From November 18 to 20, 2022, eyecare practitioners from around the world gathered online for Eyes On 2023, a 3 day educational summit offering up to 9 hours of COPE-accredited CE and CME providing the latest innovations in the ophthalmic industry.
Enjoy this presentation from Jeremy M. Cotliar, MD, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
Glaucoma is a disease of progressive optic neuropathy with loss of the nerve fiber layer. As glaucoma develops, the patient slowly loses peripheral vision, and blindness can occur if left untreated. Nearly three million Americans suffer from glaucoma.
High intraocular pressure (IOP) is the strongest known risk factor for glaucoma. Some of the other risk factors for glaucoma include a cup-to-disc ratio greater than 0.5, suspicious retinal nerve fiber layer, a disc hemorrhage, a family history of glaucoma, advanced age, or hyperopia.
How to evaluate a patient for glaucoma
There are five major components to a comprehensive eye exam that are relevant to assessing glaucoma: the slit lamp examination, IOP, gonioscopy, optic nerve evaluation, visual field testing, and pachymetry. Different types of glaucoma will present themselves very differently during a slit lamp exam.
Primary open angle glaucoma (POAG), also referred to as chronic simple glaucoma, is typically bilateral and characterized by adult onset, increased IOP, optic disc cupping, and visual field loss. When performing a gonioscopy on a patient with POAG, the ciliary body band and the adjacent scleral spur indicate an open angle.
Closed-angle glaucoma, however, presents with a red, painful eye. Often the patient will experience nausea, vomiting, photophobia, halos, and rapidly progressive vision impairment. A narrow-angle gonioscopy will present overlapping portions of the ciliary body with less or no definition between them.
We measure IOP a few different ways, the iCare tonometer and Goldmann tonometry being the most common. Although both are considered accurate, Goldmann remains the most trusted and accurate in measuring IOP.
Evaluating the optic disc
When evaluating the optic disc in a non-glaucomatous eye, the inferior segment should be larger than the superior, which should be larger than the nasal segment, which, in turn, should be larger than the temporal segment. This is referred to as the “ISNT rule” (inferior, superior, nasal, temporal), and though there are exceptions, it is a good acronym to remember when evaluating the optic disc.
In a non-glaucomatous eye, the cup-to-disc ratio should be less than 0.35, with sharp margins and healthy appearing vessels. An eye with glaucoma will have a larger cup-to-disc ratio, with blurred margins, and will often be elongated at the superior and inferior poles due to nerve fiber loss.
Assessing the optic nerve with OCT
We also use
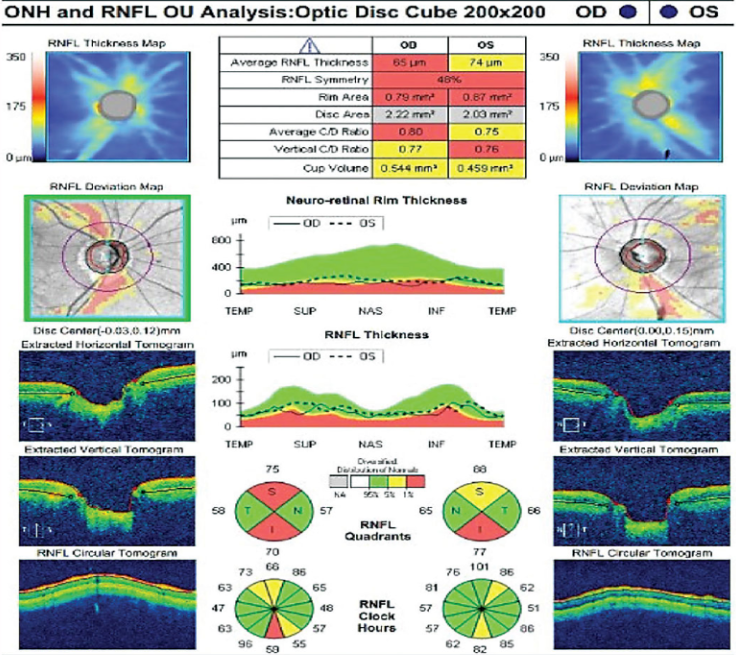
optical coherence tomography (OCT) when evaluating the optic disc. The OCT uses non-invasive light to take a cross-section image of the optic disc and measures the nerve fiber layer. When we’re evaluating an OCT, we like to see lots of green in the normative data section, and in the topography segment of the analysis, we want to see the red “fire” coming out of the optic nerve, indicating a robust nerve fiber layer.
In a glaucomatous OCT (shown below), the quadrants will often appear red, the topographical map will be bluer, and the “fire” of the healthy optic nerve is pretty much extinguished.
Figure 1 is an OCT analysis of the optic nerve and retinal nerve fiber layer of the eye of a glaucoma patient.
