



You may find yourself in a situation where you need to take an unscheduled photo and the queue for the office fundus camera is long. Or you may find yourself with a squirmy child that may not be able to sit for traditional fundus photography. Or you may find yourself doing exams at the local community center and you see something that you want to document, but you do not have access to any photography equipment. And you may ask yourself, what should I do?
Keep calm and check your back pocket for your smartphone. This tutorial article will instruct you on how you can use your smartphone to take good quality fundus images when access to a fundus camera is not an option.
Smartphone fundus photography scenarios
Smartphone fundus photography (SFP) is not a novel technique, it has been used by clinicians for a number of years since 2010.1 With continued advancement in smartphone technology and camera upgrades, SFP is considered comparable to traditional fundus photography in terms of its accuracy and validity.2 The procedure is cost effective, patient friendly, and the photos can be used for teaching purposes, patient education, or telemedicine. Most clinicians have smartphones and the built-in connectivity and post-processing capabilities make SFP an extremely effective option.
In underserved populations, SFP has become a powerful tool for screening and documentation in clinics that are not able to afford traditional fundus photography equipment. In a humanitarian project in Africa, Furdova et al. used SFP to document their findings, found the method to be a completely manageable technique, and captured high-quality retinal images with excellent reproducibility.3
For many bed-ridden patients, SFP might be the only option if there is lack of mobility and no available fundus camera equipment, such as in a nursing home environment.4 This approach is also helpful in young children or babies who may not be able to sit up for proper chin placement or may not fit into an instrument for a gold-standard exam.
Smartphone fundus photos can be used for teaching students, patient education, or co-management through telemedicine. Photographic data can be sent to a specialist for a remote consultation to assess urgency and discuss treatment. Hanson et al. evaluated telemedicine referrals from optometrists to retinal specialists. Compared to conventional examination and referral methods, telemedicine reduced retinal office visits by 48% and improved the efficiency of the whole treatment process.5
Ocular conditions and interpretation of smartphone images
An early diabetic retinopathy (DR) screening and grading SFP study in 2015 by Ryan et al., compared images taken from smartphones, mydriatic, and non-mydriatic cameras and determined that smartphone images lacked sensitivity in DR detection.6 Since early SFP in DR studies, smartphone technology and clinicians uses of SFP has improved significantly. In 2020, Tan et al. scrutinized the smartphone diagnostic test accuracy in DR. Their meta-analysis reviewed nine studies with 1430 patients and found strong evidence that SFP performed well in detecting DR with high sensitivity and specificity.7
Similarly, the photodocumentation and grading of the optic nerve head cupping is critical in glaucoma screening and management. Idriss et al. studied the vertical cup-to-disc ratio (vCDR) in SFP compared to spectral-domain optical coherence tomography (OCT). They determined that SFP provided high sensitivity and specificity in detection of vCDR >0.5, using OCT as a reference standard.8
While SFP can be used in age-related macular degeneration (ARMD), the gold standard in diagnosis and treatment combines high resolution macular photography with OCT and fluorescein angiography. Because of this, the use of SFP as a diagnostic practice in ARMD has not been validated.9
On the other hand, SFP has been indispensable in pediatrics, especially with the screening and monitoring of retinopathy of prematurity (ROP). Babies and children require fast and precise assessment times due to position, poor fixation and patient cooperation issues. SFP is easy to use and provides the clinician incredible freedom and mobility which is why numerous studies have touted the advantages and importance of SFP in ROP management.10
Lekha et al. demonstrated the technique of fundus examination with scleral depression combined with photography simultaneously. In one hand, they used an adapter, which is a device that holds the condensing lens and smartphone together as one unit. This freed up the examiner to perform scleral depression with the other hand.
