



Our 45 year old patient is in for their annual eye exam. Aside from wanting new glasses, they have no additional ocular complaints, and to their knowledge no other pertinent ocular history. We go to check the posterior pole and BOOM, to our surprise their optic nerve is a bit too pale for our liking. Our wheels begin to turn, and the quest for an explanation and diagnosis begins.
When our patient is sitting in front of us, presenting with unexplained optic atrophy, it is our responsibility to provide an explanation and if necessary, conduct a further investigation to determine the etiology. Sometimes the patient will tell us they’ve had a history of a “stroke in the eye” (i.e., NAION) or longstanding decreased vision from a past ocular injury or trauma (i.e., beer bottle or car accident). In these cases, the history can serve as an excellent tool for explaining the optic atrophy.
Other times, the patient may come in with 20/20 vision, not aware of any optic nerve pathology (or maybe even was told at their last eye exam that they were a suspect for glaucoma). Being the astute clinician that you are, you already know any sign of unexplained optic atrophy (simply a finding, NOT a diagnosis) warrants a slightly different medical workup and investigation. Underlying causes of pale optic nerves can range from benign to brain tumor, so the stakes are potentially high. In cases where we come up short on explaining the presence of optic atrophy given the patient’s history and exam findings, neuroimaging is our next best step.[1]
Atrophy to the optic nerve occurs when there is degeneration to the axons of the nerve. This results in recession and loss of the micro-capillary networks that supply the optic nerve. Sometimes the optic nerve can transition from being normal and healthy to having a pale/atrophic appearance. This is referred to as primary optic atrophy. Another scenario is when the optic nerve appears pale and atrophic secondary to a prior history of optic disc edema (secondary optic atrophy).
From anatomy class, we know that unilateral nerve pallor results from lesions anterior to the optic chiasm, whereas lesions affecting the optic chiasm or optic tract can produce bilateral optic nerve pallor, often referred to as “band or bowtie atrophy” (disc pallor @ nasal/temporal disc margins).Optic nerve pallor isn’t always easy to distinguish, especially when assessing the fundus through media opacities like a dense cataract.
Patients who’ve had cataract surgery sometimes appear to have optic nerves that are slightly more pale than usual. This phenomenon, referred to as “pseudophakic pseudopallor,” is caused by the alteration in light filtration between the natural lens and the lens implant after surgery. In these cases, the temporal rim tends to be lighter than the rest of the disc.
Myopic/tilted discs and myelinated nerve fibers can also create the illusion of rim pallor or cupping. Requesting/reviewing old optometry/ophthalmology records from the patient’s last exam can be helpful to clarify exam findings in some cases.
| Primary optic atrophy | Secondary optic atrophy (Prior history of optic disc edema) |
|---|---|
| Central/branch retinal artery occlusion | Arteritic anterior ischemic optic neuropathy (giant cell arteritis) |
| Excessive pan-retinal photocoagulation | Non-arteritic anterior ischemic optic neuropathy |
| Hereditary (Leber’s Optic Neuropathy Dominant Optic Atrophy) | Central retinal vein occlusion |
| Trauma | Optic neuritis |
| Toxic/nutritional deficiency (e.g., chronic alcoholism, malnutrition) | Papilledema |
| END-stage open angle glaucoma | Hypotony |
| Compressive lesion to optic nerve/chiasm/tract (i.e., tumor/aneurysm) | Grave’s disease |
| Congenital (i.e., Optic nerve hypoplasia) |
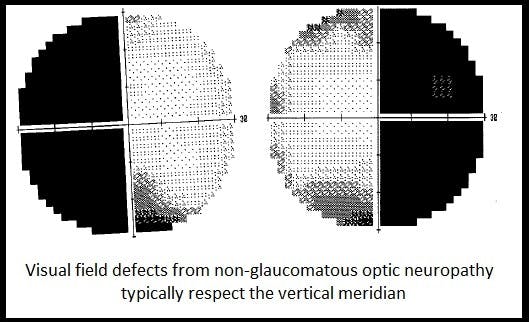
If you suspect a non-glaucomatous optic neuropathy in a younger patient (<50 y/o) with reduced visual acuity, afferent pupillary defect, vertically aligned VF defects, and/or pallor of the neuroretinal rim, you must rule out the presence of an intracranial mass lesion.
Magnetic resonance imaging (MRI) of the brain and orbits (with and without contrast, with fat suppression) is the preferred imaging modality, and in most cases, it is a good place to start . In patients where MRI is contraindicated (i.e., pacemaker, cochlear implant, vascular clips, retained metallic foreign body, prosthetic devices), a computed tomography scan of the brain and orbits may be the next best approach.
Compressive optic neuropathy can be caused by a wide array of conditions, including thyroid eye disease, orbital/intracranial tumors, aneurysms, and orbital inflammation or infection. One study showed that over 50% of non-glaucomatous optic neuropathy was caused by pathology of the pituitary gland,[2] with classic bitemporal vs. junctional scotoma visual field patterns.
Approximately 1/3 of tumors to the optic nerve are from optic nerve sheath meningiomas (ONM). ONM are the 2nd most common tumor to the optic nerve, after optic nerve gliomas.[11] The literature can vary as to what percentage of non-glaucomatous optic atrophy is attributed to compressive etiology, with ranges anywhere from 5%,[3] 20%[4] to over 50%[5] of cases.
Non-glaucomatous optic neuropathy

