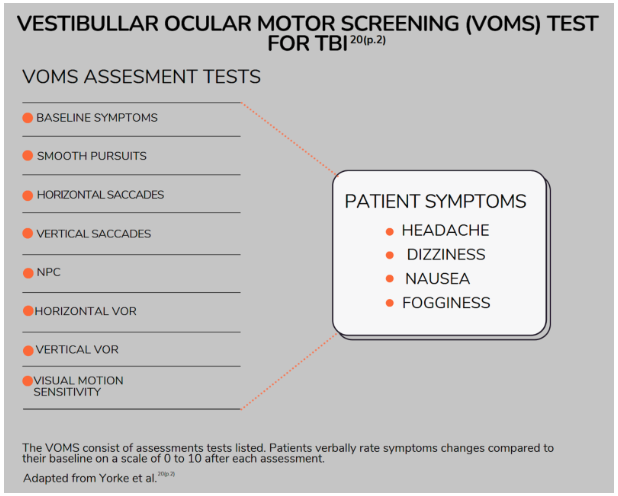
Figure 8
A study by Ferris et al. highlighted the relevance of the vestibular and oculomotor systems in TBI and proved that when the VOMS tool was added to the SCAT3, the overall diagnostic ability to detect concussed patients improved greatly.18 Further, Kontos et al. discovered that vertical saccades and H-VOR were the “most robust discriminators” of TBI among VOMS test items.19
The Eppendorf-Cologne Scale (ECS)
The Eppendorf-Cologne Scale (ECS), introduced in 2012, combines pupil size and reactivity findings with a motor component.
ECS Scoring Strategy Scale
| Category | Finding | Score |
|---|---|---|
| Pupil Reactivity | brisk sluggish fixed | 0 1 3 |
| Pupil Size | normal anisocoric bilaterally dilated | 0 1 2 |
| Motor Response | normal specific nonspecific none | 0 1 2 3 |
Hoffman et al. studied the predictive accuracy of the GCS components with the ECS for TBI diagnosis and outcome. They reported that anisocoria and fixed anisocoria were the most prevalent pupil findings in TBI. Regarding the presence of TBI, the factor with the most predictive accuracy was the GCS verbal component, followed by ECS pupil reactivity, the GCS eye component, ECS pupil size, and finally the GCS motor component.
Their study demonstrated that using the ECS along with the GCS motor component was a good triage tool when assessing TBI.21
Referral
As mentioned earlier in the article, patients having even one “red flag” sign or symptom should be referred to the emergency department immediately. However, diagnosis of acute TBI may not be as clearly defined in mild cases compared to severe injuries. Vaca et al. studied the impact of treatment delays on the outcome in TBI severities and discovered that mild and moderate TBI’s accounted for 50% of the total mortality in the TBI study population. Their conclusions stressed the importance of not only early diagnosis but timely referral for medical intervention in all TBI cases.23
Don't forget to download the Acute TBI Cheat Sheet!
Treatment and patient education
The spectrum of treatment for TBI can range from bed rest, medications, emergency care, surgery, and rehabilitation depending on the nature and severity of the TBI. A review by Hart et al. looked at different methods of patient education in mild, moderate, and severe TBI and confirmed that providing even basic information can improve outcome and recovery of all TBI severities. They validated patient education in a critical role in the management of TBI and called on clinicians to deliver evidence-based content for the future.24
Optometric treatment options
After the acute TBI phase, most patients will present to the optometric practice post TBI, especially if there are visual symptoms. Following the usual exam, which includes refractive and binocular vision assessment, there are several treatment options the optometrist can employ, depending on the particular symptoms and findings. Prescribing tints, plus lenses, prism, and occlusion can specifically benefit the post TBI patient.