Figure 1 illustrates this two-handed technique.10

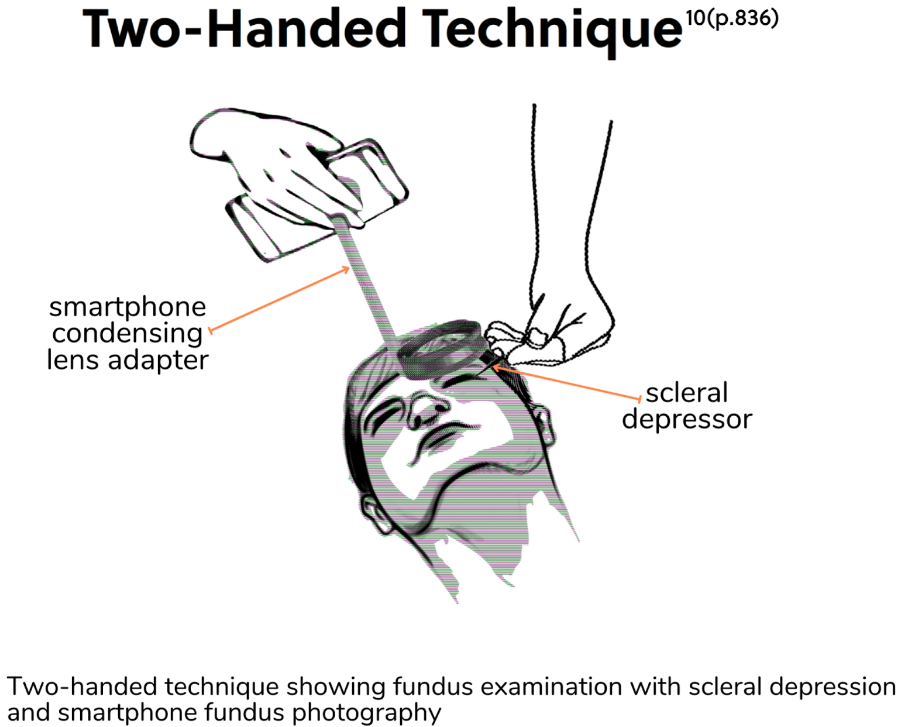
Figure 1: Adapted from Lekha et al.
Adapters, DIY, and apps
This article will focus on using a smartphone alone to capture good quality images, but there are optional devices and apps that are worth mentioning.
Adapters for SFP are devices that hold a smartphone and condensing lens at an adjustable distance lined up co-axially.11 There are three commercially available adapters made by I-spot vision, MII RetCam, and oDocs. These adapters are able to accommodate different sized smartphones and sell for $280 to $380. However, there are a couple of published journal articles for do-it-yourself (DIY) adapters that are quite inventive.The images captured were impressive and of very good quality.12,13
Figure 2 shows an example of an adapter.14


Figure 2: Adapted from Sharma et al.
Along with their adapters, MII RetCam and oDocs both have coordinating apps that aid in image capture that are available for iPhone and Android. While performing SFP, the smartphone camera flash illumination will need to be constantly on. Some smartphones allow manual control and adjustment of the camera flashlight.
For smartphones that do not have this native camera function, there are free apps available that can control the camera flashlight. However, obtaining a separate app is not necessary since turning on the video mode will keep the camera flashlight continuously on.
Finally, most smartphones are capable of image cropping and video editing so photo processing apps may not be necessary. But there are apps available if separate image and video manipulation is desired.
Safety and contraindications
Smartphone cameras can have single, double, triple, or even quad light-emitting diodes (LED) flashlights. A study by Hong et al. showed that the LED light intensity and duration used in SFP was considered to be safe and well below the standards put forth by the International Organization for Standardization (ISO 15004-2.2).15
The study was done with the iPhone 6 and 6 plus which have double LED flashlights. The iPhone 7 and later models have quad LED flashlights. No recent studies have been done with newer smartphones with multiple LED’s. Newer models may have brighter led lights so moderation of the brightness and prolonged time periods should be observed and kept to about one minute.15
Xenon flash is more often used in regular camera photography for their powerful brightness. Xenon flash has the potential to cause possible ocular damage, especially with prolonged exposure times.16,17 The safety of smartphones with xenon flash is not entirely known, therefore SFP with xenon flash is not recommended.
How to take quality photos
Dilation
To achieve the highest quality fundus or SFP images, full dilation is necessary. Good images are possible in non-mydriatic situations but this may depend on patient cooperation, pupil size, proper illumination, and clinician skill.18
Condensing lens considerations
An absolutely clean 20D condensing lens will give optimal results as any debris on the lens surface will cause image artifacts. Glare from the camera flashlight can be managed by a slight tilting of the condensing lens. Glare from room ceiling lights can be reduced by darkening the room.18 A lighter 28D lens will help decrease the amount of focusing necessary and can be easier to use.19
Camera location
In SFP, the smartphone camera should be in alignment with the condensing lens, so awareness of the location of the camera on the backside of the smartphone is necessary. Whether the camera is centered or off in the corner, the smartphone should be adjusted accordingly. Additionally, some smartphones have up to four camera lenses in the rear, so knowing the exact camera lens being used is crucial to getting the best alignment and focus.18
Flashlight location
The location of the flashlight in relation to the camera lens is also important. The closer the flashlight is to the camera lens, the easier it will be to focus on the retina.18 The camera flashlight illumination should not be too bright and it must be set to stay continuously on.
