For eyecare practitioners (ECPs), both optometrists and ophthalmologists,
managing glaucoma patients start with the important step of disease detection.
Disease detection for glaucoma patients
In 2023, practitioners have a surfeit of diagnostic technologies in glaucoma, but I distill it down to eight pieces that heavily factor into the decision, “Is this glaucoma?”
Eight factors to use to determine if a patient has glaucoma include:
- Age
- Intraocular pressure (IOP)
- Family history
- Corneal pachymetry
- Corneal hysteresis (CH)
- Optic nerve cupping
- Retinal nerve fiber layer (RNFL)/ganglion cell analysis (GCC) measurements on optical coherence tomography (OCT)
- Visual field (VF)
The support for five of eight comes from the initial
OHTS (Ocular Hypertension Treatment Study) trial, with the three outside of OHTS being family history, OCT, and CH.
1 A 2015 study in the American Journal of Ophthalmology showed a first-degree family member (mom, dad, brother, sister, son, or daughter) with glaucoma increases a patient's glaucoma risk 9-fold.
2This is important as new in-office
genetic tests have come onto the scene. Optical coherence tomography (OCT) seems like a now obvious must-have in glaucoma diagnosis and tends to detect early glaucomatous changes with support evident from a meta-analysis of OCT’s predictive accuracy in over 16,000 eyes showed a nearly 0.9 predictive accuracy for areas under the curve.
3 Finally, CH is a measurement of corneal biomechanics, simply defined as the cornea’s ability to absorb shock or changes in pressure.
Studies continue to mount that show CH is supportive in making the glaucoma diagnosis, but equally importantly, CH can be a powerful predictor of glaucoma progression.4,5
Treatment protocols for glaucoma patients
After diagnosing glaucoma, ECPs need to establish a treatment plan which includes treatment modality and a follow-up schedule. The treatment plan will revolve around lowering IOP, and I advocate for setting a target pressure range. This gives patients an expectation or expected path.
The American Academy of Ophthalmology's preferred practice guidelines recommends an initial goal of reducing IOP 20 to 30% below the unmedicated baseline in
primary open-angle glaucoma (POAG).
6 Some practitioners alter this in POAG patients based on disease severity (mild, moderate, severe), and this goal is modified in low-tension glaucoma.
6Similar to the treatment goal, the glaucoma follow-up schedule can be highly dictated by disease severity. Initially, making sure the IOP management is successful 4 to 6 weeks after initiation of therapy is a good start. Long-term, in mild-moderate POAG, planning for two to three visits per year with one to two visual fields (VFs) per year is reasonable, and in moderate-severe disease, relying on four or more visits with at least three VFs in the first year can be a cookbook schedule.
Measuring visual field loss in glaucoma patients
With both treatment goal setting and follow-up schedules hinging heavily on disease severity, defining severity is important. Second, billing and coding set forth with
ICD-10 codes require practitioners to specify glaucoma disease severity. Visual field loss is a very common method of staging glaucoma severity, and we’ll cover two of the most common grading systems.
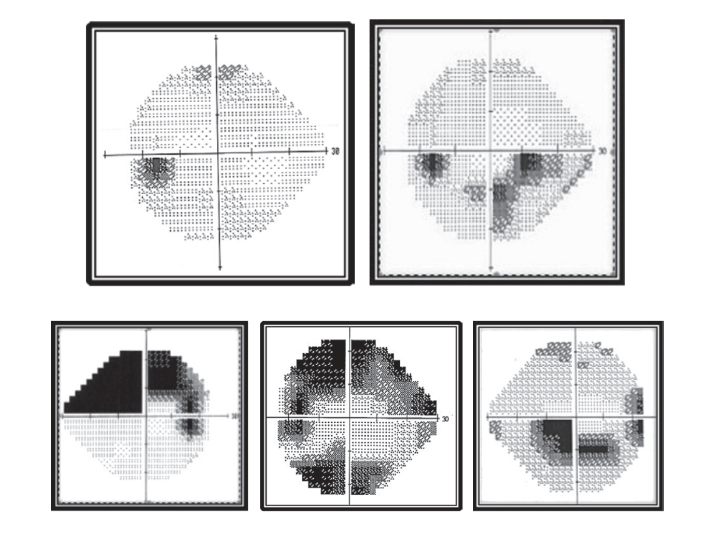
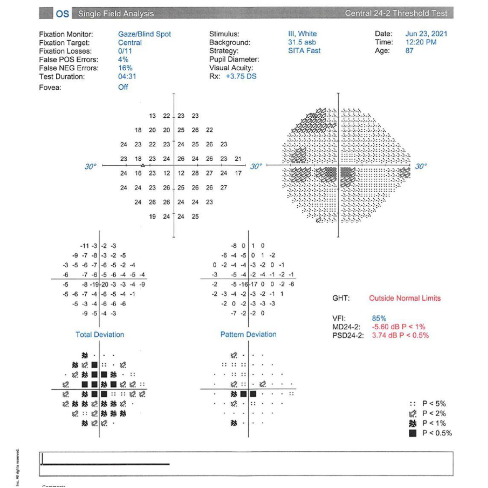
First, the American Glaucoma Society (AGS) and AAO preferred practice guidelines build the severity grade primarily on the premise that if one or two hemifields are affected and if the patient’s central 5 degrees of VF is compromised (See Figure 1 below).8
Figure 1 highlights various visual fields based on glaucoma severity. Top left: mild or early-stage glaucoma. Top right: moderate stage glaucoma. Bottom row: advanced, late, and severe stage glaucoma.
