


The concept of medical billing in optometry first began over 30 years ago when legislation was passed to include optometry under Medicare. In 1987, President Ronald Reagan approved a Medicare budget expansion, bringing some of the first medical billing privileges to the optometric profession. After seeing the quality of patient care optometry could offer, many other medical insurance companies began to follow suit in allowing ODs to bill medically for their services. Today, over 36,000 optometrists participate in Medicare.
In this article, we’ll review the main reasons why optometrists should be billing medically. We’ll review common office visit/procedure codes used in medical billing, mistakes to avoid as well as discuss how to implement this crucial component to growing your practice.
What is medical billing?
Medical billing is the process of submitting health insurance claims to medical insurance companies (e.g., Anthem, Aetna) on behalf of the patient for the purpose of acquiring reimbursement for any medical eye services rendered. Think diabetic eye exams, ocular emergencies and walk-ins, (e.g., red eye, foreign body, iritis, trauma) or glaucoma follow ups (eg. visual fields, IOP checks). Co-managing ocular surgery also requires the implementation of medical billing.
Optometry medical billing not only includes reimbursement for office visits (eg. 992xx codes) but also myriad procedure codes as well (e.g., fundus/anterior segment photography, optical coherence tomography, visual fields, pachymetry etc).
Why should optometrists adopt medical billing?
Medical billing can be an incredible way to increase practice revenue, expand eyecare services for patients, and practice a broader scope of optometry. In today’s world of healthcare, many clinicians face increased challenges in trying to balance quality patient care while also receiving reimbursement and compensation for their services. Regardless of practice modality, optometrists are no exception to this conundrum.
In most cases, the implementation of medical billing can help circumvent downward trending reimbursement rates from vision care plans. Many of today’s vision plans tend to reimburse at significantly lower rates when compared to medical insurance plans. Many vision plans also encourage patients to purchase glasses and contact lenses through their own online channels, making it even less likely for offices to “make up the difference” of lower exam fees through in-house optical sales.
Steps for effective implementation
Before effectively implementing medical billing, practices and employers must get their optometrist(s) credentialed with medical insurance plans in their area. Being credentialed with Medicare (and Medicaid in some states) is often the first step to getting credentialed with other medical insurance plans in your area.
Understanding billing and coding for medical optometry is crucial for optimizing practice flow and ensuring adequate compensation for services rendered. It is important that doctors and staff are properly trained in optometry coding and billing and have a system in place for submitting medical claims. Failure to do so could cost thousands of dollars in lost revenue. Outsourcing medical billing (i.e., Optometric Billing Consultants) can be a great option for some practices.
ODs should also be familiar with specific patient scenarios where medical billing will take place, and develop patient education “pitches” for why certain testing needs to be performed and why additional follow-up visits may be warranted.
Patient education
Conveying to patients the difference between “vision” and “medical” related eye problems (and which insurance plan will be billed) is important.
Patients must understand that their vision plan will cover their basic exam and glasses, but their medical insurance may be necessary to cover other medically necessary follow ups (e.g., glaucoma management). The patient’s chief complaint can also help dictate whether a patient’s vision plan or medical plan will be billed.
Understanding Medicare’s Merit Based Incentive Payment System (MIPS) is also essential when implementing medical billing. This system allows clinicians to receive payment bonuses (or penalties!) based on various performance measures: Was patient’s PCP sent a summary letter of diabetic eye exam? Was glaucoma patient’s IOP reduced by > 15%?)
Clinicians may be exempt from MIPS reporting for various reasons, including all doctors credentialed during their first year, as well as those who meet the “low volume threshold” (Medicare billing < $90,000/year or seeing <200 patients/year)
Optometry billing challenges to avoid
There are several challenges to minimize and avoid when implementing medical billing. These are typically denied claims and/or audits from insurance companies.
There are several reasons medical insurance claims may be delayed or denied after submission. One is by submitting claims prior to being fully approved and credentialed with an insurance carrier. The incorrect use of modifiers on procedure codes can be another reason for denied claims (see Table 1 below).
Understanding deadlines for submitting claims is also important. Some plans expect claims to be submitted within 60 days from the date of service, while others allow providers up to 12 months (e.g., Medicare).
Avoiding audits from insurance companies is also important when billing medically. These can cost practices hundreds of thousands of dollars and inflate accounts receivables’ balance. Denied or reduced insurance reimbursements are typically triggered by several things. These include excessive use of level 5 (992x5) codes, using the same code for every office visit, ordering tests without a medically necessary reason, and significant variability in codes submitted by nearby doctors.
Having a thorough understanding of CPT coding can help streamline medical billing and avoid triggering an audit.
