Although
glaucoma is the leading cause of irreversible blindness worldwide,
1 we fortunately have many effective therapeutic options to combat the potentially visually devastating effects of the disease. Unfortunately, the same medications that prevent glaucoma from progressing can also take a significant toll on the ocular surface.
2-4In fact, it is estimated that 38.5 to 75% of patients who are being treated for glaucoma also have ocular surface disease (OSD), with
dry eye being more prevalent in patients using topical glaucoma medications than those without glaucoma.
3Therefore, glaucoma treatment can be a cause of OSD for some, while for others, treatment acts as a source of exacerbation for preexisting ocular surface disorders.
The link between OSD and glaucoma
Despite the common occurrence of
OSD in glaucoma patients, especially OSD that is specifically related to glaucoma treatment, it often can go unaddressed. A major reason glaucoma-associated OSD is often overlooked is the necessity of glaucoma treatment to prevent permanent vision loss.
When faced with the choice between blindness and OSD, disruption to the ocular surface is often perceived as unfortunate collateral damage in the effort to prevent irreversible vision loss. However, this view could underestimate not only the impact of OSD as an independent condition, but its impact on glaucoma treatment as well.
“OSD negatively affects patients’ quality of vision and ocular comfort, and these disruptions can be significant.”
OSD and dry eye have been associated with a lower quality of life, as well as anxiety and depression.2,5,6 Patients with OSD will often suffer from poor visual quality due to an unstable tear film and surface disruptions such as punctate epithelial keratitis (PEK). Further, significant irritation and light sensitivity can make it difficult to perform visual tasks, including computer use, walking, or even driving.
The impact of OSD on patient compliance for glaucoma treatment
OSD can have a detrimental effect on adherence to glaucoma treatment itself. Patient compliance is already one of the greatest challenges in managing glaucoma,7 as patients are required to use their glaucoma drops daily, typically for life (barring any surgical intervention), and the vast majority of patients are on multiple medications.8
So, if keeping up with their daily drop routine was not already daunting enough, add in the fact that the drops also might make their eyes irritated every time they use them, and you have a perfect recipe for
non-compliance. This predicament requires a clinical balancing act, were eyecare providers (ECPs) must try to achieve the dual goals of maintaining adequate intraocular pressure (IOP) control to prevent glaucoma progression, while also mitigating secondary damage to the ocular surface caused by glaucoma treatment itself.
This is a particularly challenging scenario, as the solution to one of these challenges often opposes the goal of the other. Therefore, ECPs must be aware of all treatment options—for both glaucoma and OSD—to successfully manage these challenging cases.
Adding insult to injury: glaucoma treatment and OSD
While there are numerous subtypes of glaucoma, such as
primary open angle glaucoma, normal tension glaucoma, and pigmentary glaucoma, each with different underlying causes, the goal of treatment remains the same—which is to lower IOP to a point where the condition can be stabilized and progression is prevented.
9Available glaucoma treatment modalities
There are numerous pharmaceutical and surgical options available to meet the goal of pressure reduction, including topical prostaglandin analogs (PGAs), beta-blockers, alpha-adrenergic agonists, carbonic anhydrase inhibitors (CAIs), rho-kinase inhibitors, and several combination drops.
Surgically, options range from relatively noninvasive laser procedures like
selective laser trabeculoplasty (SLT), to
microinvasive glaucoma surgeries (MIGS) performed alongside cataract surgery or as standalone, to more invasive procedures like trabeculectomy and last-line options like micropulse transscleral cyclophotocoagulation (MP-TSCPC) which are usually reserved for more advanced cases.
10-12Typically, with the exception of SLT, the first-line of treatment for glaucoma is the use of topical hypotensive agents.13 While each topical agent can be used effectively in the management of glaucoma, some pose more challenges to ocular surface health than others.
Regardless of the treatment regimen used, two factors that have the greatest impacts on ocular surface health include:2,3,14
- The number of drops and frequency used.
- Duration of treatment.
A greater number of drops and a longer duration of treatment have both been associated with worsening impacts on the ocular surface.
2,3 Unfortunately, glaucoma is chronic and progressive if left untreated, and patients often require several topical treatments to achieve adequate IOP control, as over 88% of glaucoma patients need to use
two or more medications to manage the disease.
