





Introduction
Today’s eyecare providers have an ever expanding plethora of options to address their patients’ uncorrected astigmatism. Between high index spectacle lenses, expanded parameters for toric soft contact lenses, and custom GP/scleral lenses, patients are no longer being left with uncorrected refractive error from astigmatism. This has also never been more true than in the context of cataract surgery, with increasing options for IOLs tailored for astigmats and presbyopes (soon to be pseudophakes). With cataract surgery being the most common ocular surgical procedure performed worldwide,1 IOL implantation has become a mainstay in addressing refractive error in addition to the cataract itself.
In this course, we’ll be discussing the importance of choosing the right IOL implant for our astigmatic patients undergoing cataract surgery and dive into three patient cases using toric lenses.
*Drs. Blecher, Farid, and Scott are paid consultants for Johnson & Johnson Surgical Vision Inc.
Background
Astigmatic refractive error results from irregular anatomy within various parts of the eye. Corneal astigmatism results from unequal curvature along the two principal meridians of the anterior (or posterior) cornea, commonly referred to as either with-the-rule (WTR) or against-the-rule (ATR) astigmatism. Lenticular astigmatism results from unequal curvatures of the front and back surfaces of the crystalline lens. Lastly, varying indices of refraction within the crystalline lens itself is known as internal or residual astigmatism.
The prevalence of astigmatism can be as high as 60% in the adult population and is generally WTR in nature.2 Based on ethnicity, some patient populations may have even greater amounts of astigmatism as compared to Caucasian subjects, namely Native American and Asian populations.2 Corneal curvature tends to shift in older adulthood, causing increasing amounts of ATR astigmatism, while internal astigmatism remains relatively stable.2
Chief Complaint
Patients with uncorrected astigmatism present with a wide range of visual symptoms. These can range from being completely asymptomatic to having debilitating blur, distortions, double vision, and photophobia (eg. increased glare at night).3 Astigmatic patients who develop significant cataracts can begin to re-experience all of these symptoms and more. Symptoms that were once alleviated through contact lens wear or spectacle correction may progressively return and persist.
Some patients’ cataracts are monitored over many years prior to needing surgery, while others tend to progress rapidly. When it comes to age-related cataracts, diabetes remains the greatest risk factor for developing them prematurely and/or progressing at a faster rate.2 It is not uncommon to see patients with uncontrolled type 2 diabetes needing cataract surgery earlier on in life, while their healthy counterparts may not need surgery until later in life.4
Treating Astigmatism in Cataract Surgery
Treating astigmatism in cataract surgery & choosing the right toric IOL
It is important for both the patient’s referring optometrist and the cataract surgeon to set clear expectations for patients undergoing cataract surgery. Many patients not only want to improve their visual function, but are also seeking to be less dependent on spectacle lens wear after cataract surgery. Patients desire the cosmetic and economic benefits to having satisfactory uncorrected vision postoperatively.
Numerous techniques have been developed and used to correct astigmatism during cataract surgery.7 These include selective positioning of the phacoemulsification incision, limbal/corneal relaxing incisions (typically along the steepest meridian of the cornea), and toric IOL implantation. Altering the shape of the cornea intraoperatively requires the surgeon to predict the healing pattern of the cornea, which can be a challenging task in some cases.
The use of toric IOLs has become an increasingly popular strategy to correct for astigmatism during cataract surgery. They provide optimal correction of the patient’s astigmatism while having a minimal impact on corneal curvature. While misalignment of a toric IOL can leave residual astigmatism, the enhanced rotational stability of newer toric IOL options is less likely to have this side effect.
After patients undergo cataract surgery, there is a brief window of time before the capsular bag condenses to enclose and secure the new IOL implant. It is during this time that rotation may occur. This is why it is important to wait at least a month before conducting a final post-op refraction, as this is the typical time frame for a full recovery after cataract surgery.8 In some cases, corneal healing can also leave the patient with varying degrees of residual corneal astigmatism as well.
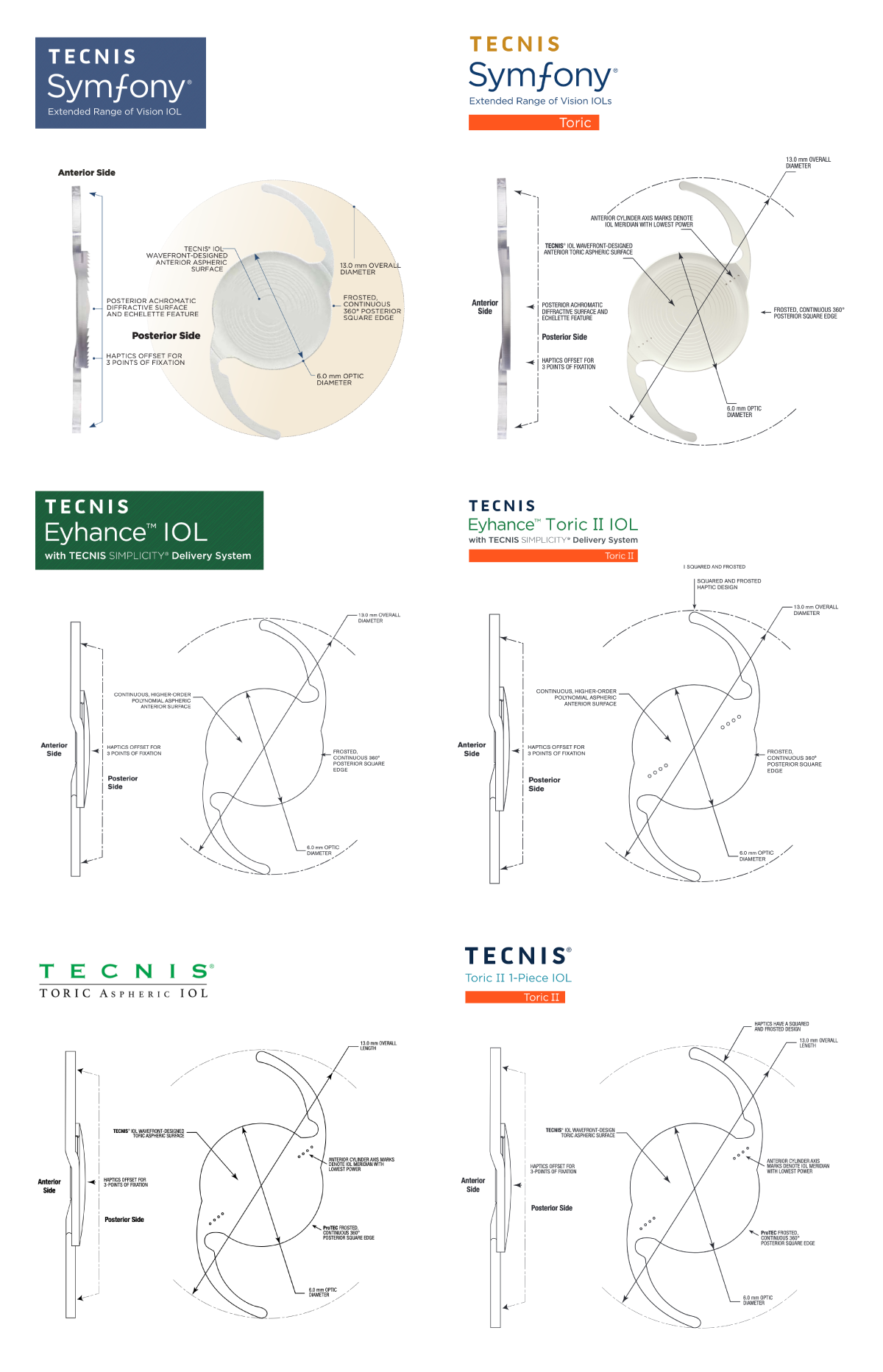
Knowing the lens types available and those your preferred surgeon uses will be helpful to have these discussions with your patients. Johnson & Johnson Vision has a variety of toric IOLs to meet most of your astigmatic patient’s needs.
Typically, if a patient has > 1.00D of corneal astigmatism, they could be considered a candidate for a toric IOL. This is best determined by comparing topography to biometry values.