As mentioned earlier, there is no need to download a specialty app if the flashlight cannot be manually adjusted. Simply set the camera to record video, i.e. video mode instead, and the flashlight will be constantly on. Optionally, if there is an ISO adjustment, reducing the exposure to -1 or -0.5 will give exposure levels that might enhance image quality.19 If the camera flashlight it is still too bright, a good trick is to put a piece (or two) of transparent tape over the flash to dull the brightness.20
BIO optics
The optics of binocular indirect ophthalmoscopy (BIO) remain exactly the same in SFP except the clinician’s eye is replaced by the smartphone and the light source is replaced by the flashlight of the camera. The aerial image is also the same as in regular BIO, it is laterally inverted and upside down.18,20
A diagram of the optics is represented by Figure 3.20

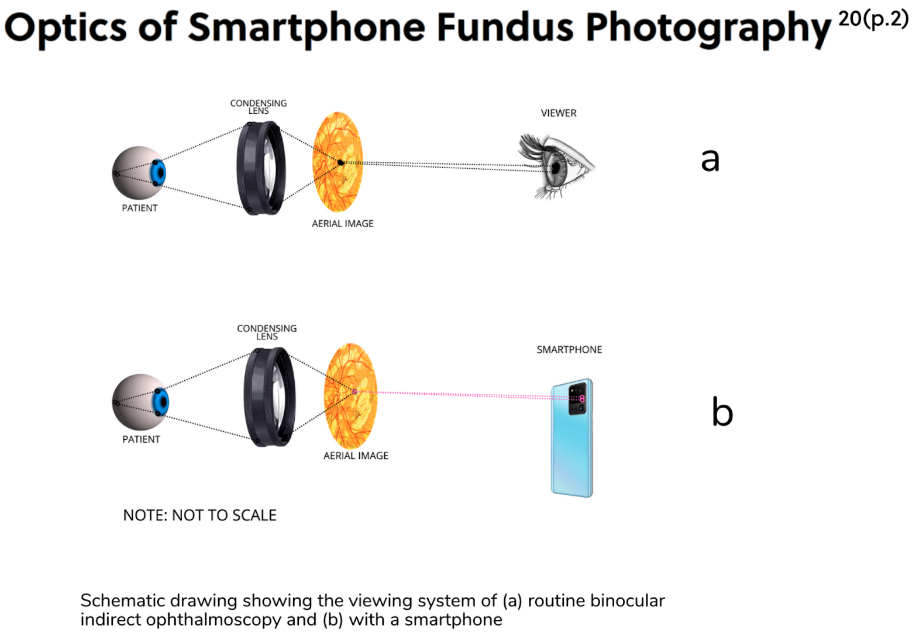
Figure 3: Adapted from Khanamiri et al.
Filming distance
When performing SFP, the condensing lens and smartphone camera lens should both be in alignment with the patient’s pupillary axis. The smartphone is placed between the clinician and condensing lens. The filming distance is the distance between the condensing lens and the smartphone.