Figure 1: Image courtesy of Jeremy M. Cotliar, MD
Pachymetry
Pachymetry measures
central corneal thickness. Normal corneal thickness is between 540 and 560 microns. The thinner the cornea, the greater chance of progression of glaucoma. The corneal thickness impacts our measurements, as thinner corneas will measure lower IOP, and thicker corneas will measure higher. Pachymetry allows us to correct corneal thickness when determining a patient’s true IOP.
Table 1 compares the central corneal thickness to corresponding correction values.
| Central corneal thickness (μm) | Correction value (mmHg) |
|---|
| 410 | 10 |
| 415 | 10 |
| 420 | 9 |
| 425 | 9 |
| 430 | 8 |
| 435 | 8 |
| 440 | 7 |
| 445 | 7 |
| 455 | 6 |
| 465 | 6 |
| 475 | 5 |
| 485 | 4 |
| 495 | 4 |
| 505 | 3 |
| 515 | 2 |
| 525 | 1 |
| 535 | 1 |
| 545 | 0 |
| 555 | -1 |
| 565 | -1 |
| 575 | -2 |
| 585 | -3 |
| 595 | -4 |
| 605 | -4 |
| 615 | -5 |
| 625 | -6 |
| 635 | -6 |
| 645 | -7 |
Table 1: Image courtesy of Jeremy M. Cotliar, MD
Stages of glaucoma
The American Academy of Ophthalmology grades glaucoma in three stages: mild, moderate, and severe. In mild glaucoma, the optic nerve appearance is consistent with glaucoma, but there is no visual field loss. The
visual field of a patient with mild glaucoma will not look any different than a non-glaucoma patient’s visual field.
It takes a loss of at least 50% of the axons, or nerve fiber, to start to see visual field abnormalities. In moderate glaucoma, the optic nerve appears consistent with glaucoma, and we start to see visual field abnormalities. Finally, in severe glaucoma, the visual field loss is advanced, often being seen in more than one hemifield. The visual field loss may completely cover one hemifield, or in the case of severe end-stage glaucoma, the patient may be left with only a small island of vision.
4 options for glaucoma therapy
There are four main ways of treating glaucoma: eye drops, laser, microinvasive glaucoma surgery (MIGS), and incisional surgery.
Eye drops used to treat glaucoma
First, let’s go over
glaucoma eye drops: I tell my patients using monotherapy drops to look at the color of the top when identifying drops because drops in the same class will have the same color top. For example, prostaglandins have turquoise tops and are typically administered at bedtime, yellow tops are beta-blockers, and dark green tops are miotics.
The next stage in drop therapy is combination drops, where two medications, such as dorzolamide and timolol, are administered in the same bottle. These combination drops do not follow the same bottle-top color rule for monotherapy drops.
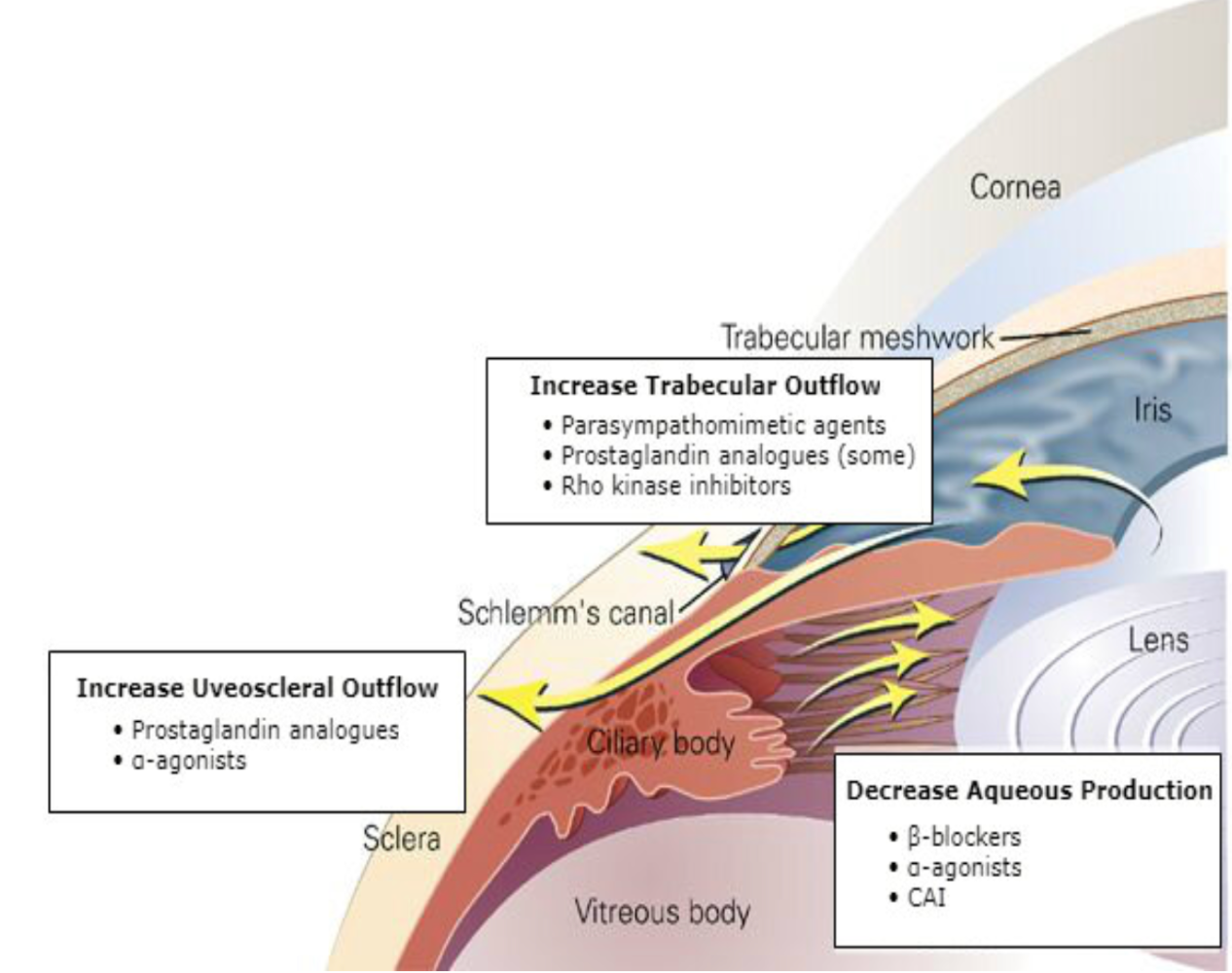
Figure 2 is a cheat sheet for the mechanism of action of the main drops used for glaucoma treatment.
Figure 2: Image courtesy of Jeremy M. Cotliar, MD
Laser therapy for glaucoma