Refer to the Directions for Use for a complete listing of Indications and Safety Information.
What are some of the primary reasons toric IOLs aren’t as commonly utilized?
With today’s plethora of new toric IOL options, patients with astigmatism are no longer left with large amounts of refractive error after cataract surgery. Prior to new advances in toric IOLs, surgeons may have been reluctant to use toric IOLs due to concerns of rotational stability. However, the TECNIS lenses showed that in >94% of patients at 6 months had <5' rotation.6 Between 35% and 40% of patients undergoing cataract surgery have astigmatism > 1.00D9 and up to 22% will have astigmatism > 1.5D.7
The proper implantation of a toric IOL requires significantly more precision than a conventional spherical IOL implant. Alignment of the toric IOL in relation to the patient’s astigmatic refractive error is of utmost importance.
What are the main reasons to consider toric IOL options/good candidates for toric IOL?
After considering their refractive error, ocular anatomy, personality type and visual priorities, choosing the right IOL is an integral part in providing a satisfactory surgical outcome for these patients. It is no surprise that patients are more satisfied with their cataract surgery when they can recognize improvements to their visual function and performance.10
There are several reasons to choose a toric IOL for patients undergoing cataract surgery. For starters, patients with an astigmatic refractive error of > 1.00D will typically benefit from a toric IOL implant. Good candidates for toric IOLs generally desire little or no dependence on spectacle lens correction after surgery. Patients with less particular, more open (Type B) personalities can also make better candidates for toric IOLs.
Some patients may be good candidates for cataract surgery, but would do better with a conventional spherical IOL implant. Other patients may still benefit from a toric IOL implant but should understand that they may still need to wear glasses for optimal vision postoperatively. Patients with preexisting ocular disease (eg. macular degeneration, glaucoma) may be poor candidates for toric IOLs.13 Patients with high amounts of irregular astigmatism, especially if they have keratoconus or pellucid marginal degeneration, are poor candidates for toric IOLs..13
Patients with Type A personalities should also understand that they may still be dependent on spectacle lens wear, regardless of which type of IOL they receive.
How do you present toric IOL as an option?
Discussing the patient’s anticipated functional visual goals post-operatively will be crucial for determining who is a good candidate for a toric IOL. This discussion should begin with the referring optometrist. As the patient is starting to have functional vision problems while performing their daily activities, discussing that cataract surgery is imminent and starting the conversation about what their postoperative visual goals are is a crucial first step. If the patient wants sharp distance vision and limited glare, they would be a good candidate for a toric IOL.
For example, long-haul truck drivers or previous emmetropes may be very bothered by poor distance contrast if left with residual astigmatism or fit with a multifocal IOL and will likely appreciate the toric correction. If a patient is a 2-3D myope and is happy with their uncorrected near vision before surgery, they may need a stronger reading add power for satisfactory vision postoperatively. This is true regardless of whether they’re left wearing spectacle/contact lenses, or receiving a multifocal/extended range IOL.
Patients need to understand that they have an option to correct astigmatism with a toric IOL during surgery, or will need to correct the astigmatism with contacts or spectacles after surgery.
What are the most important considerations and processes to take in order to ensure a good surgical and visual outcome?
Candidate selection is of utmost importance in positive post-surgical outcomes. Candidates with compounding ocular disease such as age-related macular degeneration, ocular surface disease, or diabetic retinopathy are contraindicated for toric IOLs. Those with milder or asymptomatic conditions such as epithelial basement membrane corneal dystrophy, mild epiretinal membrane or keratoconus may also lead to post-surgical problems.
After candidate selection, setting patient expectations would be the most important next step to post-surgical success. Explain to patients before their surgery that even if the goal of surgery is to be minimally dependent on glasses, there may still be activities where glasses are required. Helping patients understand that there will be a neuronal adaptation period (especially if they do a multifocal or toric multifocal lens) will ensure they do not think the surgery had a “bad” outcome. Letting the patient know that symptoms of glare or halos are possible post-op symptoms that could occur. Patients need to understand what expected side effects to anticipate ahead of time instead of trying to address them as they happen.
Lastly, ocular surface disease (OSD) and meibomian gland dysfunction (MGD) should be evaluated and treated in every surgical patient in order to receive optimal surgical outcomes. The ASCRS OSD Pre-Operative Algorithm has shown that OSD and MGD can alter the ocular surface, causing surgical measurements to be inaccurate.11 Treating OSD before surgical referral allows the eyecare team to optimize the ocular surface and increase the likelihood of accurate measurements. In one study, treating MGD in surgical patients before surgery correlated with a 40% change in surgical plan.12 Optometrists have a great opportunity to identify and provide patients with both treatment and education before their first appointment with the surgeon.
Are there any special considerations when it comes to multifocal torics? How do you go about the IOL selection process?
When helping a patient determine which intraocular lens choice would best suit their visual needs, it all depends on their post-surgical expectations and goals. Does the patient spend a lot of time outdoors? If so, all Johnson & Johnson Vision’s lens implants are UV blocking. Has this patient returned to your office dissatisfied in the past with progressive lenses or multiple glasses redos? This personality type may not be ideally suited for multifocal lenses where some degree of halos is expected at least in the short term. Ideally, you want to recommend multifocals and multifocal toric IOL options to those patients whose main priority is to limit the amount of time they need to wear glasses, even if that means sacrificing a little bit of vision in certain instances (eg. dim lit settings or when focusing on fine detail).
For the patient with > 1.00D corneal astigmatism who wants uncompromised distance vision and doesn’t mind wearing reading glasses (think people who drive long distances or do other primarily distance viewing tasks like certain sports or watching TV) the TECNIS® Toric II 1-Piece IOL may be the ideal recommendation. This could be used as a monovision design as well, especially for those who have opted for and previously done well with monovision contacts.
For those with <1.00D corneal astigmatism who want to see well at all distances and don’t mind reading glasses occasionally for fine detail, they may prefer the extended depth of focus IOL found in the TECNIS Symfony™. The extended depth of focus virtually eliminates poor contrast and difficulty transitioning between zones of previous multifocal IOL designs. For those without significant corneal astigmatism but requiring detailed near vision range, the TECNIS® Multifocal IOL is available in near power ranges from +2.75 to +4.00.
For those patients with >1.00D corneal astigmatism and visual demands primarily at intermediate and distance locations, they would typically do very well with a TECNIS Symfony™ Toric lens to correct for their corneal astigmatism as well as their distance, intermediate, and near demands. Lastly, for those with significant corneal astigmatism but higher near demands, they may be better suited to a TECNIS® Multifocal Toric II lens with astigmatism correction and all-range viewing with a particular focus on demanding near work. This lens type is available in two different near ADD powers (+2.75 and +3.25)
Keep in mind that all of these lenses can be used in combination as well. So for example, a patient implanted with a TECNIS Symfony™ or TECNIS Symfony™ Toric in the first eye but still struggling with near tasks such as reading the standard J5 font on a smartphone, may be recommended a TECNIS® Multifocal Toric for the other eye. This may provide excellent vision at all distances after adaptation.
Due to the chromatic aberration compensation inherent in the TECNIS Symfony™ lens, auto-refractors (including aberrometers) may yield erroneous refractive results. Instead, Johnson & Johnson Vision recommends a post-op refraction to be done in a specific series of steps to determine the best refraction for those with TECNIS Symfony™ IOL.
Patient Cases
Case #1 - TECNIS Symfony™ Toric
Mark H. Blecher, MD - Co-Director of the Cataract and Primary Eye Care Service at Wills Eye Hospital. Dr. Blecher is a paid consultant of Johnson & Johnson Surgical Vision Inc.
Pre Operative Exam
A 63 y/o Female presents with chief complaint of constant blur at all distances, progressive dry eye symptoms OU and decreased tolerance to Gas Permeable contact lenses. Her exam findings were significant for 3+ nuclear cataracts OU, all other testing unremarkable - OCT, corneal topography, IOLMaster.
Her visual goals were to gain independence from her GP contact lenses and have satisfactory uncorrected vision at all distances after cataract surgery. She was also an avid motorcyclist—a hobby I took into consideration when deciding on the best lens to use.