The condensing lens may need to be held a little farther away from the patient compared to normal BIO technique. Getting this filming distance is the hardest part of SFP and takes the most practice of getting just right.18
Figure 4 demonstrates the alignment set up.18

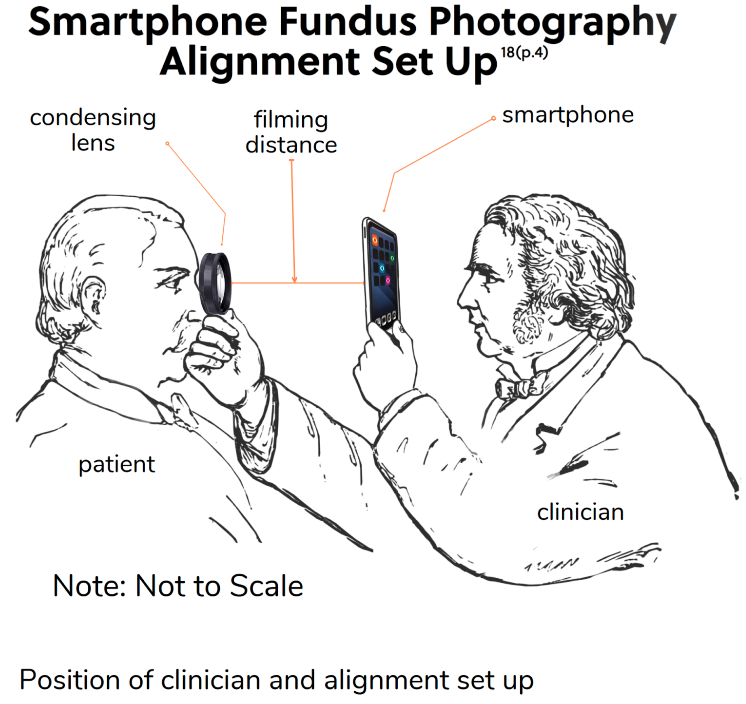
Figure 4: Adapted from Iqbal
Magnification and photo/video capture
Recording video may be easier than taking photos, especially in the beginning of the learning curve.
To record video, follow these steps:
- Set the smartphone camera to video mode and start recording.
- Simultaneously, introduce the smartphone camera and adjust the condensing lens, aiming the beam of light through the pupil and lining everything up to get the best results.
- Focus the image and adjust the zoom on the smartphone camera so that the entire condensing lens fills the smartphone display screen.
- Have the patient adjust their fixation in all quadrants as usual for different fields of view, and direct their fixation to center any areas of interest.19
Refer to Figure 5 for a drawing of a smartphone display screen with the retina in focus.18

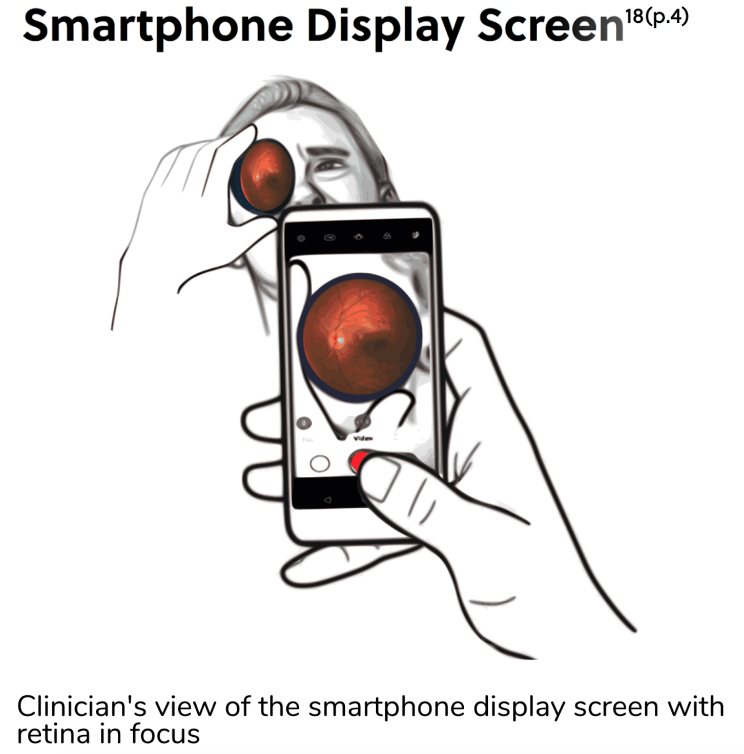
Figure 5: Adapted from Iqbal
Image processing and video editing
From the video, the best images can be captured, adjusted and cropped at your leisure. As mentioned earlier, the image is laterally inverted and upside down so photo editing can be done at your discretion. Also, the video can be edited to delete any redundant views. This will reduce the file size which will decrease upload times. A wide field montage or collage can be pieced together from images taken from different quadrants.
Figure 6 compares the image quality differences from SFP and standard fundus photography, such as glare, distortion and overall blur.

