“My eyes were never dry until I had cataract surgery.” This is a statement nearly every eyecare provider has heard at one point or another, but it highlights the importance of discussing and addressing any signs of dry eye and
ocular surface disease (OSD) prior to surgery, even if the patient is asymptomatic.
In fact, one study found that over 37% of patients who underwent cataract surgery were found to have dry eye postoperatively that was not previously present.
1 This is just one of several reasons why it is crucial to address OSD
prior to ocular surgery.
Overview of OSD and cataract surgery
It is especially true for cataract surgery, as advancements in the procedure and the use of
premium intraocular lenses (IOLs) have essentially transformed the surgery into a refractive procedure, where many patients’ expectations for their postoperative vision are beyond just the improvement gained by removing the cloudy crystalline lens.
Many cataract patients now expect to have minimal, if no, reliance on spectacle or contact lens correction after surgery, especially if they opt for a premium
intraocular lens, which typically is paid for out-of-pocket. All these factors create high expectations for a patient’s postoperative visual outcome, and, as we all know, the greatest disappointments often come from unmet expectations.
Where we begin: preoperative assessments for OSD
The first step towards meeting these expectations begins well before any surgical incision is made. One study found that 45% of patients with cataracts were shown to have dry eye, while another found that 80% of patients presenting for cataract surgery displayed at least one sign suggestive of ocular surface dysfunction.
2,3 In terms of
meibomian gland dysfunction (MGD), 52% of patients presenting for cataract surgery had MGD; however, half of these patients were asymptomatic.
4 Switching to dry eye, it is estimated that over 24% of cases, in general, are asymptomatic.
5Therefore, ECPs need to be proactive in screening for ocular surface disease, especially those with significant or developing cataracts, for whom surgery is likely on the horizon, even if the patient is asymptomatic. And if a patient is already experiencing symptomatic dry eye, any ocular surface disease must be addressed prior to surgery, as the procedure will likely only serve to exacerbate their condition.6
Additionally,
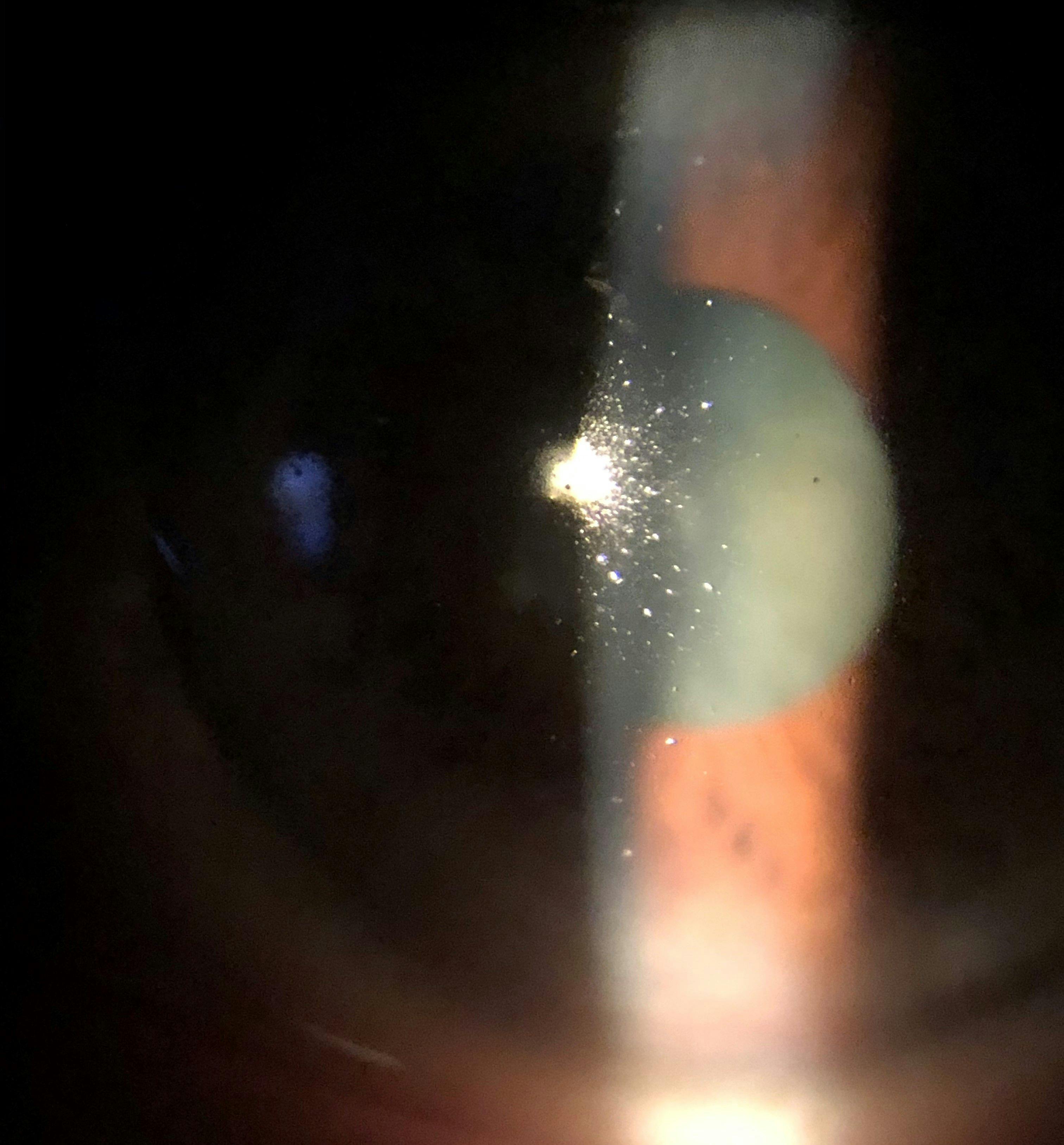