Medical decision making must also be specified in the EHR when billing medically. This typically can be broken into two categories, “low complexity” (e.g., follow-up visits) and “moderate complexity” (e.g., new problems)
Common Modifiers
| Modifier | Meaning |
|---|---|
| RT/LT | Laterality (right/left) |
| E1, E2, E3, E4 | Eyelids: upper left, lower left, upper right, lower right respectively |
| -24 | When performing office visit during global period of unrelated procedure (eg. foreign body removal during 90-day post-op cataract co-management period) |
| -25 | Used when performing two separate procedures on the same day, unrelated to each other |
| -55 | When co-managing an ocular surgery with an ophthalmologist and only performing the postoperative care |
| -79 | When providing postoperative care on a patient who had surgery performed on both eyes, -79 modifier is used to verify procedure is not a duplicate |
Table 1
Also, remember to have all orders for diagnostic imaging and testing submitted in the EHR prior to the tests being performed. Typically, ophthalmic testing performed as part of a routine work-up (regardless of ocular pathology present) are considered “screening tests” and are not reimbursable.
The timing of testing matters and could be a point of contention during an insurance audit. After diagnostic testing and imaging is performed, results should be documented and interpreted in the patient’s chart. If test results are not written and documented in the chart, the test was not performed as far as the insurance carrier is concerned.
Top codes to know: Glaucoma, diabetes, AMD
Knowing which codes to use is crucial when implementing (and getting paid for) medical eyecare services. ICD-10, procedure, and CPT office visit codes must all match and make sense.
Starting with Evaluation & Management (E&M) or office visit codes, when billing medically, we’ll bill the same 99202 to 99205 (for new patients) or 99212 to 99215 (for established patients) codes that all other medical providers use.
Some common procedure codes that ODs typically use when billing medically include 92250 “Fundus Photography” and 92083 “Threshold Visual Field-Extended”. These bilateral procedures have one fee associated with them regardless if the procedure is performed on one or both eyes. Conversely, “Corneal Foreign Body Removal” 65222 (unilateral procedure) allows a separate fee to be billed if the procedure is performed on separate eyes.
Test frequency is typically determined by the patient’s ocular condition as well as guidelines set by their insurance carrier. Most insurance plans allow two OCT scans per year, generally alternated with threshold visual field testing. For fundus photos, optometrists must establish a medical necessity in the patient’s chart each time they bill for a photo (e.g., “suspicious changes in optic nerve appearance noted on slit lamp exam”).
Remember, that a visual field and a fundus photo (or OCT) can be billed on the same date of service, however an OCT and fundus photo cannot be billed together.
The American Academy of Ophthalmology (AAO) states that a diagnosis of primary open-angle glaucoma (POAG) suspect can be established by the presence of any one of the following clinical findings: consistently elevated intraocular pressure (IOP), suspicious optic nerve head appearance or abnormal visual field presentation. In addition, patients with associated risks of elevated IOP, family history of glaucoma or glaucoma suspect, thin central corneal thickness, African race or Hispanic/Latino ethnicity, older age, myopia and type 2 diabetes.
Diagnostic testing associated with a patient at risk for glaucoma can include gonioscopy, pachymetry, tonometry, perimetry, careful optic nerve observation and ocular imaging. The term “ocular imaging” may include fundus photography and/or OCT based on medical necessity (see table 2).
When it comes to billing and coding for diabetes, most insurance carriers will not reimburse for any diagnostic imaging/testing in the absence of retinal changes. These are considered “screening images” and are typically not covered. On other hand, if patients are being followed for any level of retinopathy or macular edema, then fundus photography and OCT scans are warranted and therefore reimbursable.
