Eyes On Dry Eye 2023 provided eyecare professionals with the latest research and education, live sessions, and interactive Q&As with renowned specialists. Attendees could earn up to 7 hours of free COPE-accredited CE on topics directly related to patient care, including how to get started with a dry eye practice, learning about the most promising treatments in the pipeline, and many more.
Enjoy this presentation from I. Paul Singh, MD, and Justin Schweitzer, OD, FAAO, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
It’s well-known that the medical management of
glaucoma suffers due to patient noncompliance during treatment.
Clinicians can find it very difficult to keep patients happy on multiple medications long-term, and compliance is even harder when it is necessary to treat glaucoma and OSD simultaneously.
Watch the full lecture from Drs. Singh and Schweitzer here!
Sign up for our newsletter to watch the full recording and to register for more Eyes On events.
Redefining controlled glaucoma
The definition of controlled glaucoma has changed over the years. Previously, the focus of glaucoma treatment was limited to watching a patient’s intraocular pressure (IOP),
visual field, and optical coherence tomography (OCT) retinal nerve fiber layer (RNFL). Now, controlled glaucoma also factors in looking at the patient’s tolerability to treatment and the likelihood that they will stay on their therapy long-term.
The impact of glaucoma medications on the ocular surface
Glaucoma therapy can impact the ocular surface in many ways, including the
meibomian glands. It can be helpful to conceptualize glaucoma treatment as a marathon, and as the eyecare practitioner (ECP), the goal is to piece together different medications/treatments throughout the course of the marathon to slow disease progression.
A
study looking at the effects of glaucoma medications on the ocular surface found that patients on multiple medications with preservatives had increased meibomian gland dysfunction (MGD) due to reduced meibomian glands and acinar density.
A separate
study conducted in 2008 looked at 101 patients with glaucoma and/or ocular hypertension (OHTN) who used glaucoma medications preserved with benzalkonium chloride (BAK). Researchers found that 59% of patients had symptoms of OSD.
The rate of OSD symptoms increased with the number of BAK-containing drops:
- 1 BAK drop: ~52% of patients with symptoms
- 2 BAK drops: ~62% of patients with symptoms