8 Consequently, glaucoma treatment by necessity typically requires the use of multiple drops per day for life, which unfortunately puts the ocular surface at increased risk for significant damage.
The impact of topical glaucoma treatments on the ocular surface
The ocular surface is comprised of the cornea, conjunctiva, tear film, meibomian glands, lacrimal glands, goblet cells, the eyelids, and lashes.
15,16 Each of these constitutive elements must work together to ensure the proper
homeostatic function of the ocular surface.
Unfortunately, the use of topical glaucoma treatments can have a negative impact on nearly every one of these components, as patients using topical glaucoma medications have been shown to have reduced tear production and breakup time,2,3 lower lipid layer thickness,2,3 meibomian gland dysfunction (MGD),2,3 blepharitis,3 PEK and conjunctival staining,2,3 ocular hyperemia,2 decreased corneal sensitivity,2,3 and increased tear osmolarity.2,3
Meibomian gland dysfunction is a common ocular surface finding in glaucoma, with 80% of patients on topical therapy affected by the condition.
17 Topical glaucoma therapies, specifically PGAs, and beta-blockers, have been associated with abnormal gland structure and disrupt meibomian gland epithelial cell homeostasis,
2,3,18,19 resulting in impaired meibum production as evidenced by reduced lipid layer thickness. Topical glaucoma treatments also have a negative impact on the conjunctiva, causing a reduction in goblet cell density and a subsequent decrease in mucin production, which can cause chronic ocular surface inflammation and conjunctival fibrosis.
20 Additionally, the corneal nerves can be damaged by long-term topical hypotensive use, especially the use of beta-blockers.
2-4,21 This nerve disruption causes an attenuation in corneal sensitivity which can impair the trigeminal reflex arcs responsible for blinking and tearing, resulting in a reduced blink rate and tear production.
2,22,23 This reduction in sensitivity can ultimately lead to the spontaneous breakdown of the corneal surface and impaired wound healing, which is characteristic of
neurotrophic keratitis.
24-26The result of these disruptions is an unstable tear film with thinning of the mucus, aqueous, and lipid components.2,3 This instability is shown functionally by the reduced tear break-up time observed in glaucoma patients.2,3
Screening patients for OSD caused by glaucoma medications
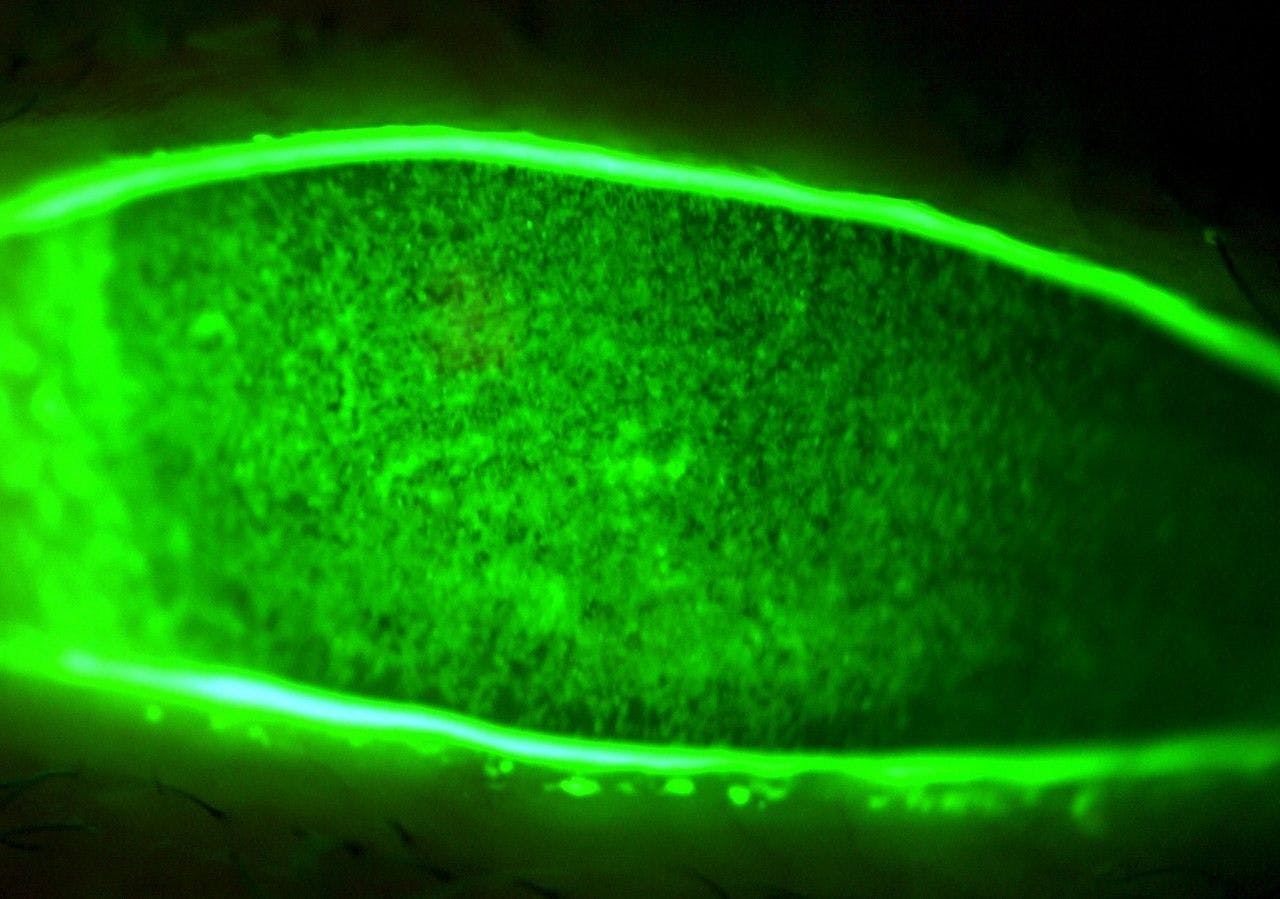