Surgical Planning
The patient understood that she would need to be out of her GP contact lenses for at least a month to stabilize her corneal topography measurements and that prior to cataract surgery, her surgeon would like to see two serial K readings that are stable over time.
- MRx
- OD: +4.50 + 1.50 x 83 20/50
- OS: +5.25 + 1.00 x 90 20/50
- K’s
- OD: 41.41/43.77 x 83, OS: 41.82/44.12 x 94
The Holladay® II formula and Optiwave Refractive Analysis (ORA) System™ Technology were both used to assist with optimal IOL selection and to ensure satisfactory post-operative refractive status. The Holladay II calculation advised a +29.00D IOL power.
The ORA System™ Technology device attaches to the surgical microscope and utilizes wavefront aberrometry to measure the patient’s refractive power once the cataract is removed. The ORA System™ Technology assists the surgeon in the real-time assessment of the patient’s refractive status intraoperatively.

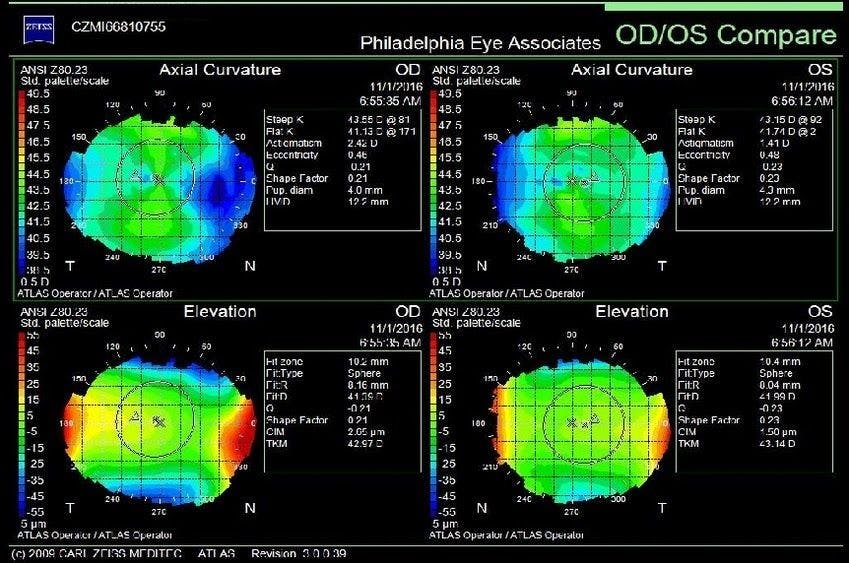
Image courtesy of Mark H. Blecher, MD
For this patient, we opted for the TECNIS Symfony™ Toric Lens implant in both eyes (model ZXT150 +28.50 OD, +29.00 OS).
Post Operative Exam
- Refraction, OD: Plano 20/20+
- Refraction OS: Plano 20/20+
- Near J1 OU @ 14” 20/20 vision
This patient was thrilled with their vision and surgical outcome. As with most patients undergoing cataract surgery, they are looking to improve their vision and gain more independence from spectacle lens wear, both of which we were able to achieve with this patient.
Takeaways
The TECNIS Symfony™ Toric IOL has all the performance of TECNIS Symfony™ with the addition of astigmatism correction. Pre-op planning is the same for both the TECNIS Symfony™ and Toric lenses. Similarly, implantation is the same as for the Toric lens; in my opinion, however, the Barrett Toric Calculator is more ideal for determining proper toric IOL lens alignment.
Case #2 - TECNIS Symfony™ Toric and TECNIS® Multifocal Toric II IOLs
Marjan Farid, MD - Professor of Ophthalmology, Director of Cornea, Cataract, and Refractive Surgery, Vice-Chair of Ophthalmic Faculty - Gavin Herbert Eye Institute at UC Irvine Health. Dr. Farid is a paid consultant of Johnson & Johnson Surgical Vision Inc.
Pre Operative Exam
A 72 y/o Female presents with significant decreased vision OU and was found to have bilateral 2+ nuclear cataracts. She is a therapist and much of her work is at the computer (On Zoom) meeting her patients. She also charts on paper and typically takes off her glasses when charting.
- Preoperative MRx: OD: -2.75 + 1.50 x 90 OS: -3.25 + 1.50 x 100 OS
- Preoperative biometry with: OD: 1.25 D cyl at 95 deg, OS 1.35 D cyl at 100 deg
The patient’s topography astigmatism assessment was fairly consistent with biometry measurements.

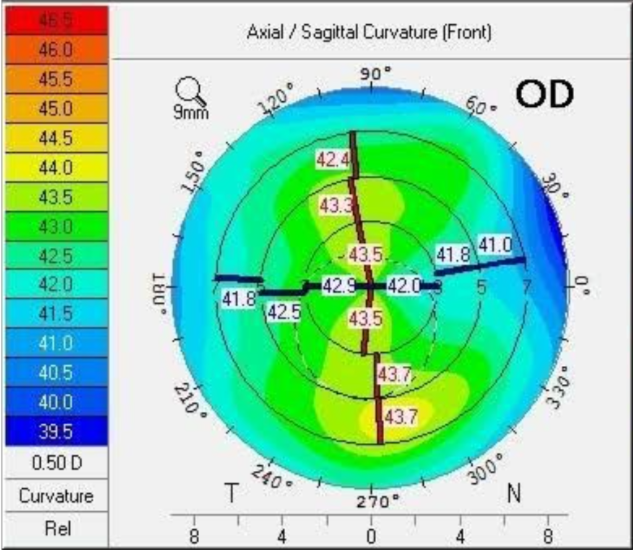
Image courtesy of Marjan Farid, MD
Surgical Planning
The patient was scheduled for cataract extraction with the TECNIS Symfony™ Toric IOL OD first followed by the OS 1 week later. We chose this lens to maximize her distance and intermediate vision.
Post Operative Exam
Right eye
Following cataract surgery in her right eye with TECNIS Symfony™ Toric, the patient was satisfied with her distance and computer vision but dissatisfied with her uncorrected near vision. She stated that she was unable to do her charting, but does not want to wear reading glasses and prefers more near focus after cataract surgery in the left eye.
Based on this update from the patient, a decision was made to use the TECNIS® Multifocal Toric II with 3.25 add for her left eye cataract surgery. After both eyes underwent cataract surgery, the patient was much happier with her uncorrected vision at distance and near with both eyes open. On post-op refraction, no manifest residual astigmatism was present, and uncorrected visual acuity was 20/20 in each eye, with near vision J3 and J1 in the right eye and left eye respectively.
Takeaways
It is important to personalize vision related goals to maximize range of vision based on patient’s expectations and lifestyle. If a patient is a -2 to -3 myope preoperatively (and before they developed a cataract), they will typically require a greater reading add power as they are accustomed to good near focus prior to cataract formation.
The TECNIS® Multifocal Toric II now available for eyes that need a toric IOL and greater near add in their presbyopic correcting IOL.
Case #3 - CATALYS® Precision Laser System cOS 6.0
Wendell Scott, MD - Ophthalmologist at Mercy Hospital, Springfield Missouri. Dr. Scott is a paid consultant of Johnson & Johnson Surgical Vision Inc.
Pre Operative Exam
A 75 year-old farmer referred for progressive decreased vision that is interfering with driving, especially with night-time glare.
BCVA:
- OD: +0.50 +2.00 x 013, 20/40
- OS: +1.50 +1.25 x 169, 20/40
- Glare vision testing OD: 20/70, OS: 20/60.
The patient has 2+ nuclear sclerosis and 2+ cortical cataracts in each eye. His examination is otherwise unremarkable.