- 3 BAK drops: ~68% of patients with symptoms
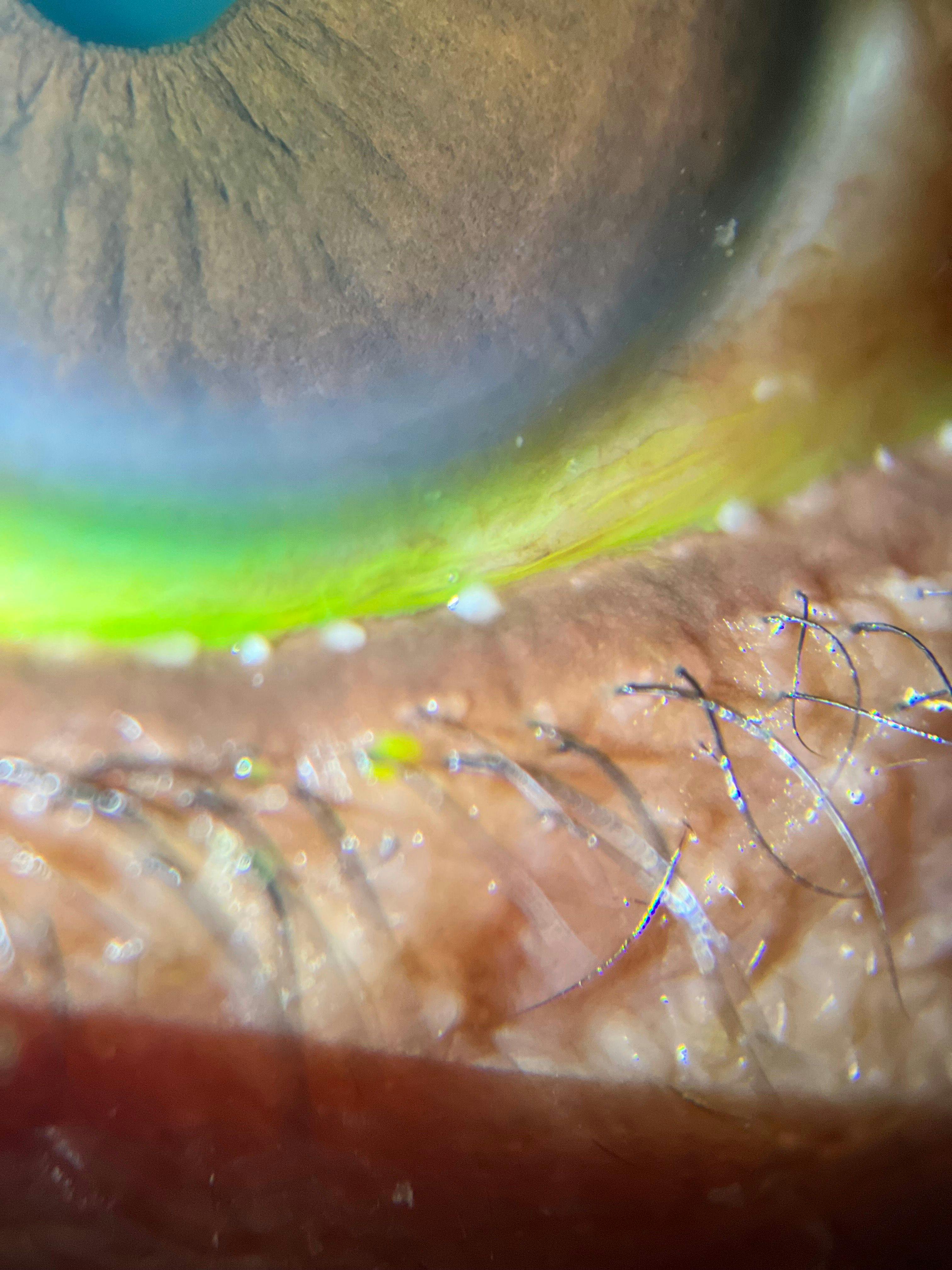
Figure 1 highlights a patient with meibomian gland dysfunction caused by the use of glaucoma medications with preservatives.
Dry eye disease and glaucoma medication compliance
Dry eye disease (DED) is a common reason for the discontinuation or inadequate adherence/compliance to glaucoma treatment. A
study from Christophe Baudouin showed that there is a 30% reduction in patient compliance if there is concomitant OSD.
The ultimate goal of glaucoma treatment is to stabilize and lower IOP and data shows that fluctuating IOP increases the risk of glaucoma progression. So a patient with concomitant OSD is even less likely to be taking their glaucoma medications every day due to their symptoms, meaning, in turn, that their IOP is fluctuating even more.
Furthermore, in a
study by Stringham et al. with 74 glaucoma patients, DED symptoms were a predictor of noncompliance. Patients without DED symptoms had an 89% compliance rate with glaucoma medications, while patients with DED symptoms had a 63% compliance rate.
Solutions for treating glaucoma and concomitant OSD
BAK- and preservative-free glaucoma medications
BAK- and preservative-free formulations of
glaucoma medications offer ECPs an avenue for treating glaucoma while minimizing the effects on the ocular surface.
Drs. Singh and Schweitzer noted that they both prefer to offer patients glaucoma medications with preservatives and then switch to a preservative- or BAK-free formulation, depending on how patients respond.
Selective laser trabeculoplasty to treat glaucoma
Another option available to ECPs is a
selective laser trabeculoplasty (SLT), which targets pigmented trabecular meshwork (TM) cells. SLTs provide a physiologic approach to treating glaucoma, as the TM is the primary source of resistance in about 50% of patients with primary open-angle glaucoma (POAG).
By using a Q-switched YAG laser, there is little tissue destruction from the procedure, leaving behind healthy tissues. This process rejuvenates the natural drain to help the fluid move around by improving aqueous outflow and regenerating the trabecular meshwork.
Another perk of this procedure is that it can be repeated because it is non-destructive, meaning it doesn’t limit the potential for future procedures, such as a
minimally invasive glaucoma surgery (MIGS) that involves the conventional pathway as well.