Topical glaucoma medications can also cause damage to the corneal and conjunctival epithelium, as shown by the presence of corneal and conjunctival staining upon instillation of fluorescein dye.2,3 Figure 1 shows an example of such staining, as this patient, who is using three different topical glaucoma medications, displays significant corneal SPK. Preservative-containing glaucoma medications have been shown to impair corneal epithelial barrier function, and even cause cellular necrosis and apoptosis.27,28 The resultant epithelial disruption can range from SPK to significant epithelial defects.29
Additionally, topical drop therapy has also shown to increase the level of inflammatory factors present in the tear film and ocular surface, which can lead to further damage of the cornea, meibomian glands, and other surface structures.
2,3,29,30 Although a longer duration of treatment worsens these effects, it is worth noting that a prolonged period of time is not necessary for these changes to manifest, as inflammation associated with initiation of
glaucoma treatment can occur within 3 months.
31Figure 1 shows corneal and conjunctival staining of a patient on three topical glaucoma medications with significant corneal superficial punctate keratitis.
Figure 1: Courtesy of Cory J. Lappin, OD, MS, FAAO
Understanding the effect of preservatives on the ocular surface
So, how exactly do topical glaucoma medications cause these adverse effects? Much like ocular surface disease itself, the detrimental effects of glaucoma treatment are thought to be multifactorial.2 The primary offender is not the active ingredient of the medication, but rather the preservative, specifically benzalkonium chloride (BAK), which is present alongside the therapeutic agent in most topical formulations.2,3
However, while BAK has the greatest impact, studies have shown that even preservative-free formulations of several glaucoma agents can disrupt the ocular surface, so both appear to play a role in glaucoma-associated OSD.2,3
BAK is a detergent-like substance that disrupts cellular membranes and metabolic function,
30 and is one of the most common preservatives used in topical ophthalmic drops.
3 However, it is notorious for its
toxicity to the ocular surface.
32-34 This potential for toxicity compounds with repeated use, so much of the ocular surface damage related to topical glaucoma therapy is due to chronic exposure to preservatives.
2,3 BAK is proinflammatory and can significantly disrupt the ocular surface.
30 The preservative can alter the tear film and damage the meibomian glands,
17 goblet cells,
35 corneal and conjunctival epithelium,
3,27-29 and corneal nerves (which can result in neurotrophic keratitis
21,32,33).