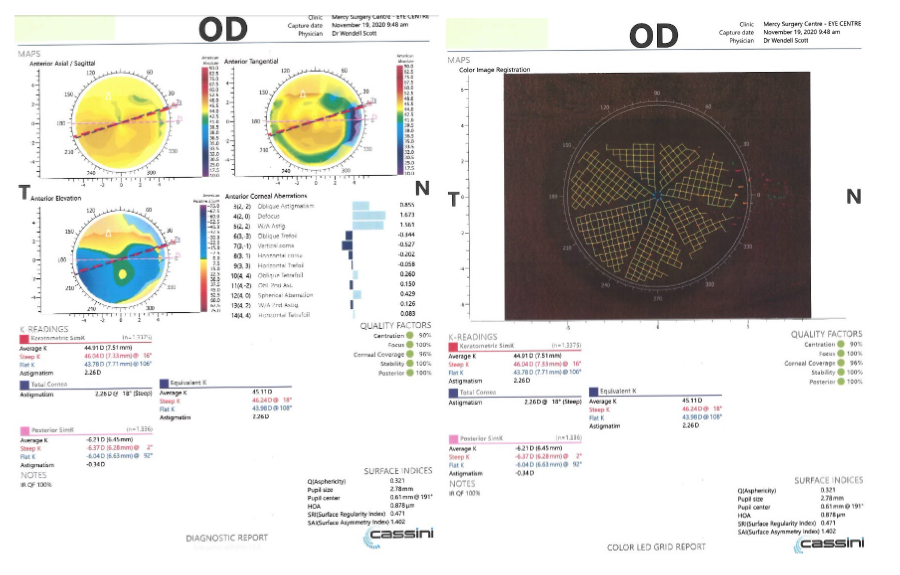
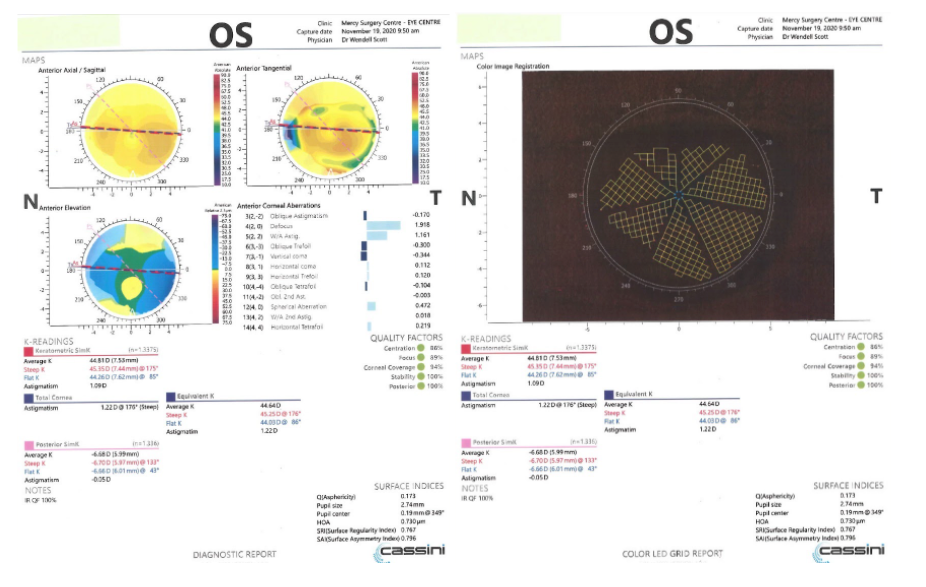
A review of the pre-operative tests include the Zeiss IOLMaster® 700, Nidek® OPD, and the Cassini® topographer. I look at all three comparing the anterior/SIM-K®, and at the IOLMaster® and Cassini® for the TK and TCA, respectively. On the IOLMaster® I note the CCT and the CW Chord (angle kappa), the OPD wavefront analysis and RMS, and the Cassini® HOA, SRI, SAI, and IR QF. Based on the exam and the pre-operative tests, I decide what the IOL choices are for this patient.

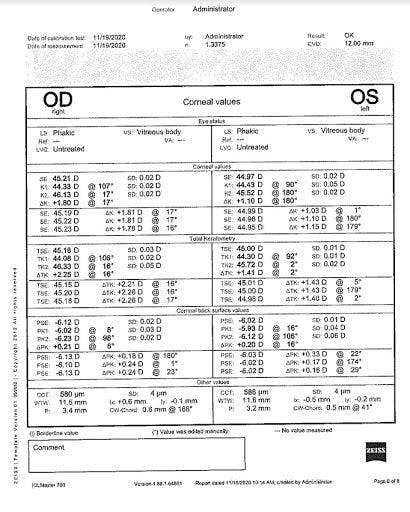
Image courtesy of Wendell Scott, MD
I let the patient know that he has cataracts and that the cataracts are the cause of his decreased vision and glare. I explain that we use the laser for cataract surgery because we can make precise incisions in the cataract capsule and that the laser also softens the lens so that we can remove it in a way that is more gentle on the eye. Also, once the cataract is removed, we place a lens implant in and that there are different choices. The single focus implant is covered by insurance and will help restore the vision, but he will still need glasses all the time. He also has astigmatism, which I explain as the cornea being more oval and not round, thus preventing the light from being sharply focused. This is true at all distances and one of the reasons he needs glasses all the time. Almost everyone has some measurable amount of astigmatism and that if it is low enough, it doesn’t have much effect. Unfortunately, his is higher and is likely to have an effect. I also explain that there are implants that have a range of vision, meaning less dependence on glasses. His choice is a single vision implant and glasses, or an implant called a toric lens for astigmatism, or an implant that has astigmatism correction in it plus a range of vision.
What are the patient’s goals after surgery? Do they mind wearing glasses or is their goal to reduce or eliminate the need for glasses? If I have determined that their eyes are otherwise healthy and that we have reliable measurements, I tell them that they are good candidates for all three choices and find out more about what their near and intermediate vision needs are. This patient works on his farm equipment. He reads normal print approximately one hour per day. He has a smartphone and checks his email on a desktop computer. He occasionally goes fly-fishing.
In this case, the patient does not mind wearing glasses, but he is interested in making his vision as sharp and clear as possible. I explain that reducing astigmatism is the best way to sharpen his vision. Although he will still need glasses, he will reduce how much prescription he needs in his glasses, especially at distance. He says that many of his friends only need reading glasses after surgery. In my opinion, this is true for 80% of patients who don’t have significant astigmatism, but I tell this patient that in his case, he would probably need the glasses for distance if the sharpness of focus is important to him. I truly believe that the toric IOL offers “value” and is worth it and I think patients can see that I mean it. With this assurance, he elects to proceed with a toric IOL.
Have I promised too much? In our practice, we will include laser PRK for patients that have a significant residual refractive error at no additional charge. We do this for all premium IOL patients. In my experience, I’ve found that the need for this is especially rare with the toric IOL where over 90% of patients have minimal refractive error. As I discussed, our goal is to reduce the astigmatism to a level low enough that it is not significant, not eliminate it. It is an important point for the referring doctor and the patient so that we comfortably meet expectations.

Images courtesy of Wendell Scott, MD
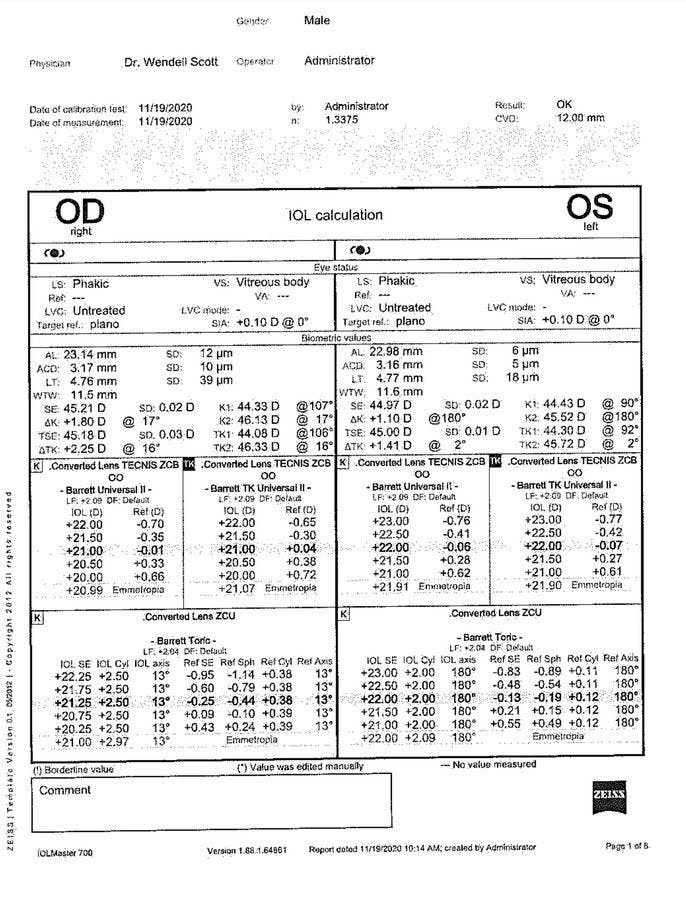
I usually do the non-dominant eye first, so let’s look at the toric planning for the left eye.