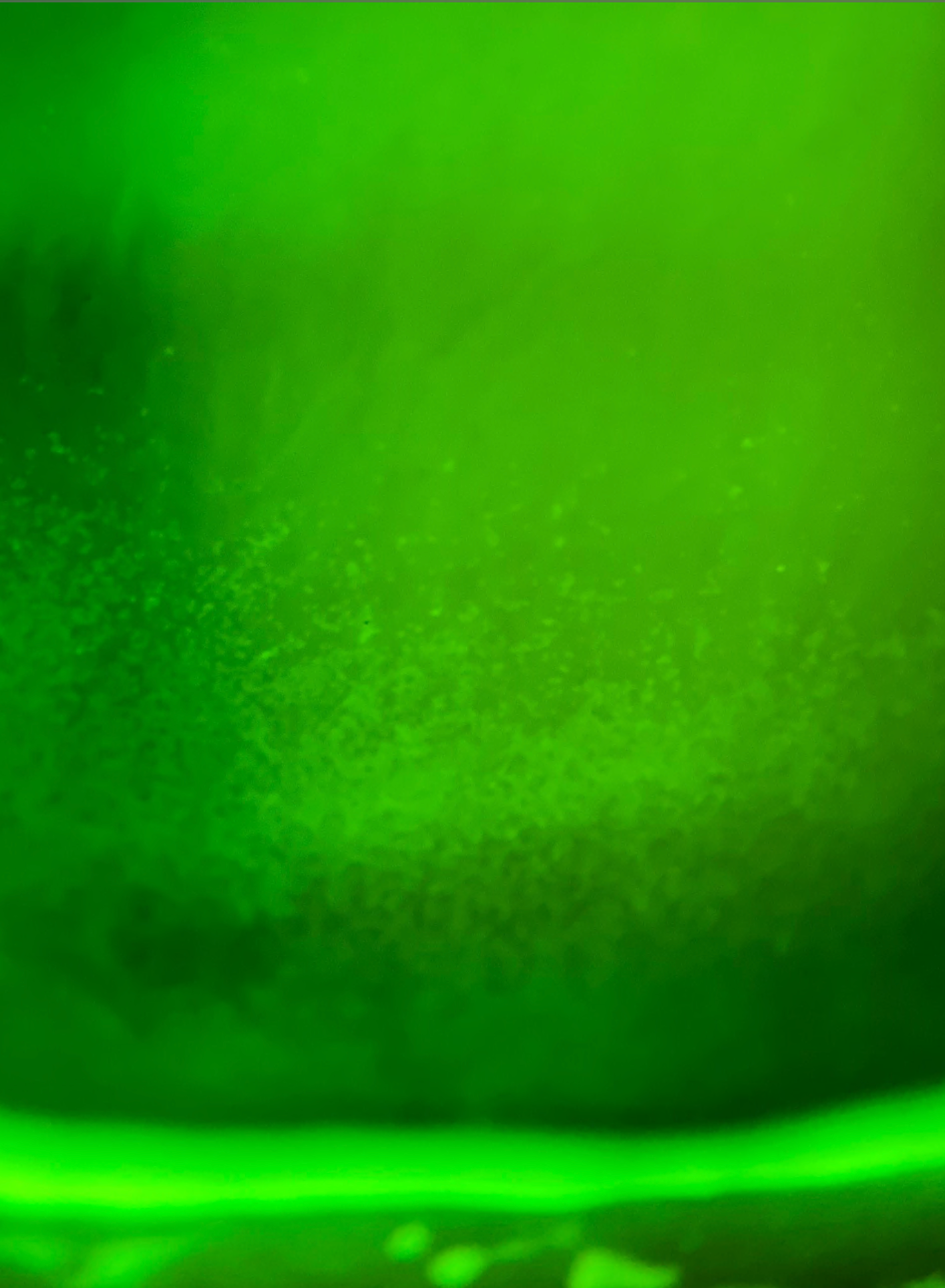
Figures 2 and 3 highlight the ocular surface of a patient from Dr. Singh prior to and 6 weeks after an SLT procedure, respectively. The patient discontinued the use of a prostaglandin drop following the SLT, which also accounts for a clearer ocular surface.
Figure 2: Courtesy of I. Paul Singh, MD
Figure 3: Courtesy of I. Paul Singh, MD
Developments in glaucoma drug delivery systems
A treatment that both Drs. Singh and Schweitzer recommend for glaucoma patients is Bimatoprost SR (Allergan), which is a biodegradable 10 microgram bimatoprost sustained-release implant. It is FDA-approved and indicated to reduce IOP in patients with
open-angle glaucoma or OHT.