Common medical codes
Glaucoma suspect
ICD-10
- H40.00X*: Pre-glaucoma
- H40.01X: Open-angle with borderline findings, low risk
- H40.02X: Open-angle with borderline findings, high risk
- H40.05X: Ocular hypertension
X: 1 = Right eye, 2 = Left eye, 3 = Bilateral
Procedure
- 92250 - fundus photography
- 92083 - threshold visual field
- 92133 - OCT optic nerve
- 76514 - pachymetry
Note: 92133 and 92250 cannot be billed on same date of service
CPT
- 992x2
Glaucoma
ICD-10
- H40.11xx
Primary open-angle glaucoma
Low tension glaucoma
- H40.12xx
Pigmentary glaucoma
- H40.13xx
Acute angle-closure glaucoma
- H40.21x
Procedure
- 92250 - fundus photography
- 92083 - threshold visual field
- 92133 - OCT optic nerve
- 76514 - pachymetry
CPT
- 992x2
Corneal foreign body
ICD-10
- T15.01XA (initial encounter)
- T15.01XD (subsequent encounters)
Procedure
- 65222 - corneal foreign body removal
CPT
- Procedure-only encounter (initial encounter)
- 99212 (subsequent encounter)
Dry macular degeneration
ICD-10
- H35.31xx
- 6th digit laterality (1 = right eye, 2 = left eye, 3 = bilateral)
- 7th digit severity (1 - early, 2 - intermediate, 3 - advanced w/o subfoveal involvement, 4 - advanced w/ subfoveal involvement)
Procedure
- 92250 - fundus photography
- 92134 - OCT retina
CPT
- 992x2 or 992x3
Wet macular degeneration
ICD-10
- H35.32xx
- 6th digit laterality (1 = right eye, 2 = left eye, 3 = bilateral)
- 7th digit severity (1 - active, CNVM2 - inactive CNVM, 3 - inactive scar)
Procedure
- 92250 - fundus photography
- 92134 - OCT retina
CPT
- 992x2 or 992x3
Type 1 diabetes
ICD-10
- E10.3xxx
Procedure
- 92250 - fundus photography
- 92134 - OCT retina
CPT
- 992x2 or 992x3
E10.9 = Type 1 diabetes w/o complication (Cannot bill additional procedures for these)
Type 2 diabetes
ICD-10
- E11.3xxx
- 5th digit : Severity (2 = mild, 3 = moderate, 4 = severe)
- 6th digit : Macular Edema Presence/Absence (1 = yes, 2 = No)
- 7th digit : Laterality (1 = right eye, 2 = left eye, 3 = bilateral)
Procedure
- 92250 - fundus photography
- 92134 - OCT retina
CPT
- 992x2 or 992x3
E11.9 = Type 2 diabetes w/o complication (Cannot bill additional procedures for these)
Dry eye
ICD-10
- H16.143 - punctate keratitis (bilateral)
- H16.123 - filamentary keratitis (bilateral)
- H16.203 - keratoconjunctivitis (bilateral)
- H04.123 - dry eye syndrome of bilateral lacrimal gland
- H02.88A - MGD upper/lower lids (OD)
- H02.88B - MGD upper/lower lids (OS)
Procedure
- 68761 - punctal occlusion (use modifier E1-E4 + OD/OS to specify location/laterality)
- 83861 - tear osmolarity
- 83516 - inflammatory tear test for MMP-9 marker
- 68810 - dilation & irrigation of nasolacrimal duct
(use modifier E1-E4 + OD/OS to specify location/laterality)
CPT
- 992x2
The ICD-10 Glaucoma Reference Guide put out by the American Academy of Ophthalmology (AAO) is also an excellent resource for staging, billing and coding for glaucoma. The AAO also has a great summary of macular degeneration and diabetic retinopathy staging and coding guidelines as well.
The fundus photography, as seen in Figure 1, on a 67 y/o female glaucoma suspect was billed as procedure code 92250. See this list for medicare’s approved diagnosis codes for billing fundus photography.

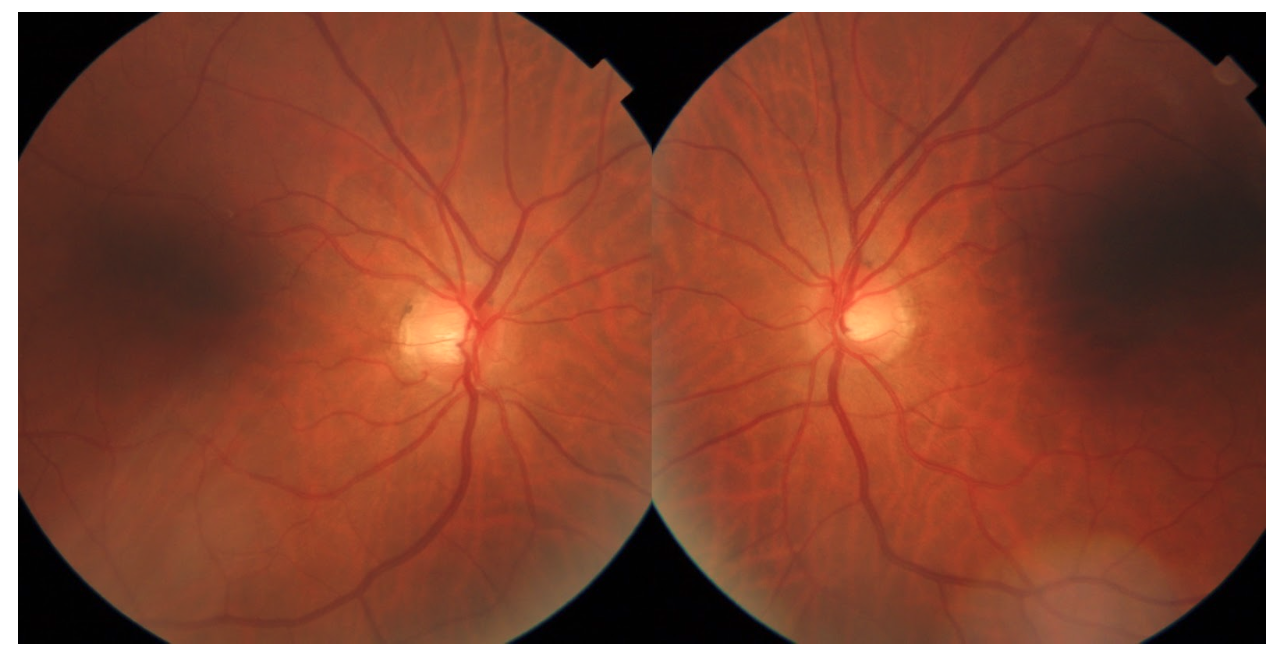
Figure 1: Photo courtesy of Kevin Cornwell, OD.