dry eye and OSD create an unstable tear film, as displayed by the cataract patient in Figure 1, which can negatively impact preoperative measurements used to calculate IOL power, which can lead to poor postoperative refractive outcomes.
7,8Figure 1 is a clinical image of a cataract patient with an unstable tear film caused by ocular surface disease.
Figure 1: Courtesy of Cory Lappin, OD, MS, FAAO
Next steps: treating the ocular surface disease
The process of preparing the ocular surface for surgery begins by recognizing the signs and symptoms of common ocular surface diseases, including dry eye, MGD, blepharitis,
ocular rosacea, and chronic ocular surface exposure due to incomplete lid closure or malposition.
General signs and symptoms to be on the lookout for include:
- Dryness
- Burning
- Grittiness
- Foreign body sensation
- Light sensitivity
- Vision that fluctuates with blinking
- An unstable tear film with a reduced breakup time
- Obstructed and/or inflamed meibomian glands
- Superficial punctate keratitis (SPK)
- Telangiectasia
- Conjunctival hyperemia
- Eyelash loss (madarosis)
- Tear film saponification
- Lash collarettes
- Notching or scalloping of the lid margin
- Lagophthalmos.
If any of these signs or symptoms and their corresponding OSD are identified, they should be addressed to ensure the ocular surface is prepared not only for surgery but the preoperative evaluation as well.
An example of a standard dry eye and OSD treatment regimen that addresses several common constitutive elements of a patient’s condition may include an
omega-3 fatty acid supplement to support meibomian gland health and meibum composition, lid hygiene to address any microbial blepharitis, such as that associated with bacterial or Demodex overgrowth, blink exercises to encourage proper blinking mechanics and tear secretion, warm compresses,
preservative-free artificial tears as a palliative treatment, and the use of a nighttime gel, ointment, or moisture chamber goggles if there is any nocturnal exposure.
Treating OSD with a limited amount of time
However, one element of
treating OSD prior to surgery that can pose a significant challenge is time itself. While the length of time between the diagnosis of visually significant cataracts to the preoperative visit and, ultimately, surgery can sometimes span several months, it is often truncated down to potentially weeks for a variety of reasons (i.e., insurance, travel, etc.).