Selective laser trabeculoplasty (SLT) is increasingly being used as a first-line therapy to lower IOP by glaucoma specialists. SLT uses short pulses of low-energy light to target pigment in a glaucomatous eye. In response, the natural healing mechanisms of the body then rebuild these cells. The rebuilt cells result in improved drainage and lower IOP. When used as first-line therapy, it can lower the IOP by 30%, which is the equivalent of a monotherapy eyedrop.
Micro invasive glaucoma surgeries
The benefits of
MIGS are that these surgeries are safer and often less painful than more invasive incisional surgery and can be performed earlier in the progression of glaucoma, hopefully preventing advanced glaucoma.
Some can be performed as stand-alone procedures, and others must be used in conjunction with cataract surgery. There are many different types of
MIGS; the OMNI from Sightsciences, the Kahook dual-blade goniotomy, the iStent, the Hydrus, and the XEN gel stent, which all provide mild to moderate reduction of IOP.
Incisional surgery to treat glaucoma
Endoscopic cyclophotocoagulation (ECP) is a technically challenging procedure in which you ablate the posterior ciliary processes. It can damage the eye and has mixed results in lowering IOP since the aqueous fluid is not produced in the posterior ciliary body.
Durysta is the first, and currently the only, FDA-approved dissolvable ocular implant proven to reduce IOP for 15 weeks.
The major drawback of Durysta is the FDA only approved it for one injection per eye per lifetime, so it can really only be used as a vacation from drops.
In many cases, patients will still opt for the vacation from drops due to the heavy load of preservatives that drops carry, which can cause chronic irritation. In my personal practice, I’ve seen Durysta work effectively for anywhere between 1 month and 1 year. It varies greatly from patient to patient.
What’s coming in the pipeline for 2023 and beyond
There are several new drops in the pipeline. One example of the new drops we will see is Monoprost, a preservative-free latanoprost agent, which shows long-lasting IOP reduction with significantly less redness and irritation for the patient. CKPL-1 is a drop that is not yet being tested on humans but uses an entirely new mechanism of action and is very exciting because early studies show this new drop could lower pressure as much as
invasive glaucoma procedures.
Lastly, although not a glaucoma drop, GS010 is an intravitreal injection that could be the start of
gene- and cell-based therapies for diseases like glaucoma. If we could find ways to regenerate optic nerve tissue, that would be a major development in glaucoma treatment and prevention of vision loss.
Two surgical technologies currently in the pipeline that I am excited about are the iDose and the Sion. The iDose is in stage III of clinical trials and is essentially a combination of the iStent and Durysta. It’s shown promising results in sustained IOP reduction. The Sion from Sightsciences is a bladeless device that removes trabecular meshwork and can be used as a standalone procedure or along with cataract surgery.
Conclusion
These are just a few of the many new technologies we have to look forward to in the world of glaucoma in 2023 and beyond.