From November 18 to 20, 2022, eyecare practitioners from around the world gathered online for Eyes On 2023, a 3 day educational summit offering up to 9 hours of COPE-accredited CE and CME providing the latest innovations in the ophthalmic industry.
Enjoy this presentation from Eric Donnenfeld, MD, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
A healthy tear film consists of a delicate balance of aqueous, lipid, and mucin components. The lipid layer, the outermost layer, prevents the evaporation of the aqueous and is released through the meibomian glands. Aqueous secretions come from the lacrimal glands and provide
moisture to the eyes through the tear ducts. Lastly, mucins are produced by goblet cells in the bulbar conjunctiva and provide stability with each blink.
Vision starts at the tear film
The tear film is the most important refracting surface of the eye. When discussing any corneal refractive procedure, dry eye is the rate-limiting step for surgical outcomes, so it’s important that any patient with even minimal
dry eye be treated prior to surgery. The ocular surface has an effect on IOL calculations, as well as topography and wavefront measurements.
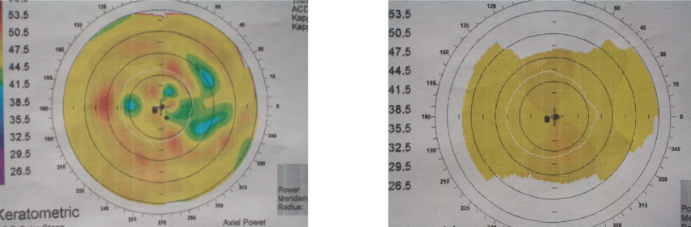
When calculating an intraocular lens, a dry eye can change the results by more than a diopter and greatly distort the direction of the astigmatism. The patients who need the most attention preoperatively are the dry eye patients who are considering a multifocal lens, as all of the issues of glare that inherently come with a multifocal lens will be magnified by the patient's dry eye disease (DED), which translates into an unhappy patient.
Figure 1 highlights two corneal topography maps of a patient with dry eye before (left) and after (right) receiving treatment.
Figure 1: Courtesy of Eric Donnenfeld, MD.
What is dry eye disease?
Dry eye is one of the most common and often undiagnosed diseases in optometry and ophthalmology. Dry eye can be difficult to diagnose because of its variability and the wide range of symptoms accompanying it. When a patient comes in with symptoms of fluctuating vision, they should be treated as if they have dry eyes until proven otherwise.
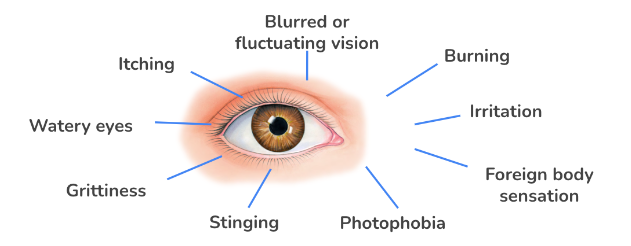
Figure 2 highlights symptoms associated with dry eye disease.
Figure 2: Image courtesy of Eric Donnenfeld, MD.
How is dry eye disease diagnosed?
One of the easiest ways to diagnose dry eye is by
having a conversation with the patient or having them fill out an ocular surface questionnaire. Staining of the cornea is another simple diagnostic test to determine the severity of a patient’s dry eye. Using lissamine green or rose bengal will help diagnose patients with early dry eye disease, whereas fluorescein corneal staining is seen in the later stages of dry eye. At that point, the disease is significant.
“The Schirmer strip is a common diagnostic test used to determine the severity of a patient's dry eye.”
The Schirmer strip was developed in 1904 by Adolf Schirmer. Despite over a century of advancements in dry eye technology, the Schirmer strip continues to be used routinely in offices all over the country. It is still valuable in diagnosing dry eye in patients with a history of
rheumatoid disease such as Sjogren’s, but with the technology now available, relying on the Schermer strip alone is not enough when diagnosing dry eye.
DED prevalence and impact
Studies have suggested upwards of 15% of the United States population suffer from chronic dry eye, which translates to roughly one out of every seven people.
As many as 40% of patients who seek the help of an optometrist or ophthalmologist are there because of their dry eye symptoms; the majority of these patients are elderly, and ⅔ of them are women.
Dry eye has a profound effect on a patient’s quality of life; it causes blurred and fluctuating vision, increased glare, and reduced contrast sensitivity. Just like other chronic diseases, dry eye can significantly affect a
patient’s psychological well-being; patients have reported being willing to take years off the end of their life to be free of dry eye disease. Studies show that DED decreases work productivity, decreases reading speed, and impairs the ability to drive, operate technology, and function socially.