- Current glasses RX: +1.25 @ 169
- Nidek® OPD: +1.25 @ 179
- IOLMaster® 700 anterior K: +1.10 @ 180
- IOLMaster® 700 TK (total cornea): +1.41 @ 2
- Cassini® SIM-K®: +1.09 @ 175
- Cassini® TCA (total corneal astigmatism): +1.22 @ 176 degrees
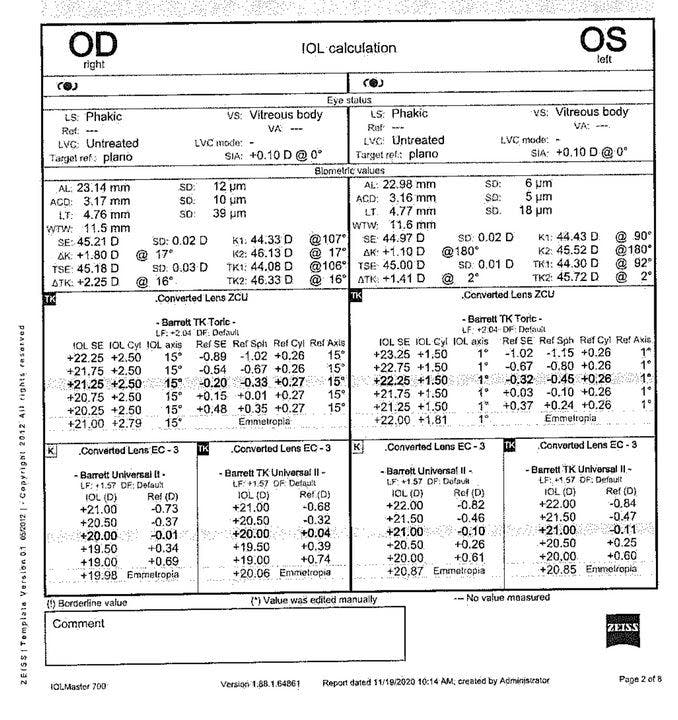
I think the glasses RX is the least helpful, but it is reassuring if the axis is in the same general direction (ATR, WTR, or oblique). Next, I look at the anterior Ks of the OPD, IOLMaster®, and Cassini® and see that they are relatively close. At this point, you would expect the IOLMaster® TK and the Cassini® TCA, both of which measure the posterior astigmatism, to have a higher magnitude of astigmatism due to the posterior contribution. The finding confirms this. In the end, you have to pick a number to plug into the TECNIS® Toric calculator. Now that we have the CATALYS® Precision Laser System cOS 6.0 in combination with the Cassini® Ambient, I prefer to import the Cassini® iris registration and Ks. In this case, either the SIM-K® or the TCA will give similar results. However, remember that the PCA “No or Yes” must be selected. If you use the SIM-K®, you would select “Yes” so that the PCA adjustment would be included in the calculation. If you use the TCA Ks, select “No” because the TCA Ks already include posterior astigmatism as measured directly. An example of the calculation using the TCA Ks with “No” selected under PCA is provided. A ZCU150 @ 176 degrees is selected, which is the closest value to no residual refraction without flipping the axis. Some surgeons prefer to select an IOL that will leave a slight residual WTR result. This may be preferable in a younger patient due to the natural drift to more ATR with time.
Images courtesy of Wendell Scott, MD
Surgical Planning
So, once we have selected the IOL, what do we do in the OR? With the Cassini® Ambient data input into CATALYS® Precision Laser System cOS 6.0, we no longer have to mark the patient manually. Before, we either marked the patient sitting up at 0 and 180 as reference marks, or we had the patient lay down under the microscope before the prep and use the Callisto to mark 0 and 180. Either way, inaccurate, thick marks are a risk. With the Cassini® iris registration, those days and inefficiencies are gone. The iris registration is performed during the OCT and the match accuracy is confirmed. This allows us to confidently place our axis-dependent toric marks, as well as the incision and paracentesis. The toric marks are distinct and are still visible for at least 3 months, based on our documented experience. We have minimized the amount of cornea treated to 20% with the lowest energy possible (see settings). The “marks” are actually a thin column of air in the mid-stroma. This allows them to be more distinct with less surrounding whitening at the border of the mark. It also is reassuring to know that the marks have no refractive effect since they are affecting significantly less stroma than the pre-approval studies showing no effect. An advantage of using cornea marks vs capsule tags or notches is that the axis of the cornea marks will not be altered by capsule fibrosis. They remain independent and can be used to verify the position of the intended IOL placement for months, if not longer.

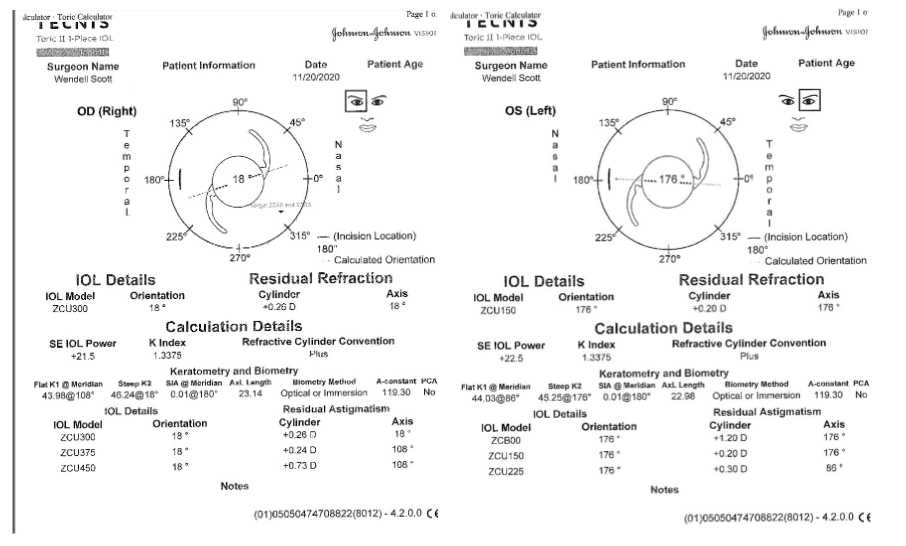
Image courtesy of Wendell Scott, MD
Once the cataract is removed and the IOL placed, the viscoelastic is removed and the final IOL alignment made. Depending on the microscope you are using, you can use the patient fixation of the light source as the visual axis. The cornea marks will be aligned or parallel, allowing for precise placement.
Post Operative Exam
Post-operatively, our patients are seen the same-day at least 2 hours after surgery if time allows or the next AM. (It is necessary for the patients to wait in order to catch any post-op IOP increases. We give the patient a drop of brimonidine at the end of surgery. If they are going to be seen the next day instead of the same-day, we send it home with them and ask that they put a drop in at bedtime.) The presence of the cornea marks can immediately be compared to the IOL, verifying the axis position.
Patients are then brought back for follow-up one week after their surgery. For this patient, surgery was performed first on the left eye (as mentioned earlier, the non-dominant eye), before moving to the right eye.
- 1 week post-op without correction: OS 20/25 and with -0.50 +0.25 x 165 degrees = 20/20
- 1 week post-op without correction: OD 20/20 plano
Takeaways
Patients undergoing cataract surgery now have myriad options available to them when it comes to the correction of astigmatism and independence from corrective lens wear. Adding the CATALYS® cOS 6.0 astigmatism planning features further streamlines this workflow and provides more accurate data at the start of my surgery. Never before have so many IOL options been available to meet the unique visual demands of each patient undergoing cataract surgery today.
Conclusion
Thanks to Johnson & Johnson Vision’s innovative IOL implant technologies, there are several IOL options to address patient's desires to minimize or eliminate astigmatism.