BAK exposure is associated with worsening dry eye and OSD, and limiting exposure by switching to preservative-free drops has been shown to greatly improve ocular surface health.2,3
The link between glaucoma medications and ocular surface disruption
Although PGAs appear to have a minimal effect on the corneal surface, they are intrinsically proinflammatory and can cause significant conjunctival injection and negatively impact the eyelids and meibomian glands.18,20,36 Additionally, in patients with a history of herpetic keratitis, the use of PGAs carries the risk of inducing reactivation of the infection.4
Of the routinely used ocular hypotensive agents, beta-blockers, specifically timolol, have been shown to have the most detrimental effect on ocular surface health.
2,3,4 The primary reason for this is the impairment of nerve sensation associated with their use, as well as their negative impact on
meibomian gland health.
19,21 By impairing nerve sensation, the reflex arcs responsible for blinking and tear production are blunted, which causes a reduction in tear secretion and a resultant abnormal tear film.
2,22,23“If this decrease in nerve sensitivity becomes too great, neurotrophic keratitis can develop.”
This can result in diminished epithelial cell turnover, impaired corneal wound healing, persistent epithelial defects, ulcers, and even corneal melting and perforation.24-26 Even preservative-free formulations have been shown to have these detrimental effects, although to a lesser extent than their preservative-containing counterpart.37-39
Alpha-adrenergic agonists and CAIs have both been associated with drug-related ectropion, which can lead to corneal exposure and impaired blinking mechanics.4 Additionally, CAIs have also been shown to temporarily destabilize the tear film.40 Rho-kinase inhibitors, while not particularly damaging to the ocular surface, are known to cause significant hyperemia, which can be a major cosmetic concern for some patients.41
Managing glaucoma-associated OSD
So, what is the best way to manage all the potential detrimental effects of topical glaucoma medications, while still effectively
managing a patient’s IOP control? An effective management strategy addresses the major factors behind glaucoma-associated OSD, such as frequent dosing and chronic preservative exposure and toxicity.
2Therefore, it is recommended that glaucoma patients with OSD:
- Use preservative-free formulations.
- Utilize combination drops when possible.
- Consider “dropless” options, such as SLT or MIGS, when appropriate.
- Directly treat concomitant OSD.
1. Using preservative-free formulations
The first step is to use preservative-free formulations, as this eliminates the main driver of glaucoma-associated OSD. Studies of patients who were switched from preservative-containing to preservative-free topical drops noted improvement in discomfort upon drop instillation, ocular irritation, redness, SPK/surface staining, and
blepharitis.
42-44 After switching to preservative-free medication, patients also reported less frequent use of artificial tears.
44Consequently, patient compliance has also been shown to improve when switching to preservative-free drops, likely due to a decrease in the irritating side-effects associated with preservative-containing medications.2,3 However, preservative-free formulations of glaucoma medications are not as common as their preservative-containing counterparts. Additionally, when preservative-free versions are available, they tend to be more costly, so accessing these medications can be a significant obstacle for some patients.
2. Prescribing combination drops
The use of combination drops should be utilized whenever possible to decrease the total drop burden on the ocular surface. In terms of IOP control, it has been shown that the use of two combination drops (dual maximum therapy) was non-inferior in efficacy to two single-drug treatments plus one combination drop (triple maximum therapy).
However, patients using dual maximum therapy had significantly better signs and symptoms of dry eye,45,46 likely due to a reduction in the number of drops instilled daily.
3. “Dropless” treatment options
If a patient is unable to obtain preservative-free therapies, or the use of drops, in general, is irritating, another viable alternative is a “dropless” option, such as SLT.
Selective laser trabeculoplasty is already considered by many to be a first-line treatment for glaucoma given its efficacy and the fact it is not reliant on patient compliance,
13 as the patient will not be required to use any topical medications if adequate IOP control is achieved with the procedure alone. And even if a patient still needs to use a topical therapy after SLT is performed, ideally the number of drops instilled daily would be reduced, which would help improve ocular surface health.
MIGS are another excellent dropless alternative for patients who also have significant cataracts, as these procedures can eliminate or reduce the reliance on topical therapy for IOP control.
47 Furthermore, patients who underwent MIGS procedures demonstrated increased tear break-up times, reduced corneal staining, and reported an improvement in quality of life.