“This is an incredibly short window of time in terms of dry eye and ocular surface disease treatment ahead of surgery.”
Dry eye is a chronic and progressive condition that typically develops over a long period of time, often years. Accordingly, it often requires a significant period of time for treatment to take effect. But this is an amount of time we may not have. Consequently, it is often necessary to be a bit more aggressive with initial
dry eye treatment when surgery is quickly approaching.
Using topical steroids to manage inflammation
For instance, if the patient has a significant inflammatory component to their dry eye, a
steroid pulse or taper will likely be necessary, at least initially, to quickly quell the ocular surface inflammation as immunomodulators can take weeks or even months to reach maximal effect.
9-11In such cases, it can be beneficial to start the patient on a steroid pulse or taper alongside an
immunomodulator like Xiidra (lifitegrast ophthalmic solution 5%, Novartis), Cequa (cyclosporine ophthalmic solution 0.09%, Sun Pharmaceuticals), or Restasis (cyclosporine ophthalmic emulsion 0.05%, Allergan).
This treatment combination quickly reduces preoperative inflammation while also allowing the immunomodulator time to reach maximal effect to provide long-term inflammatory control in the postoperative period and beyond.
Treating cataract patients with concomitant blepharitis
Microbial blepharitis is another key OSD-related concern in cataract surgery. Blepharitis is a common finding in patients with cataracts which tends to appear in later decades of life by the nature of the condition. Studies have shown that 84% of patients at age 60 have Demodex present, with that number reaching 100% at 70 years old and above,
12 and nearly 56% of patients with cataracts also have
Demodex blepharitis.
13It is not only the mites themselves that pose a potential challenge, as Demodex also harbor potentially problematic bacteria as well.
14-16 Given the proximity of the lid margin and lashes, where the bacteria and mites reside, to the surgical incision sites, the need to address these potential pathogens to avoid any surgical complications, such as serious infections like
endophthalmitis, is imperative to manage upfront.
17,18In fact, untreated blepharitis is one of the most common causes of cataract surgery cancellation.18,19 Thus, addressing blepharitis preoperatively is a crucial step in providing an avenue to safe and successful cataract surgery.20,21