References
- Grzybowski A & Kanclerz P. (2019). Recent Developments in Cataract Surgery. In Grzybowski, A, ed. Current Concepts in Ophthalmology. Switzerland: Springer Nature; 2020: 55-97. 10.1007/978-3-030-25389-9_3.
- Read, S.A., Collins, M.J. and Carney, L.G. (2007), A review of astigmatism and its possible genesis. Clinical and Experimental Optometry, 90: 5-19. https://doi.org/10.1111/j.1444-0938.2007.00112.
- Nazario B. Astigmatism: Causes, Symptoms, Diagnosis, and Treatment. Astigmatism. https://www.webmd.com/eye-health/astigmatism-eyes. Published November 9, 2020.
- Kiziltoprak H, Tekin K, Inanc M, Goker YS. Cataract in diabetes mellitus. World journal of diabetes. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6422859/#:~:text=Several%20
clinical%20studies%20 have%20reported,under%20the%20age%20of%2065. Published March 15, 2019. - Nirmalan PK, Robin AL, Katz J, et al. Risk factors for age related cataract in a rural population of southern India: the Aravind Comprehensive Eye Study. Br J Ophthalmol. 2004;88(8):989-994. doi:10.1136/bjo.2003.038380
- Waltz KL, Featherstone K, Tsai L, Trentacost D. Clinical Outcomes of TECNIS® Toric Intraocular Lens Implantation after Cataract Removal in Patients with Corneal Astigmatism. American Academy of Ophthalmology. https://www.aaojournal.org/article/S0161-6420(14)00543-0/fulltext. Published November 17, 2014.
- Buckhurst PJ, Wolffsohn JS, Davies LN, Naroo SA. Surgical correction of astigmatism during cataract surgery. Clin Exp Optom. 2010;93(6):409-418. doi:10.1111/j.1444-0938.2010.00515.
- Haddrill M and Slonim C. Cataract surgery recovery: 8 tips to minimize recovery time. All About Vision. https://www.allaboutvision.com/conditions/cataract-surgery-recovery.htm
- Núñez MX, Henriquez MA, Escaf LJ, et al. Consensus on the management of astigmatism in cataract surgery. Clin Ophthalmol. 2019;13:311-324. Published 2019 Feb 11. doi:10.2147/OPTH.S178277
- Samadi B, Lundström M, Kugelberg M. Improving Patient-Assessed Outcomes after Cataract Surgery. European Journal of Ophthalmology. 2017;27(4):454-459. doi:10.5301/ejo.5000927
- Starr C, Gupta P, Farid M, Beckman K, Chan C, FRCSC, Yeu E, Gomes J, Ayers B, Berdahl J, Holland E, Kim T, Francis M, the ASCRS Cornea Clinical Committee. An algorithm for the preoperative diagnosis and treatment of ocular surface disorders. ASCRS and ESCRS. 2019; 45(5) : 669-684
- Matossian CA. Effect of thermal pulsation system treatment on keratometry measurements prior to cataract surgery. Presented at: American Society of Cataract and Refractive Surgery annual meeting; May 3-7, 2019; San Diego.
- Jordan L, ed. Premium IOLs: How to Spot Poor Candidates. Review of Ophthalmology. http://www.reviewofophthalmology.com/article/premium-iols-how-to-spot-poor-candidates. Published January 10, 2018.
PP2021MLT4977
Indications and Important Safety Information
INDICATIONS and IMPORTANT SAFETY INFORMATION for TECNIS SYMFONY™ and TECNIS SYMFONY™ TORIC EXTENDED RANGE OF VISION IOLs
Rx Only
INDICATIONS: The TECNIS Symfony™ Extended Range of Vision IOL, Model ZXR00, is indicated for primary implantation for the visual correction of aphakia, in adult patients with less than 1 diopter of pre-existing corneal astigmatism, in whom a cataractous lens has been removed. The TECNIS Symfony™ Toric Extended Range of Vision IOLs, Models ZXT150, ZXT225, ZXT300, and ZXT375, are indicated for primary implantation for the visual correction of aphakia and for reduction of residual refractive astigmatism in adult patients with greater than or equal to 1 diopter of preoperative corneal astigmatism, in whom a cataractous lens has been removed. These models of IOLs, ZXR00, ZXT150, ZXT225, ZXT300, and ZXT375, mitigate the effects of presbyopia by providing an extended depth of focus. Compared to an aspheric monofocal IOL, these models of IOLs provide improved intermediate and near visual acuity, while maintaining comparable distance visual acuity. These models of IOLs are intended for capsular bag placement only.
WARNINGS: Patients with any of the conditions described in the Directions for Use may not be suitable candidates for an intraocular lens because the lens may exacerbate an existing condition, may interfere with diagnosis or treatment of a condition, or may pose an unreasonable risk to the patient’s eyesight. Lenses should not be placed in the ciliary sulcus. May cause a reduction in contrast sensitivity under certain conditions, compared to an aspheric monofocal IOL; fully inform the patient of this risk before implanting the lens. Special consideration should be made in patients with macular disease, amblyopia, corneal irregularities, or other ocular disease. Inform patients to exercise special caution when driving at night or in poor visibility conditions. Some visual effects may be expected due to the lens design, including: a perception of halos, glare, or starbursts around lights under nighttime conditions. These will be bothersome or very bothersome in some people, particularly in low-illumination conditions, and on rare occasions, may be significant enough that the patient may request removal of the IOL.
Rotation of the TECNIS Symfony™ Toric IOLs away from their intended axis can reduce their astigmatic correction, and misalignment ˃30° may increase postoperative refractive cylinder. If necessary, lens repositioning should occur as early as possible prior to lens encapsulation.
PRECAUTIONS: Interpret results with caution when refracting using autorefractors or wavefront aberrometers that utilize infrared light, or when performing a duochrome test. Confirmation of refraction with maximum plus manifest refraction technique is recommended. The ability to perform some eye treatments (e.g. retinal photocoagulation) may be affected by the optical design. Target emmetropia for optimum visual performance. Care should be taken to achieve IOL centration, as lens decentration may result in a patient experiencing visual disturbances under certain lighting conditions.
For the TECNIS Symfony™ Toric IOL, variability in any preoperative surgical parameters (e.g. keratometric cylinder, incision location, surgeon’s estimated surgically induced astigmatism and biometry) can influence patient outcomes. Carefully remove all viscoelastic and do not over-inflate the capsular bag at the end of the case to prevent lens rotation.
SERIOUS ADVERSE EVENTS: The most frequently reported serious adverse events that occurred during the clinical trial of the TECNIS Symfony™ lens were cystoid macular edema (2 eyes, 0.7%) and surgical reintervention (treatment injections for cystoid macular edema and endophthalmitis, 2 eyes, 0.7%). No lens-related adverse events occurred during the trial.
ATTENTION: Reference the Directions for Use for a complete listing of Indications and Important Safety Information.
INDICATIONS AND IMPORTANT SAFETY INFORMATION FOR THE TECNIS® Multifocal of 1-Piece IOLs
Rx Only
INDICATIONS: The TECNIS® Multifocal 1-Piece intraocular lenses are indicated for primary implantation for the visual correction of aphakia in adult patients with and without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire near, intermediate, and distance vision with increased spectacle independence. The intraocular lenses are intended to be placed in the capsular bag.
WARNINGS: Physicians considering lens implantation under any of the conditions described in the Directions for Use should weigh the potential risk/benefit ratio prior to implanting a lens. Some visual effects associated with multifocal IOLs may be expected because of the superposition of focused and unfocused images. These may include a perception of halos/glare around lights under nighttime conditions. It is expected that, in a small percentage of patients, the observation of such phenomena will be annoying and may be perceived as a hindrance, particularly in low illumination conditions. On rare occasions, these visual effects may be significant enough that the patient will request removal of the multifocal IOL. Contrast sensitivity is reduced with a multifocal lens compared to a monofocal lens. Therefore, patients with multifocal lenses should exercise caution when driving at night or in poor visibility conditions. Patients with a predicted postoperative astigmatism >1.0D may not be suitable candidates for multifocal IOL implantation since they may not fully benefit from a multifocal IOL in terms of potential spectacle independence. Care should be taken to achieve centration, as lens decentration may result in patients experiencing visual disturbances, particularly in patients with large pupils under mesopic conditions. Multifocal IOL implants may be inadvisable in patients where central visual field reduction may not be tolerated, such as macular degeneration, retinal pigment epithelium changes, and glaucoma. Patients with certain medical conditions may not be suitable candidates for IOLs. Consult the Directions for Use for more information.