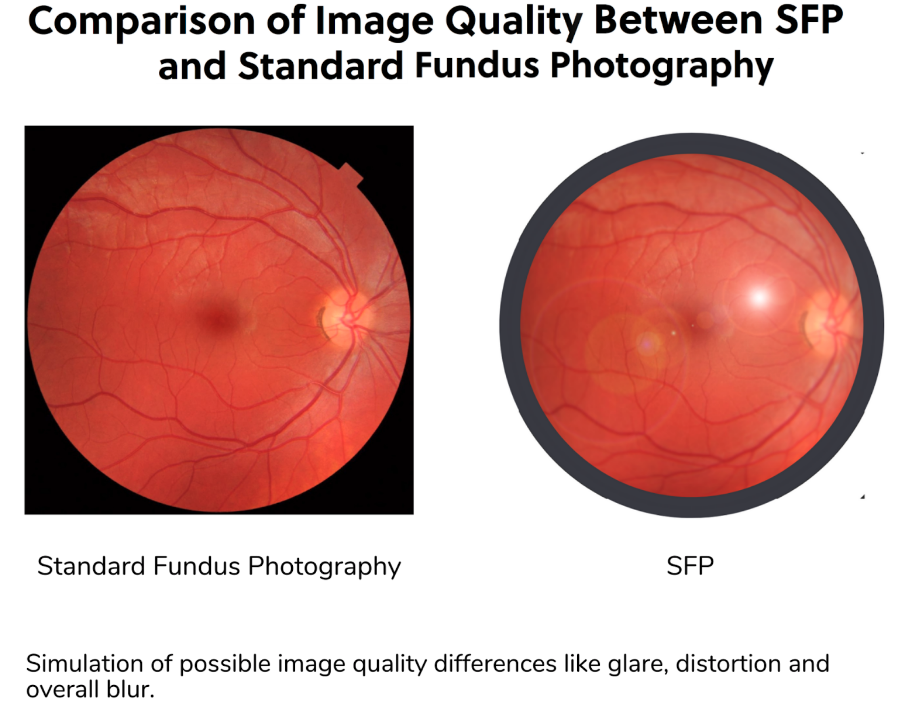
Figure 6
Becoming proficient in SFP may take some practice but the learning curve is not steep for the experienced clinician. The more the procedure is performed, the easier it will be to use this skill when called upon.
HIPAA
HIPAA guidelines must be followed throughout the whole process of SFP. The usual practice for obtaining patient consent for photographs apply before taking any photos. The smartphone device should have all security measures in place that adhere to HIPAA protocols such as having password protection and encryption. Additionally, the smartphone should be set to auto lock if idle and have the capability to be wiped if it is lost. Data transfer and storage should be done using encryption and password protection as well, whether the images are being transferred to a local drive, cloud storage, or another clinician for consultation.
When transmitting the images to another clinician, all security measures must be in place. Even if a text messaging service is encrypted, unless it is known to be expressly HIPAA compliant, texting photos is not wise. Further, data should only be transmitted using HIPAA compliant systems.
All these security measures will ensure patient confidentiality and HIPAA compliance especially when using SFP.21
Fundus photography is the standard of care in photodocumenation and an essential part of patient care and management. However, if you find yourself in a position where you may need to take a quick photo of a fundus irregularity or concern, and you do not have access to a fundus camera, just know that you probably have a powerful tool in your back pocket. You can calmly whip out your smartphone and capture a good quality image quickly and efficiently on the fly.