While the use of routine lid hygiene, such as hypochlorous acid spray or a tea tree oil cleanser, should be implemented, in cases where the time until surgery is relatively short, the use of an adjunct microblepharoexfoliation treatment, like BlephEx (BlephEx) or NuLids PRO (NuSight Medical), can help quickly reduce the microbial burden on the lid margin and lashes, including associated proinflammatory debris including biofilm and lash collarettes.
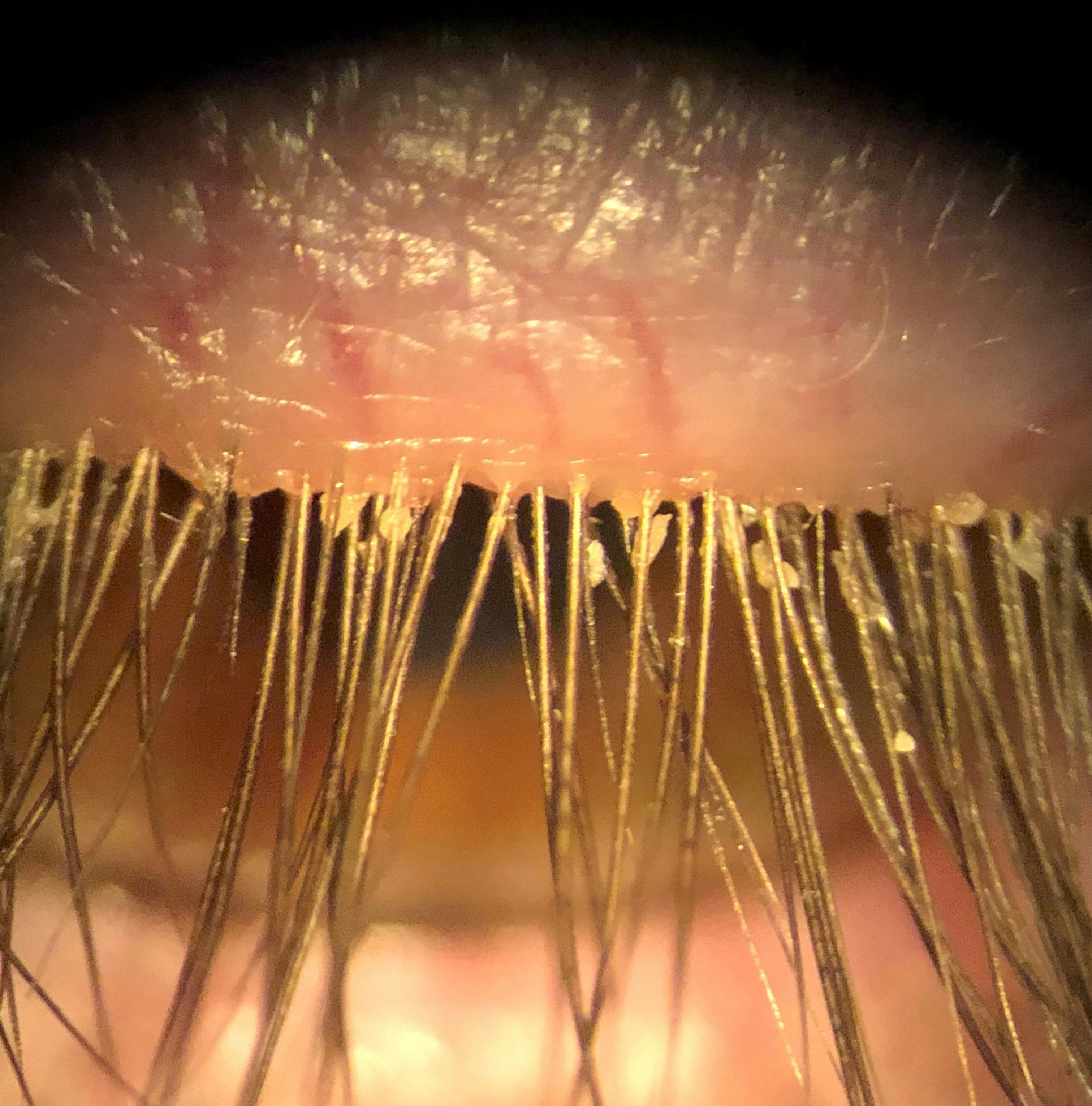
This can be particularly helpful in cases of Demodex blepharitis, as illustrated by Figure 2, as the minimum recommended treatment duration of the condition is 6 weeks, as this corresponds to two life cycles of the mites.22
Figure 2 is a clinical image of a patient’s lash margin with visible collarettes caused by Demodex blepharitis.
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO
Managing ahead: preoperative calculations and premium IOLs
The key to the successful refractive element of cataract surgery is
accurate preoperative IOL calculations.
23 To minimize the chance of an unexpected refractive outcome, referred to as “refractive surprise,” it is crucial to get these measurements as accurate as possible. The tear film-cornea interface provides nearly 70% of the refractive power of the eye; therefore, it is of paramount importance that the tear film be stable and of high quality when taking preoperative measurements for determining IOL power.
24Additionally, any surface disruption, such as SPK, should be treated to ensure measurements are obtained through a smooth optical surface. The importance of stabilizing the tear film in obtaining accurate preoperative measurements has been highlighted by studies showing that patients with
dry eye and short tear break-up times have reduced repeatability in corneal curvature radius and axial length measurements.
25Premium IOL selection for patients with ocular surface disease
Specific premium IOL designs of note in regard to dry eye are multifocal (MF) and
extended depth-of-focus (EDOF) IOLs. These IOLs are designed for patients who desire to be potentially free of spectacle wear and are willing to pay the associated out-of-pocket cost for these lenses.
However, this also means their expectations for their postsurgical vision are significantly higher than the monofocal lens candidate, and they may be even less likely to tolerate any deviation in their postoperative refractive status. So, as just mentioned, optimizing the ocular surface prior to obtaining preoperative IOL calculations can help increase the chance of obtaining the desired postoperative refractive outcome.