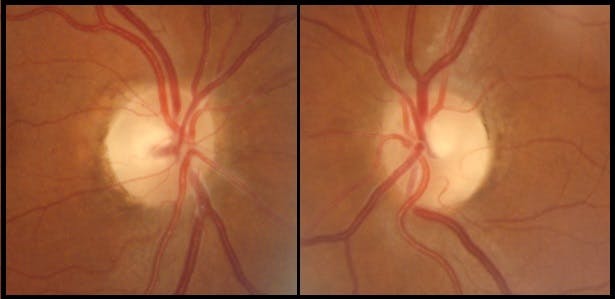

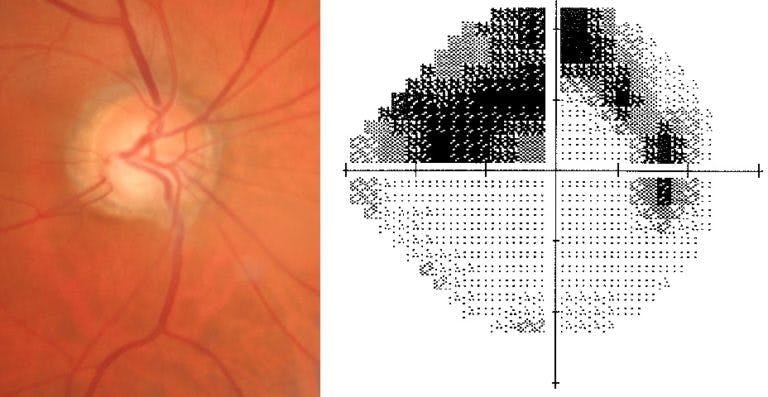
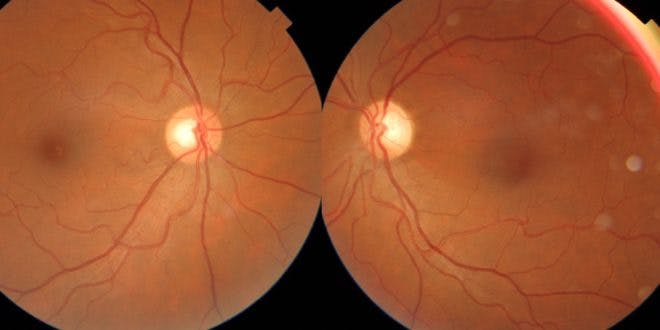
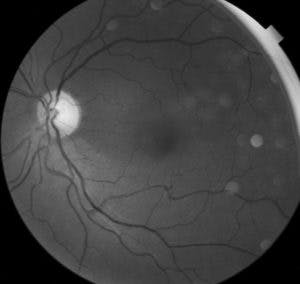
Younger age (typically <50 y/o), vertically aligned VF defect, and optic disc atrophy are more indicative of a compressive lesion. The above example shows the optic nerves of a 50 y/o male with bilateral optic disc pallor secondary to chiasmal compression from a pituitary adenoma.
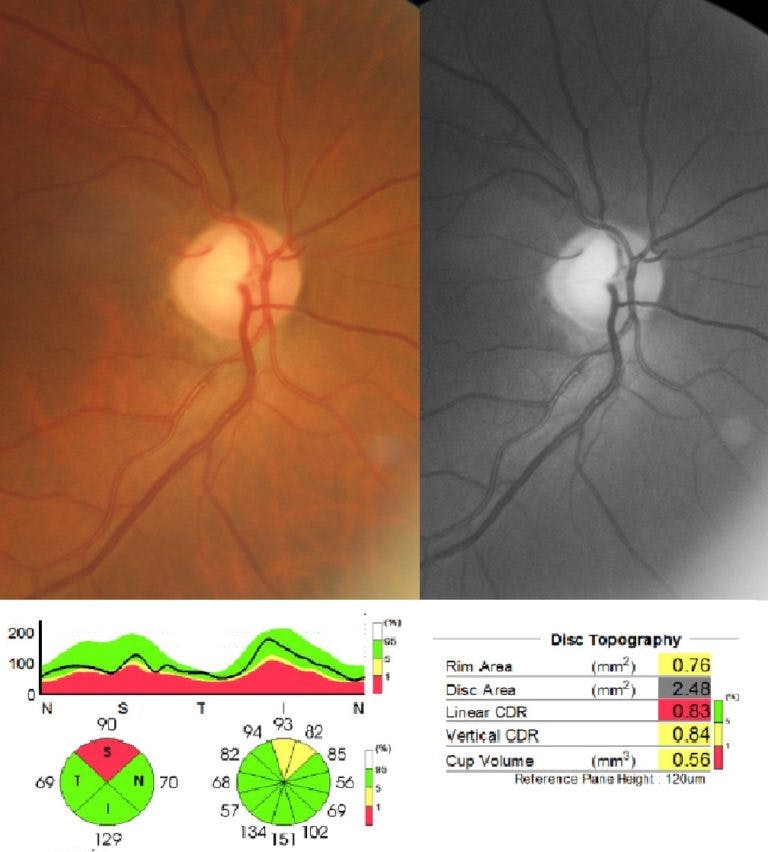
Primary open angle glaucoma