Optical coherence tomography (OCT) in a 54 y/o male glaucoma patient, seen in Figure 2, was billed as procedure code 92133. For insurance purposes, OCT scans are often referred to as Scanning Computerized Ophthalmic Diagnostic Imaging, or “SCODI” for short. See this list for medicare’s approved diagnosis codes for billing OCT.

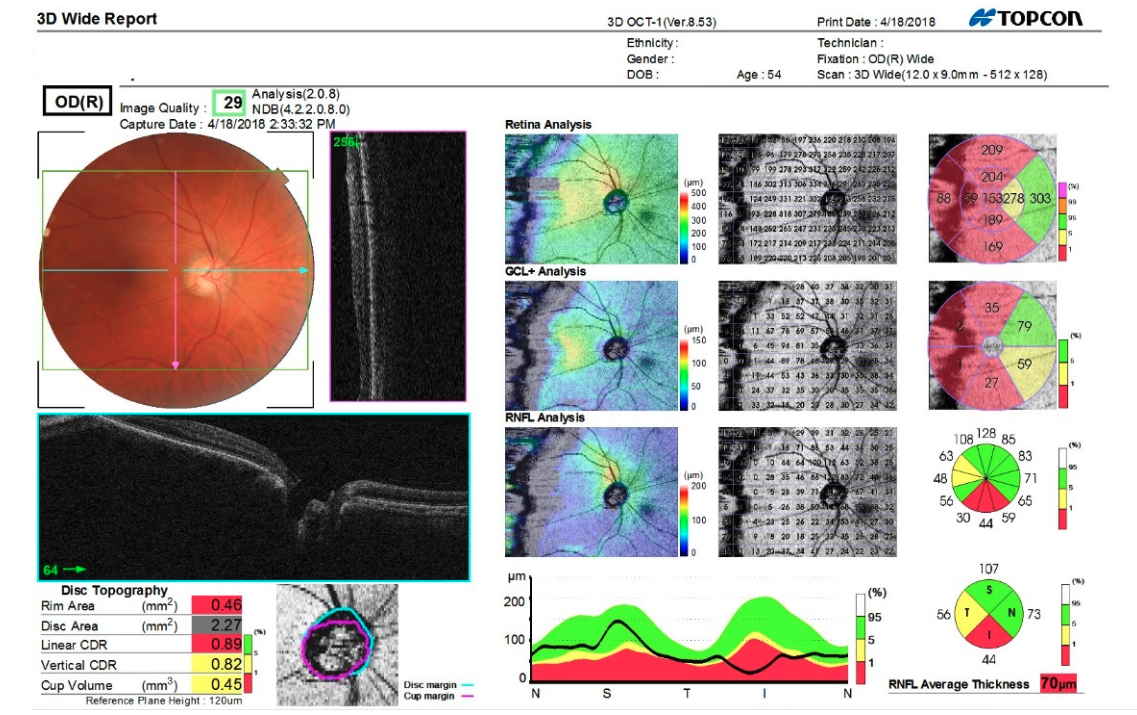
Figure 2: Photo courtesy of Kevin Cornwell, OD.
Staying updated
In most practice settings, the implementation of medical billing makes sense from a business standpoint, but also from a patient-care perspective.
Both the American Optometric Association and American Academy of Ophthalmology are excellent resources for staying up to date with medical billing and coding in eye care. The Centers for Medicare and Medicaid Services and ICD-10 Data are also great resources. In recent years, billing and coding for optometry telehealth services has also come to fruition and is likely here to stay. Don’t overlook this important way to grow your practice and expand the eyecare services offered for your patients!