PRECAUTIONS: Prior to surgery, the surgeon must inform prospective patients of the possible risks and benefits associated with the use of this device and provide a copy of the patient information brochure to patient. There were no patients 21 years old or younger included in the clinical studies; therefore there are insufficient clinical data to demonstrate safety and effectiveness in this age group. The central one millimeter area of the lens creates a far image focus, therefore patients with abnormally small pupils (~1mm) should achieve, at a minimum, the prescribed distance vision under photopic conditions; however, because this multifocal design has not been tested in patients with abnormally small pupils, it is unclear whether such patients will derive any near vision benefit. Autorefractors may not provide optimal postoperative refraction of multifocal patients; manual refraction is strongly recommended. In contact lens wearers, surgeons should establish corneal stability without contact lenses prior to determining IOL power. Care should be taken when performing wavefront measurements as two different wavefronts are produced (one will be in focus (either far or near) and the other wavefront will be out of focus); therefore incorrect interpretation of the wavefront measurements is possible. The long-term effects of intraocular lens implantation have not been determined; therefore implant patients should be monitored postoperatively on a regular basis. Secondary glaucoma has been reported occasionally in patients with controlled glaucoma who received lens implants. The intraocular pressure of implant patients with glaucoma should be carefully monitored postoperatively. Do not resterilize or autoclave. Use only sterile irrigating solutions such as balanced salt solution or sterile normal saline. Do not store in direct sunlight or over 45°C (113°F). Emmetropia should be targeted as this lens is designed for optimum visual performance when emmetropia is achieved. Please refer to the specific instructions for use provided with the insertion instrument or system for the amount of time the IOL can remain folded before the IOL must be discarded. When the insertion system is used improperly, the haptics of the IOL may become broken. Please refer to the specific instructions for use provided with the insertion instrument or system.
ADVERSE EVENTS: The most frequently reported adverse event that occurred during the clinical trials of the TECNIS® Multifocal lenses was surgical re-intervention, most of which were non-lens-related. Lens-related re-interventions occurred at a rate of 0.6% to 1.0%. Other surgical re-interventions included lens exchanges (for incorrect IOL power), retinal repair, ruptured globe repair, macular hole repair, removal of retained lens material, treatment injections for cystoid macular edema and iritis, and blepharoplasty.
ATTENTION: Reference the Directions for Use for a complete listing of Indications and Important Safety Information.
INDICATIONS AND IMPORTANT SAFETY INFORMATION FOR THE TECNIS® Toric II 1-Piece IOL INDICATIONS AND IMPORTANT SAFETY INFORMATION
Rx Only
INDICATIONS
The TECNIS® Toric II 1-Piece IOL posterior chamber lens is indicated for the visual correction of aphakia and pre-existing corneal astigmatism of one diopter or greater in adult patients with or without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire improved uncorrected distance vision, reduction in residual refractive cylinder, and increased spectacle independence for distance vision. The device is intended to be placed in the capsular bag.
WARNINGS
Physicians considering lens implantation should weigh the potential risk/benefit ratio for any circumstances described in the TECNIS® Toric II 1-Piece IOL Directions for Use that could increase complications or impact patient outcomes. The clinical study did not show evidence of effectiveness for the treatment of preoperative corneal astigmatism of less than one diopter. The TECNIS® Toric II 1-Piece IOL should not be placed in the ciliary sulcus. Rotation of the TECNIS® Toric II 1-Piece IOL away from its intended axis can reduce its astigmatic correction. Misalignment greater than 30° may increase postoperative refractive cylinder.
PRECAUTIONS
Accurate keratometry and biometry in addition to the use of the TECNIS® Toric Calculator (www.TecnisToricCalc.com) are recommended to achieve optimal visual outcomes. The safety and effectiveness of the toric intraocular lens have not been substantiated in patients with certain preexisting ocular conditions and intraoperative complications. Refer to the TECNIS® Toric II 1-Piece IOL Directions for Use for a complete description of the preexisting conditions and intraoperative complications. All preoperative surgical parameters are important when choosing a toric lens for implantation. Variability in any of the preoperative measurements can influence patient outcomes. All corneal incisions were placed temporally in the clinical study. When the insertion system is used improperly, the haptics of the TECNIS® Toric II 1-Piece IOL may become broken. Please refer to the specific instructions for use provided with the insertion instrument or system. Do not reuse, resterilize, or autoclave.
ADVERSE EVENTS
The most frequently reported cumulative adverse event that occurred during the TECNIS® Toric 1-Piece IOL clinical trial was surgical re-intervention which occurred at a rate of 3.4% (lens repositioning procedures and retinal repair procedures).
ATTENTION
Reference the Directions for Use labeling for a complete listing of Indications and Safety Information.


INDICATIONS AND IMPORTANT SAFETY INFORMATION FOR THE CATALYS® PRECISION LASER SYSTEM
Rx only
INDICATIONS: The CATALYS® Precision Laser System is indicated for use in patients undergoing cataract surgery for removal of the crystalline lens. Intended uses in cataract surgery include anterior capsulotomy, phacofragmentation, and the creation of single-plane and multi-plane arc cuts/incisions in the cornea, each of which may be performed either individually or consecutively during the same procedure.
CONTRAINDICATIONS: The CATALYS® System is contraindicated in patients with corneal ring and/or inlay implants, severe corneal opacities, corneal abnormalities, significant corneal edema or diminished aqueous clarity that obscures OCT imaging of the anterior lens capsule, patients younger than 22 years of age, descemetocele with impending corneal rupture, and any contraindications to cataract surgery.
WARNINGS: Prior to INTEGRAL GUIDANCE System imaging and laser treatment, the suction ring must be completely filled with sterile buffered saline solution. If any air bubbles and/or a meniscus appear on the video image before treatment, do not initiate laser treatment. Before initiating laser treatment, inspect images created from the OCT data, surface fits, and overlaid pattern in both axial and sagittal views, and review the treatment parameters on the Final Review Screen for accuracy. Safety margins for all incisions are preserved only if Custom Fit Adjustments to ocular surface(s) are applied in accordance with the instructions for use. Purposeful misuse of the Custom Fit Adjustment to ocular surfaces can result in patient injury and complication(s), and therefore must be avoided. Standard continuous curvilinear capsulorhexis (CCC) surgical technique must be used for surgical removal of the capsulotomy disc. The use of improper capsulotomy disc removal technique may potentially cause or contribute to anterior capsule tear and/or a noncircular, irregularly shaped capsulotomy. Verify that the suction ring is correctly connected to the disposable lens component of the LIQUID OPTICS Interface during the initial patient docking procedure.
PRECAUTIONS: The CATALYS® System has not been adequately evaluated in patients with a cataract greater than Grade 4 (via LOCS III); therefore no conclusions regarding either the safety or effectiveness are presently available. Cataract surgery may be more difficult in patients with an axial length less than 22 mm or greater than 26 mm, and/or an anterior chamber depth less than 2.5 mm due to anatomical restrictions. Use caution when treating patients who may be taking medications such as alpha blockers (e.g. Flomax®) as these medications may be related to Intraoperative Floppy Iris Syndrome (IFIS); this condition may include poor preoperative dilation, iris billowing and prolapse, and progressive intraoperative miosis. These conditions may require modification of surgical technique such as the utilization of iris hooks, iris dilator rings, or viscoelastic substances. Surgical removal of the cataract more than 30 minutes after the laser capsulotomy and laser lens fragmentation has not been clinically evaluated. The clinical effects of delaying surgical removal more than 30 minutes after laser anterior capsulotomy and laser lens fragmentation are unknown. The LIQUID OPTICS Interface is intended for single patient use only. Full-thickness corneal cuts or incisions should be performed with instruments and supplies on standby, to seal the eye in case of anterior chamber collapse or fluid leakage. Patients who will undergo full-thickness corneal incisions with the CATALYS® System should be given the same standard surgical preparation as used for patients undergoing cataract surgery for the removal of the crystalline lens. During intraocular surgery on patients who have undergone full-thickness corneal incisions with the CATALYS® System, care should be taken if an eyelid speculum is used, in order to limit pressure from the speculum onto the open eye. Patients who will be transported between the creation of a full-thickness corneal incision and the completion of intraocular surgery should have their eye covered with a sterile rigid eye shield, in order to avoid inadvertent eye injury during transport. Patients must be able to lie flat and motionless in a supine position and able to tolerate local or topical anesthesia.