How is dry eye treated?
It is important to explain to patients that
artificial tears can be used to treat dry eye symptoms, but tears will not treat the disease. Several steps can be taken in treating dry eye, starting with
topical and systemic therapy and moving on to nutritional therapy, medication elimination, and environmental control. Simply putting a humidifier in a bedroom can go a long way in treating dry eye disease.
Lastly, a specialty referral, such as to a rheumatologist who can provide systemic therapy for a patient, may help ultimately relieve a patient’s symptoms. Suppose a patient is using artificial tears more than four times a day. In that case, it's recommended that they use a preservative-free option, of which there are many available over-the-counter today.
Nutritional supplements such as omega-3, which were once considered questionable in their effectiveness, are now universally accepted as a valid treatment.
Cyclosporine has been an FDA-approved dry eye treatment for over two decades. This was groundbreaking because, for the first time, rather than simply treating the symptoms, cyclosporine treated the disease process as well.
An example of environmental control is to have the patient position themselves, so they’re looking down at their computer. Looking down while using the computer causes the patient to close their eyes 30% more, slowing the evaporation of tear film.
Stages of dry eye disease
Four levels of severity categorize DED, ranging from level one, indicated by mild clinical findings and episodic symptoms, to level four, in which the patient exhibits disabling marked clinical findings.
Patients with dry eyes overwhelmingly have some form of
meibomian gland disease, and very few dry eye patients will have a simple aqueous deficiency, so it is extremely important to consider the meibomian glands when treating dry eyes. A meibomian gland dysfunction (MGD) patient will have a poor lipid layer and will not lubricate effectively.
Grading meibomian gland dysfunction
MGD is graded in levels of severity from zero to three, zero meaning the presence of normal clear fluid and all glands are expressible, and three meaning the fluid is more of a toothpaste consistency and no glands are expressible. As the meibomian glands atrophy, they do not regenerate, meaning that a patient with severe MGD will suffer from dry eye for the rest of their life.
Microblepharoexfoliation (MBE) is a treatment for MDG in which the eyelids are scrubbed of biofilm. More than half of microbial infections are caused by biofilm. Like the plaque that grows on teeth, biofilm is a bacteria that hot compresses cannot remove. Rather, it needs to be exfoliated. The treatment uses tiny brushes to exfoliate the lids and rid them of biofilm, which aids in other treatments working more effectively as well.
New pharmaceutical treatments for DED
Below is a list of recent developments in pharmaceuticals that treat DED.
- Approved by the FDA in January of 2021, Eysuvis uses proprietary mucus-penetrating nanoparticles that supply a low-dose corticosteroid to the eye.
- Eysuvis will not cause a spike in intraocular pressure, nor will it cause glaucoma. The patient uses it four times a day for a month during flare-ups.
- It can also be used in conjunction with starting Restasis or Xiidra to aid in the effectiveness and speed at which the patient gets relief.
- Inhaled nicotine acetylcholine receptors are now available as well. Varenicline is not an eye drop, it is a medication inhaled through the nose that helps the patient produce tears throughout the day.
- Sustained-release dexamethasone has been approved as a bioabsorbable intracanalicular hydrogel plug that slowly releases low-dose corticosteroids for a month. This option is particularly useful for patients who are about to undergo cataract surgery, as it provides the steroid they’ll need postoperatively.
- A new approach to treating dry eye is to cure the eye of collarettes. TP-03 is a new treatment currently undergoing FDA approval.
- Collarettes are caused by an ectoparasite or mite called Demodex, which lives on the skin. The collarettes are made up of the waste and undigested material of the Demodex, which contains an enzyme that irritates the eyes and clogs the meibomian glands.
Lastly, one way to relieve dry eye, which may not be seen as dry eye therapy, is to get a patient off their glaucoma medication. Patients on glaucoma medications will often have dry eyes due to the
long-term use of preserved drops. Using a bimatoprost implant rather than drops goes a long way toward improving the ocular surface and soothing symptoms of dry eyes.
Conclusion
Dry eye disease greatly affects the results of cataract and refractive surgery, a patient’s quality of vision, and overall life. It has long been underdiagnosed and undertreated by both ophthalmologists and optometrists. These
improvements in treatments, along with entirely new treatments, will enhance our ability to treat dry eye in the future.