References
- Lord RK, Shah VA, San Filippo AN, Krishna R. Novel uses of smartphones in ophthalmology. Ophthalmology. 2010;117(6):1274-1274.e3. doi:10.1016/j.ophtha.2010.01.001
- Vilela MA, Valença FM, Barreto PK, Amaral CE, Pellanda LC. Agreement between retinal images obtained via smartphones and images obtained with retinal cameras or fundoscopic exams - systematic review and meta-analysis. Clin Ophthalmol. 2018;12:2581-2589. Published 2018 Dec 11. doi:10.2147/OPTH.S182022
- Furdova A, Furdova A, Krcmery V. Our experience with smartphone and spherical lens for the eye fundus examination during humanitarian project in Africa. Int J Ophthalmol. 2017;10(1):157-160. Published 2017 Jan 18. doi:10.18240/ijo.2017.01.25
- Bhayana AA, Prasad P, Azad SV. Using smartphones for documenting bedside retinal findings during COVID-19 times. BMJ Case Rep. 2021;14(7):e245377. Published 2021 Jul 26. doi:10.1136/bcr-2021-245377
- Hanson C, Tennant MT, Rudnisky CJ. Optometric referrals to retina specialists: evaluation and triage via teleophthalmology. Telemed J E Health. 2008;14(5):441-445. doi:10.1089/tmj.2007.0068
- Ryan ME, Rajalakshmi R, Prathiba V, et al. Comparison Among Methods of Retinopathy Assessment (CAMRA) Study: Smartphone, Nonmydriatic, and Mydriatic Photography. Ophthalmology. 2015;122(10):2038-2043. doi:10.1016/j.ophtha.2015.06.011
- Tan CH, Kyaw BM, Smith H, Tan CS, Tudor Car L. Use of Smartphones to Detect Diabetic Retinopathy: Scoping Review and Meta-Analysis of Diagnostic Test Accuracy Studies. J Med Internet Res. 2020;22(5):e16658. Published 2020 May 15. doi:10.2196/16658
- Idriss BR, Tran TM, Atwine D, Chang RT, Myung D, Onyango J. Smartphone-based Ophthalmic Imaging Compared With Spectral-domain Optical Coherence Tomography Assessment of Vertical Cup-to-disc Ratio Among Adults in Southwestern Uganda. J Glaucoma. 2021;30(3):e90-e98. doi:10.1097/IJG.0000000000001779
- Mintz J, Labiste C, DiCaro MV, McElroy E, Alizadeh R, Xu K. Teleophthalmology for age-related macular degeneration during the COVID-19 pandemic and beyond [published online ahead of print, 2020 Sep 29]. J Telemed Telecare. 2020;1357633X20960636. doi:10.1177/1357633X20960636
- Lekha T, Ramesh S, Sharma A, Abinaya G. MII RetCam assisted smartphone based fundus imaging for retinopathy of prematurity. Indian J Ophthalmol. 2019;67(6):834-839. doi:10.4103/ijo.IJO_268_19
- Ludwig CA, Murthy SI, Pappuru RR, Jais A, Myung DJ, Chang RT. A novel smartphone ophthalmic imaging adapter: User feasibility studies in Hyderabad, India. Indian J Ophthalmol. 2016;64(3):191-200. doi:10.4103/0301-4738.181742
- Raju B, Raju NS, Akkara JD, Pathengay A. Do it yourself smartphone fundus camera - DIYretCAM. Indian J Ophthalmol. 2016;64(9):663-667. doi:10.4103/0301-4738.194325
- Chandrakanth P, Ravichandran R, Nischal NG, Subhashini M. Trash to treasure Retcam. Indian J Ophthalmol. 2019;67(4):541-544. doi:10.4103/ijo.IJO_1524_18
- Sharma A, Subramaniam SD, Ramachandran KI, Lakshmikanthan C, Krishna S, Sundaramoorthy SK. Smartphone-based fundus camera device (MII Ret Cam) and technique with ability to image peripheral retina. Eur J Ophthalmol. 2016;26(2):142-144. doi:10.5301/ejo.5000663
- Hong SC, Wynn-Williams G, Wilson G. Safety of iPhone retinal photography. J Med Eng Technol. 2017;41(3):165-169. doi:10.1080/03091902.2016.1264491
- William T. Ham, Harold A. Mueller, and Thomas S. Ely, "Potential ocular hazards from xenon flashlamps," Appl. Opt. 26, 3466-3469 (1987)
- Pitts DG, Cullen AP. Determination of infrared radiation levels for acute ocular cataractogenesis. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1981;217(4):285-297. doi:10.1007/BF00429289
- Iqbal U. Smartphone fundus photography: a narrative review. Int J Retina Vitreous. 2021;7(1):44. Published 2021 Jun 8. doi:10.1186/s40942-021-00313-9
- Raju B, Raju NS. Regarding fundus imaging with a mobile phone: a review of techniques. Indian J Ophthalmol. 2015;63(2):170-171. doi:10.4103/0301-4738.154407
- Nazari Khanamiri H, Nakatsuka A, El-Annan J. Smartphone Fundus Photography. J Vis Exp. 2017;(125):55958. Published 2017 Jul 6. doi:10.3791/55958
- Thomas VA, Rugeley PB, Lau FH. Digital Photograph Security: What Plastic Surgeons Need to Know. Plast Reconstr Surg. 2015;136(5):1120-1126. doi:10.1097/PRS.0000000000001712