ADVERSE EFFECTS: Complications associated with the CATALYS® System include mild Petechiae and subconjunctival hemorrhage due to vacuum pressure of the LIQUID OPTICS Interface Suction ring. Potential complications and adverse events generally associated with the performance of capsulotomy and lens fragmentation, or creation of a partial-thickness or full-thickness cut or incision of the cornea, include: acute corneal clouding, age-related macular degeneration, amaurosis, anterior and/or posterior capsule tear/rupture, astigmatism, capsulorrhexis notch during phacoemulsification, capsulotomy/lens fragmentation or cut/incision decentration, cells in anterior chamber, choroidal effusion or hemorrhage, conjunctival hyperemia/injection/erythema/chemosis, implant, diplopia, dropped or retained lens, dry eye/superficial punctate keratitis, edema, elevated intraocular pressure, endothelial decompensation, floaters, glaucoma, halo, inflammation, incomplete capsulotomy, intraoperative floppy iris syndrome, iris atrophy/extrusion, light flashes, meibomitis, ocular discomfort (e.g., pain, irritation, scratchiness, itching, foreign body sensation), ocular trauma, petechiae, photophobia, pigment changes/pigment in corneal endothelium/foveal region, pingueculitis, posterior capsule opacification, posterior capsule rupture, posterior vitreous detachment, posteriorly dislocated lens material, pupillary contraction, red blood cells in the anterior chamber (not hyphema), residual cortex, retained lens fragments, retinal detachment or hemorrhage, scar in Descemet’s membrane, shallowing or collapsing of the anterior chamber, scoring of the posterior corneal surface, snail track on endothelium, steroid rebound effect, striae in Descemet’s, subconjunctival hemorrhage, thermal injury to adjacent eye tissues, toxic anterior shock syndrome, vitreous in the anterior chamber, vitreous band or loss, wound dehiscence, wound or incision leak, zonular dehiscence.
CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. The system should be used only by qualified physicians who have extensive knowledge of the use of this device and have been trained and certified.
ATTENTION: Reference the labeling for a complete listing of Indications and Important Safety Information.
INDICATIONS AND IMPORTANT SAFETY INFORMATION FOR THE TECNIS® MULTIFOCAL 1-PIECE AND TECNIS® MULTIFOCAL TORIC II IOLs
Rx Only
INDICATIONS: The TECNIS® Multifocal 1-Piece intraocular lenses are indicated for primary implantation for the visual correction of aphakia in adult patients with and without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire near, intermediate, and distance vision with increased spectacle independence. The TECNIS® Multifocal Toric II lens models ZKU150, ZKU225, ZKU300, ZKU375 and ZLU150, ZLU225, ZLU300, ZLU375 are indicated for primary implantation for the visual correction of aphakia and for reduction of residual refractive astigmatism in adult patients with or without presbyopia, with greater than or equal to 1 diopter of preexisting corneal astigmatism, in whom a cataractous lens has been removed in order to provide near, intermediate and distance vision. The IOLs are intended for capsular bag placement only.
WARNINGS: Physicians considering lens implantation should weight the potential risk/benefit ratio for any conditions described in the Directions for Use that could increase complications or impact patient outcomes. Multifocal IOL implants may be inadvisable in patients where central visual field reduction may not be tolerated, such as macular degeneration, retinal pigment epithelium changes, and glaucoma. The lens should not be placed in the ciliary sulcus. Inform patients about the possibility that a decrease in contrast sensitivity and an increase in visual disturbances may affect their ability to drive a car under certain environmental conditions, such as driving at night or in poor visibility conditions. The clinical study of the TECNIS® Toric 1- Piece IOL did not show evidence of effectiveness for the treatment of preoperative corneal astigmatism of less than one diopter. Rotation of the TECNIS® Multifocal Toric II IOL away from its intended axis can reduce its astigmatic correction. Misalignment greater than 30° may increase postoperative refractive cylinder.
PRECAUTIONS: Prior to surgery, inform prospective patients of the possible risks and benefits associated with the use of this device and provide a copy of the patient information brochure to patient. Secondary glaucoma has been reported occasionally in patients with controlled glaucoma who received TECNIS® Multifocal IOL implants. The long term effects of intraocular lens implantation have not been determined.
Accurate keratometry and biometry in addition to the use of the TECNIS® Toric Calculator (www.TecnisToricCalc.com) are recommended to achieve optimal visual outcomes with TECNIS® Multifocal Toric II IOLs. The safety and effectiveness of the toric intraocular lens have not been substantiated in patients with certain preexisting ocular conditions and intraoperative complications. All preoperative surgical parameters are important when choosing a toric lens for implantation. Variability in any of the preoperative measurements can influence patient outcomes. All corneal incisions were placed temporally in the TECNIS® Toric 1-Piece IOL clinical study. Do not reuse, resterilize, or autoclave.
ADVERSE EVENTS: Only the rate (3.3%) of surgical re-interventions, most of which were non-lens-related, in the ZLB00 (+3.25 D) lens group, was statistically higher than the FDA grid rate (for both first and second eyes). The most frequently reported cumulative adverse event that occurred during the TECNIS® Toric 1-Piece IOL clinical trial was surgical re-intervention, which occurred at a rate of 3.4% (lens repositioning procedures and retinal repair procedures).
ATTENTION: Reference the Directions for Use for a complete listing of Indications and Important Safety Information.
INDICATIONS and IMPORTANT SAFETY INFORMATION for TECNIS Eyhance™ and TECNIS Eyhance™ Toric II IOLs with TECNIS Simplicity® Delivery System
Rx Only
INDICATIONS FOR USE: The TECNIS Simplicity™ Delivery System is used to fold and assist in inserting the TECNIS Eyhance™ IOL for the visual correction of aphakia in adult patients in whom a cataractous lens has been removed by extracapsular cataract extraction. The lens is intended to be placed in the capsular bag. The TECNIS Simplicity® Delivery System is used to fold and assist in inserting the TECNIS Eyhance™ Toric II IOLs for the visual correction of aphakia and pre-existing corneal astigmatism of one diopter or greater in adult patients with or without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire reduction in residual refractive cylinder. The lens is intended to be placed in the capsular bag.
WARNINGS: Physicians considering lens implantation should weigh the potential risk/benefit ratio for any conditions described in the Directions for Use that could increase complications or impact patient outcomes. The lens should be placed entirely in the capsular bag. Do not place the lens in the ciliary sulcus. Do not attempt to disassemble, modify or alter the delivery system or any of its components, as this can significantly affect the function and/or structural integrity of the design. Do not implant the lens if the rod tip does not advance the lens or if it is jammed in the delivery system. The lens and delivery system should be discarded if the lens has been folded within the cartridge for more than 10 minutes.
PRECAUTIONS: This is a single use device, do not resterilize the lens or the delivery system. Do not store the device in direct sunlight or at a temperature under 5°C (41°F) or over 35°C (95°F). Do not autoclave the delivery system. Do not advance the lens unless ready for lens implantation. The contents are sterile unless the package is opened or damaged. The recommended temperature for implanting the lens is at least 17°C (63°F). The use of balanced salt solution (BSS) or viscoelastics is required when using the delivery system. Do not use if the delivery system has been dropped or if any part was inadvertently struck while outside the shipping box.
ADVERSE EVENTS: The most frequently reported cumulative adverse event that occurred during the SENSAR® 1-Piece IOL clinical trial was cystoid macular edema which occurred at a rate of 3.3%.
ATTENTION: Reference the Directions for Use for a complete listing of Indications and Important Safety Information