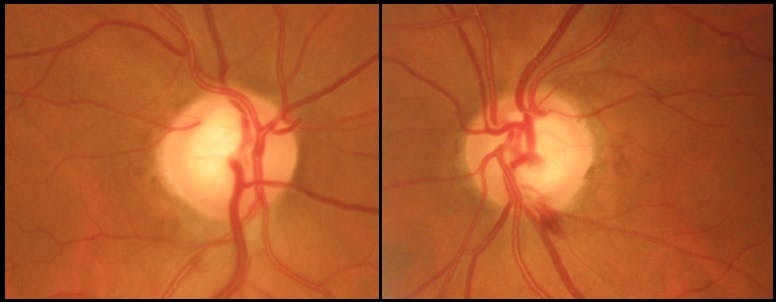

Optic disc hemorrhage, peripapillary atrophy, and horizontally aligned VF defect are almost always pathognomonic for glaucoma. Glaucoma patients are typically older in age (>50 y/o), and still have good visual acuity (better than 20/40).
In glaucoma, the optic nerve almost always predicts the visual field.
A systematic approach to unexplained optic nerve pallor
1) Obtain a thorough case history and timeline for vision loss (acute vs. chronic). While not always reliable, the patient’s age, systemic risk factors, and sequence of events can often help steer our clinical decision making. Does their medical history suggest possible etiology? (i.e., hx of optic neuritis/MS, NAION, drug/alcohol toxicity, pituitary pathology, papilledema, trauma, or high risk meds?)
Ask “was this nerve(s) ever swollen (or edematous) at some point in the past?” Are there any concomitant neurological symptoms occurring (i.e., new headaches, numbness/tingling of extremities, slurred speech, or dizziness)? Requesting and reviewing prior optometry/ophthalmology records can also be helpful in establishing a timeline of vision loss.
2) Examine the patient! Be sure to obtain visual fields, as their pattern can help refine our differential diagnosis. Does the field respect vertical vs. horizontal meridians? Does the pattern localize anywhere specific? If possible, OCT scans can be helpful as well.
3) If you’re still coming up short on explaining a pale nerve(s), proceed with ordering cranial/orbital neuroimaging to rule out compressive etiology (MRI of orbits/brain with and w/o contrast, with fat suppression vs. CT scan if MRI contraindicated).
4) Consider further serologic testing only as appropriate per your history/exam. Unless the patient is at high risk for disease (i.e., if syphillis, sarcoid or lyme are highly prevalent with a particular demographic), general screening evaluations are typically not recommended.[1]
5) Perform multiple visual fields and examinations to establish stability of vision loss.
6) Refer! If you’re still scratching your head trying to explain your patient’s optic atrophy, collaborating or co-managing with a primary care physician, neurologist or neuro-ophthalmologist is a great next step. This is especially true with cases that appear progressive or non-isolated.
Differentiating true glaucoma (POAG) vs. non-glaucomatous optic neuropathy
| Glaucoma (primary open angle) | Non-glaucomatous optic neuropathy |
|---|---|
| Older age (>50 y/o) | Younger age (<50 y/o) |
| Visual acuity typically still good (better than 20/40) | Visual acuity compromised (worse than 20/40) |
| Gradual/painless vision loss | Variable – Can be sudden vs. gradual (+/- pain) |
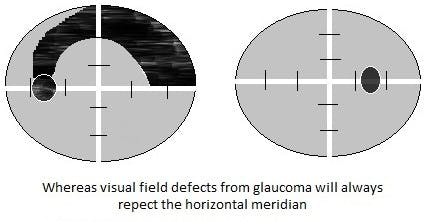
| VF defects respect horizontal meridian[2] Central fixation typically spared until late stages (Norm tension glaucoma +/- paracentral defects) | Variable HVF findings Central vs. peripheral defect More likely to respect vertical meridian[2] |