The implant requires a single intracameral administration. Using the implant provides ECPs the opportunity to offer patients a “drop holiday” from their usual glaucoma medications while still treating the symptoms of ocular surface disease plus continuing to control IOP
Clinical trials on the bimatoprost SR implant
While some may be concerned about the FDA’s limited approval for the single administration of the bimatoprost implant, recent clinical trials have shown the long-lasting efficacy of the implant. A 24-month
Phase I/II clinical trial showed that patients who received a 10μg bimatoprost implant didn’t require rescue or retreatment for a period of time longer than 4 months.
The results of the Phase I/II clinical trial included the following:
- 68% of patients didn’t need retreatment for 6 months
- 40% of patients didn’t need retreatment for 12 months
- 28% of patients didn’t need retreatment for 24 months
Researchers believe that the implant works by changing the release of metalloproteinases (MMPs). Metalloproteinases release macrophages and cytokines to open up the trabecular meshwork, similar to an SLT. Over time, the 24-hour release of medication remodels the ciliary body and the TM, making this approach to treating glaucoma so exciting.
Ocular surface disease and MIGS procedures
Across multiple studies, MIGS devices like the Hydrus, iStent inject, and the Omni have been proven to reduce patient medication burden.
- The HORIZON study showed that the Hydrus provided, on average, an 82.4% medication reduction from 1.7 to 0.3 medications.
- The iStent inject provided a 75% medication reduction from 1.6 to 0.4 medications.
- The Omni provided a 35% medication reduction from 1.7 to 1.1 medications.
Dr. Singh explained that as a practitioner, his threshold for choosing to discuss MIGS with patients has been lowered because the procedures can help with addressing OSD symptoms. Part of considering the success of a MIGS procedure is not only factoring in the IOP reduction but also the
medication burden reduction as well, which impacts the overall improvement of the patient’s quality of life.
Clinical research by the authors on MIGS procedures and OSD
A
pilot study led by Dr. Schweitzer looked at 47 patients that underwent a combined cataract surgery and MIGS procedure and looked at the 3-month results with OSDI scores following the procedures. The study showed that the mean OSDI severity was reduced from severe (40.1) to mild (17.4), there was a more than three-fold decrease in corneal staining, and a 35% longer tear breakup time (TBUT) between pre- and postoperative.
Dr. Singh was involved in a
Phase III clinical trial of the iStent inject, comparing patients who underwent just cataract surgery to those who had cataract surgery with an additional MIGS procedure to evaluate the improvements in patient outcomes.
Study participants filled out a VFQ-25 survey during the study, and based on the survey, 58% in the iStent inject group showed meaningful improvement vs. 45.8% in the cataract surgery group, yielding a 12.12% point differential between the groups at 24 months.
More glaucoma and OSD treatments to consider
Oral doxycycline to lower IOP
Recently, a
study was presented at the American Academy of Optometry by a group of doctors from the Illinois College of Optometry who put patients on oral doxycycline as an adjunctive therapy to lower IOP. Study participants were prescribed 50mg of oral doxycycline for 90 days on top of glaucoma medications.
Investigators followed up with participants at 30, 90, and 180 days to check their eye pressure. With just the addition of oral doxycycline at 30 days, there was an 8% reduction in the baseline pressure, and the mean IOP was 16mmHg. At 90 days, there was a 15% reduction in IOP, and at 6 months after discontinuing doxycycline, IOP was 4.83% lower than baseline.
Dr. Singh noted that these results likely occur because OSD causes inflammation in the eye, which can cause trabeculitis. Using doxycycline supports a better lipid layer on the eye and helps decrease this inflammation.
Further approaches ECPs can use to identify and treat OSD in glaucoma patients:
- Nutraceuticals for glaucoma patients include gamma-linolenic acid (GLA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA).
- Using SPEED questionnaires, a slit lamp examination, fluorescein dyes, a Wratten filter, and your finger or thumb to evaluate the meibomian glands.
- Remember the “look-lift-pull-push” technique to evaluate meibomian glands and then ask the patient to look down to check the lash margin for Demodex mites.
- In-office therapies for treating OSD include thermal pulsation treatments, applying heat with specific devices that warm the glands, and manually expressing the meibomian glands.