47 Additionally, numerous extended-release glaucoma treatment options are being investigated, such as drug-containing punctal plugs and intraocular implants that may reduce drop burden as well.2 Along these lines, Durysta (bimatoprost intracameral implant 10mcg, Allergan, An AbbVie Company) is commercially available as a preservative-free biodegradable implant that can lower IOP for up to several months.48
4. Treating the concomitant dry eye
It is worth mentioning that if you find yourself managing a patient’s glaucoma care but not their dry eye/OSD or vice versa, then it is critical to be in
communication with the other managing ECP. Both ECPs need to be on the same page to successfully manage each condition, which is much easier if there is clear communication between the treating doctors.
Treating ocular surface disease directly
The other obvious, but sometimes overlooked, element of managing glaucoma-associated OSD is treating the ocular surface directly. While the first treatment suggested by many ECPs for dry eye and OSD is artificial tears, experientially, the last thing most glaucoma patients want is another drop to use, even if it is preservative-free.
Fortunately, there are numerous dropless options for managing dry eye and OSD, including
omega-3 fatty acid supplementation, warm compresses, lid hygiene (hypochlorous acid spray), thermal pulsation procedures, microblepharoexfoliation, and intense pulsed light (IPL). Additionally, Tyrvaya (varenicline solution nasal spray 0.03mg, Viatris) and the iTear100 device (Olympic Ophthalmics) can be used to increase tear production without the use of a drop which can be particularly beneficial for glaucoma patients already using multiple topical medications per day.
If a patient happens to have a significant inflammatory component to their OSD, then the use of an
immunomodulator, such as Xiidra (lifitegrast ophthalmic solution 5%, Novartis), Cequa (cyclosporine ophthalmic solution 0.09%, Sun Pharmaceuticals), or Restasis (cyclosporine ophthalmic emulsion 0.05%, Allergan) can be beneficial.
However, the use of immunomodulators pose two challenges for this patient population:
- It requires twice-a-day dosing, which adds an even greater drop burden.
- The most common side effect of immunomodulators is burning or stinging upon instillation, which can be amplified if the patient’s ocular surface is already irritated from chronic drop use.
Therefore, it may be helpful to utilize strategies to reduce this irritation upon instillation by recommending the use of a preservative-free artificial tear 10 to 15 minutes prior to immunomodulator use to “prep” the surface and/or refrigeration of the drop to provide a cooling sensation upon installation.
Finally, I would be remiss if I did not mention the latest entrant into the ocular surface space called MIEBO (100% perfluorohexyloctane, Bausch + Lomb) indicated for the treatment of the signs and symptoms of dry eye disease.49 This medication looks to directly target tear evaporation to potentially aid in returning homeostatic balance back to the ocular surface.50
The positive impacts of treating OSD on glaucoma management
Treating OSD can also have a positive impact on glaucoma treatment. From a testing perspective, the use of a
preservative-free artificial tear prior to visual field testing has been shown to improve test reliability and decrease testing time, both of which have been shown to be negatively impacted by OSD.
48-50One study even showed an improvement in IOP control in patients with severe OSD who were previously nonresponsive to topical therapy.51 This improvement likely stemmed from increased compliance with therapy as drop use was less irritating, which illustrates the potential benefit of treating OSD in the context of glaucoma management, as the improved ocular surface can more readily tolerate frequent drop instillation which can result in better IOP control.2
Final thoughts on treating glaucoma and OSD
When facing glaucoma-associated OSD, we are met with the predicament of maintaining tight IOP control at the expense of the health of the ocular surface due to the chronic use of preservative-containing, and in some cases, intrinsically irritating IOP-lowering agents.
However, this tradeoff often leads to poor compliance, as patients may not see the tangible value in using these medications as
glaucoma progression is typically slow and painless, whereas the use of therapeutic drops is frequent and irritating. While this can make simultaneously managing a patient’s glaucoma and ocular surface health seem like a daunting, almost Sisyphean task, addressing both elements is necessary to achieve good clinical outcomes and maintain a patient’s quality of life.
Although this can be a challenging undertaking, the use of preservative-free medications, utilizing combination drops whenever possible, electing for dropless IOP management procedures, such as SLT or MIGS, and the direct treatment of OSD can all help successfully achieve the dual goals of keeping glaucoma controlled while
maintaining ocular surface health.