| Optic nerve appearance correlates well with VF (VF can be BETTER than optic nerve appearance but never worse with glaucoma) | Poor correlation between VF and optic nerve |
| Elevated IOP | Normal IOP |
| Increased cupping/excavation C/d Asymmetry between eyes Vertical elongation of cup, (+) disc hemorrhage | Increased cupping/excavation[6-8] C/d Asymmetry between eyes (-) disc hemorrhage unless concomitant disc edema (+) Collateral vessels |
| Rim tissue pink/healthy Focal notching/rim erosion (very useful if present) | Rim tissue pale/atrophic (diffuse vs. segmental) |
| Superior/Inferior RNFL thinning on OCT | Temporal/Nasal RNFL thinning on OCT[9,10] |
Given the variable nature of vision loss from non-glaucomatous optic neuropathy, the history may not be the most reliable, and the clinician may need to rely more on objective exam findings to help with a diagnosis. Utilizing the red-free (green) filter can also assist with the assessment of the rim tissue and associated nerve fiber layer (this filter is also good for assessing flat/shallow cups that tend to be misleading). Photographing the optic nerves and viewing them side by side can be another useful way to assess suspected unilateral optic disc pallor. Beware, as some cases of compressive pathology and giant cell arteritis have been shown to cause glaucomatous-like cupping.[6-8]
As long as papillomacular bundle fibers are still intact, these patients will typically still have 20/20 visual acuity. Always perform visual field testing on these patients. We know that the magnitude of vision loss is best determined with the assessment of peripheral vision vs. visual acuity alone.[5] Optical coherence tomography can also be of use, as patients with non-glaucomatous optic neuropathy tend to have RNFL thinning more nasal and temporally,[9,10] whereas patients with classic glaucoma have more superior/inferior quadrant thinning.
Until we’re able to definitively explain why our patient has optic atrophy in the first place, we’re not allowed to simply write “optic atrophy, monitor annually” in our assessment and plan. Pale optic nerves are a finding and not a diagnosis. Unfortunately, we’ve all seen this finding written in prior eye exam notes at some point (but not on our charts!). If we’re unable to determine the cause of our patient’s pale optic nerve(s), or if further testing is warranted, it is imperative that we refer the patient to another medical professional with whom we can further collaborate.
Next time you’re confronted with unexplained optic atrophy, don’t panic. You’re already equipped with a strong skill set and knowledge base. It’s just a matter of busting out the clinical toolbox and taking a thorough, comprehensive approach in providing a diagnosis and explanation that makes sense for the patient.
Further examples:

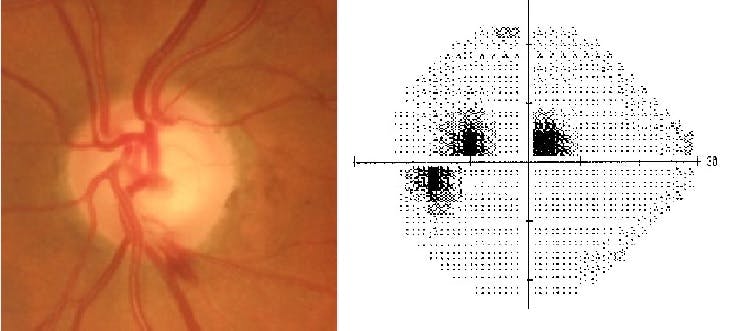
Primary open angle glaucoma: right eye in a 54 y/o male patient presenting for his first eye exam

Traumatic optic neuropathy: left eye with diffuse RNFL dropout superior temporal

Primary open angle glaucoma : right eye with superotemp RNFL wedge defect

Normal Tension Glaucoma left eye with drance heme centrocecal scotoma

Traumatic optic neuropathy with red-free filter with diffuse RNFL dropout superior temporal


Secondary optic atrophy in optic neuritis left eye
References
- Lee, A G, et al. “The Diagnostic Yield of the Evaluation for Isolated Unexplained Optic Atrophy.” Ophthalmology., U.S. National Library of Medicine, May 2005, www.ncbi.nlm.nih.gov/pubmed/158780532.
- Greenfield, David S, and et al. “The Cupped Disc: Who Needs Neuroimaging?” Ophthalmology, Elsevier, 25 Aug. 2003, www.sciencedirect.com/science/article/pii/S0161642098910314?via%
- Osaguona, Vivian B., and Valentina W. Okeigbemen. “Nonglaucomatous Optic Atrophy in Benin City.” Annals of African Medicine, 19 Feb. 2015, www.annalsafrmed.org/article.asp?issn=1596-3519;year=2015;volume=14;issue=2;spage=109;epage=113;aulast=Osaguona
- Mbekeani, Joyce N., et al. “Etiology of Optic Atrophy: a Prospective Observational Study from Saudi Arabia.” Annals of Saudi Medicine, Jan. 2017, www.annsaudimed.net/index.php/vol37/vol37iss3/4447.html
- DeWitt, C A, et al. “Visual Function in Patients with Optic Nerve Pallor (Optic Atrophy).” Journal of the National Medical Association., U.S. National Library of Medicine, May 2003, www.ncbi.nlm.nih.gov/pubmed/12793796
- Bianchi-Marzoli, Stefania, et al. “Quantitative Analysis of Optic Disc Cupping in Compressive Optic Neuropathy.” Ophthalmology, Elsevier, 27 Sept. 2013, www.sciencedirect.com/science/article/pii/S0161642095310032?via%3Dihub
- Sebag, J, et al. “Optic Disc Cupping in Arteritic Anterior Ischemic Optic Neuropathy Resembles Glaucomatous Cupping.” Ophthalmology., U.S. National Library of Medicine, Mar. 1986, www.ncbi.nlm.nih.gov/pubmed/3703503
- Danesh-Meyer, H V, et al. “The Prevalence of Cupping in End-Stage Arteritic and Nonarteritic Anterior Ischemic Optic Neuropathy.” Ophthalmology., U.S. National Library of Medicine, Mar. 2001, www.ncbi.nlm.nih.gov/pubmed/11237915
- Gupta, PK, et al. “Differentiating Glaucomatous from Non-Glaucomatous Optic Nerve Cupping by Optical Coherence Tomography.” National Center for Biotechnology Information, U.S. National Library of Medicine, 26 Jan. 2011, www.ncbi.nlm.nih.gov/pubmed/?term=differentiating%2Bglaucomatous%2Bfrom%2Bnon-glaucomatous%2Boptic%2Bnerve%2Bcupping
- Danesh-Meyer, H V, et al. “Differentiation of Compressive from Glaucomatous Optic Neuropathy with Spectral-Domain Optical Coherence Tomography.” Ophthalmology., U.S. National Library of Medicine, Aug. 2014, www.ncbi.nlm.nih.gov/pubmed/24725827
- Shapey, J. et al.Diagnosis and management of optic nerve sheath meningiomas Journal of Clinical Neuroscience , Volume 20 , Issue 8 , 1045 – 1056