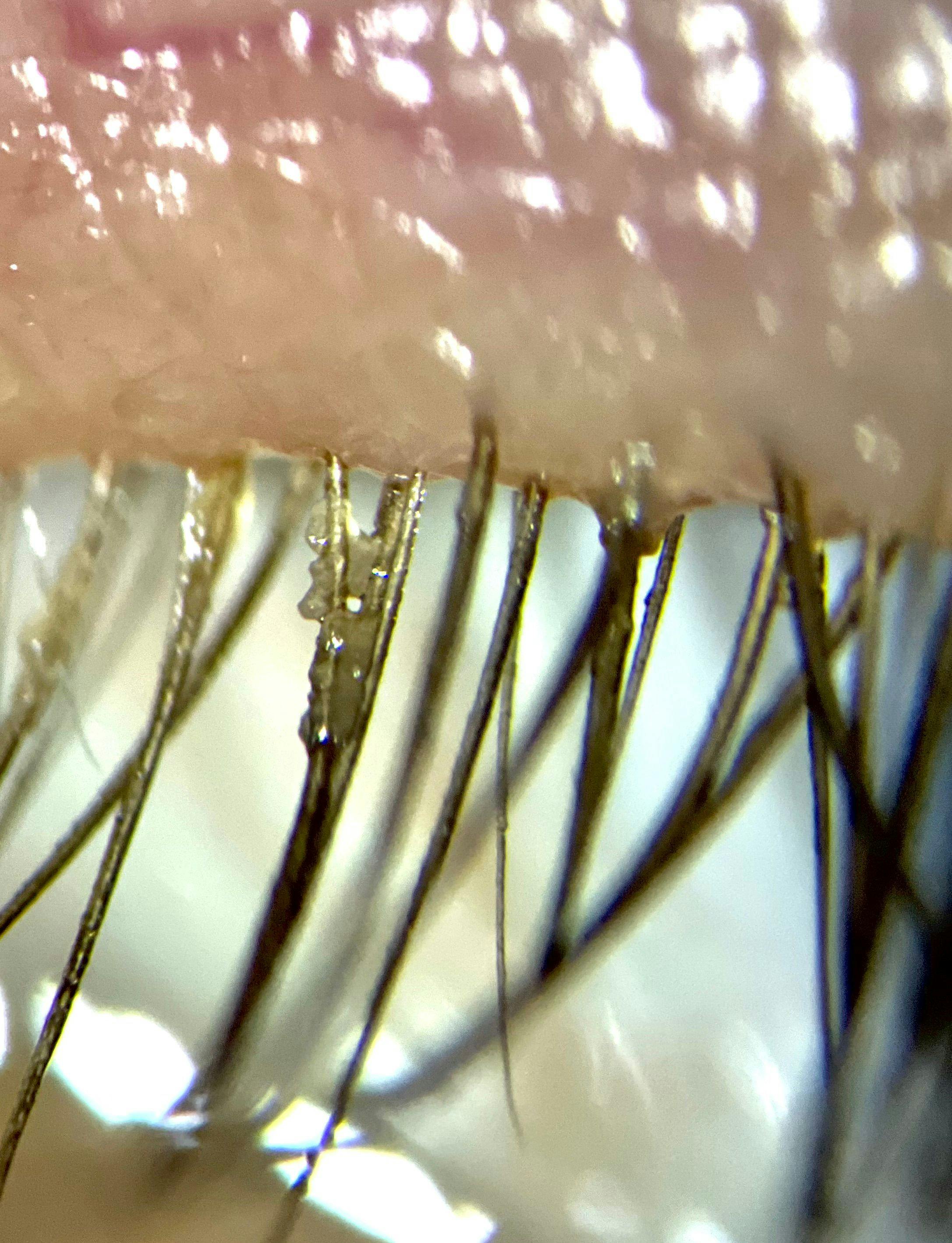
Figure 4: Courtesy of I. Paul Singh, MD
Conclusion
Ocular surface disease is present in many patient populations, but there is an undeniable connection between glaucoma and an increased risk of OSD. When treating glaucoma patients,
ocular surface issues can play a major part in decreased quality of life due to dry eye symptoms.
For eyecare practitioners treating glaucoma patients, it is critical to factor in treating the ocular surface while simultaneously addressing the patient’s
glaucoma symptoms.