When it comes to
multifocal IOLs, the importance of managing dry eye and ocular surface disease does not simply end with successful preoperative measurements or even a spot-on postoperative refractive status. We are all aware of the “give and take” relationship that exists with certain IOL designs, and one of the tradeoffs for the ability to see at both distance and near with a MF or EDOF IOL is a reduction in contrast sensitivity.
26This is one of the reasons why hypercritical observers may not be the best candidates for MF or EDOF IOLs if they desire “perfect” vision after cataract surgery. This characteristic of IOLs takes on even greater importance in the context of dry eye and OSD. Seeing as these patients are already dealing with a decrease in contrast sensitivity, any degradation in visual quality due to unstable tear film caused by dry eye will only compound this visual reduction.8,27
The delicate psychological balance between surgery and OSD
So, even if the surgeon nails the refractive aspect for a MF or EDOF IOL case, this could be all for naught if the tear film is unstable. Experientially, this situation has created some of the most dissatisfied patients I have encountered, especially since they equate the paid out-of-pocket fee directly to the anticipated premium visual result.
Therefore, properly addressing any ocular surface issues before and after surgery is particularly important in
premium IOL patients, specifically those with MF or EDOF IOLs. Early identification of OSD can also help guide a patient in the IOL selection process by counseling them on the potential challenges posed by OSD to the optimal function of MF and EDOF IOLs.
Postoperative treatment of OSD in pseudophakic patients
Along the same lines, OSD management does not end after cataract surgery has been performed. Patients may experience MGD for months after cataract surgery, even if previously asymptomatic, which may be driven by surgically-related inflammation of the glands.
28 However, proactive
preoperative treatment of MGD has been shown to alleviate postoperative MGD, and treatment prior to surgery is actually more effective than therapy initiated postoperatively.
29“This once again underscores the importance of treating MGD and other OSD prior to cataract surgery.”
As mentioned, many patients who were previously asymptomatic begin to exhibit symptoms of
dry eye after surgery, so it is vital to provide targeted education about the nature of cataract surgery and dry eye to this subset of patients. The chief reason for this is that these patients will often criticize the surgery (and guilt by association, the surgeon, and the referring doctor) for directly causing their dry eye.
Invest time in patient education on OSD and cataract surgery
Further, patients even at times blame themselves for their OSD, as cataract surgery has an elective element, and they ultimately decided to proceed with the procedure. With this thought in mind, it can be helpful to explain that dry eye is a
chronic and progressive condition in a sympathetic manner.
For all intents and purposes, it was likely that their dry eye that had been slowly building for years, but the cataract surgery, like any surgery, can be a major stressor on the body and eye, so the surgery essentially “pushed” their dry eye over the edge from being an asymptomatic condition to a symptomatic one.
These patients likely would have developed symptomatic dry eye eventually, but the stress of cataract surgery was just the straw that broke the camel’s back, so to speak. Taking the time to explain this to a patient can have a
significant psychological benefit, as well as help them understand that this is a normal occurrence and not necessarily some unexpected adverse event. Additionally, even OSD patients who were previously well-managed will often experience a flare in their dry eye symptoms after cataract surgery.
So, it can be advantageous to discuss this possibility with these patients prior to surgery to let them know their dry eye may require a little more attention after surgery to get things back under control.
Final thoughts
Patients who have significant cataracts and are preparing for
cataract surgery commonly have OSD as well, whether it be symptomatic or asymptomatic. OSD can have a significant impact on postoperative visual outcomes as well as comfort.
If not addressed prior to surgery, patients are more likely to be dissatisfied with their surgical outcomes due to less-than-optimal refractive status, whether there be causality from
newly symptomatic dry eye or an exacerbation of existing dry eye.
Therefore, it is our role as ECPs to prepare these patients for surgery by addressing any dry eye or OSD prior to surgery, as well as providing postoperative ocular surface care, to ensure the best surgical and refractive outcomes that hopefully not only meet but exceed their expectations.