A second VF grading criteria is Hoddap-Parrish-Anderson which focuses on mean deviation (MD) and also the number of points below a certain threshold.9 A hybrid formula is VF mean deviation of 0 to -6db (mild glaucoma), -6db to -12db (moderate glaucoma), and > -12db (severe glaucoma).
Treating glaucoma patients with MIGS
From our therapeutic and surgical perspectives, the last 10 years have brought an impressive broadening in the glaucoma treatment armamentarium with now four IOP treatment pillars, including topical drops, drug delivery of pharmaceuticals, laser trabeculoplasty, and intraocular surgeries.
Zeroing in on glaucoma surgery, this is where
minimally invasive glaucoma surgeries (MIGS) fit in, but it is hardly comparable to previous incisional/filtration glaucoma surgeries. MIGS spotlight minimally traumatic surgeries that excel in safety but still provide at least modest efficacy. Because MIGS prioritize safety and tolerability, practitioners have taken a more interventional glaucoma approach and placed these surgeries earlier in the treatment paradigm.
MIGS procedures can be performed on a wide variety of patients, from mild to end-stage glaucoma, and could be done in combination with cataract surgery or as stand-alone procedures.
Patient selection for MIGS procedures
In our practices, three frequent scenarios that lead to recommending conversion to MIGS surgeries are: hardships with medical therapy, glaucoma progression noted clinically and in imaging studies despite the use of other therapeutics, and finally, a concomitant visually significant cataract.
The first scenario can be rather common, where patients have adversities with topical therapies ranging from stinging/burning to redness to allergic reactions. Maximal medical therapy should be individualized because patient dissatisfaction leads to
non-compliance, a well-documented issue in glaucoma.
10The second challenge is glaucoma progression (VF, OCT, Drance hemorrhage, etc.) which can necessitate introducing surgical treatments and referring for MIGS. Lastly, and arguably the most obvious case presentation to propose utilizing MIGS therapies is the patient with a visually significant cataract with the planned surgery. This is a time-stamp in that patient's life to improve vision but also treat their glaucoma.
Preparing referral letters for MIGS procedures
Referring a patient for MIGS hopefully draws upon a pre-built trusting relationship between an OD-MD or MD-MD. From my (Mitch Ibach, OD, FAAO) point of view as a referring doctor, having a network of surgical partners who are both proficiently skilled in MIGS procedures as well as excited to offer these treatments is step one. Step two is preparing a thorough referral letter.
Over-communication is encouraged with critical data and historical information, such as IOP max, IOP history, previous topical medications plus adverse reactions, and surgical history. If the referring provider has previous ancillary testing like VFs, CH, gonioscopy measurements, and/or OCTs, share these too.
At a minimum, in the referral letter, make sure it is clear your recommendation or opinion is to consider the patient a candidate for a MIGS procedure. As confidence grows in the referring provider, they may start to make a more targeted referral (i.e., trabecular micro-bypass stent vs. canaloplasty vs. subconjunctival procedure).
The final step is to communicate post-operative care expectations. If the referring provider is comfortable and wants to be involved in post-operative care, make this known in the referral letter/record to help facilitate open dialogue.
Choosing the right MIGS procedure
Once a patient has entered the surgical practice, a myriad of MIGS options exist, and the procedure can be tailored to each patient’s needs. In general, surgeons will use the least invasive or those with the highest safety profile in the milder cases and will take more risk with the potential to combine various
MIGS procedures in the more advanced cases.
11Summary of each MIGS procedure based on the target intervention area:
- Trabecular meshwork/Schlemm's canal
- Stents: iStent, iStent Inject, Hydrus, iStent Infinite
- Ablation: KDB GLIDE, Trabectome, TrabEx
- Dilation: Ab-interno canaloplasty (ABiC), iPrime, STREAMLINE, OMNI (combo)
- Suprachoroidal/supraciliary
- Subconjunctival
- Cyclophotocoagulation
- Endoscopic and transscleral: ECP, G6/MP3
Note: xx denotes that the device is not commercially available.
Trabecular Meshwork (TM)
- Trabecular Micro-Bypass Stent: This procedure involves the implantation of a small device(s) that bypasses the trabecular meshwork. These procedures are indicated to be performed at the time of cataract surgery.
- iStent (Glaukos): A single trabecular meshwork stent.
- iStent inject W (Glaukos): Two trabecular meshwork stents placed a few clock hours apart.
- Hydrus Microstent (Alcon): A single trabecular meshwork stent that covers 3 clock hours of the trabecular meshwork.
- Trabecular Micro-Bypass Stent stand-alone: Implantation micro-bypass stents without concurrent cataract surgery.
- iStent Infinite (Glaukos): Three trabecular meshwork stents placed a few clock hours apart.
- Canaloplasty: This procedure involves the use of a small catheter to insert a flexible polymer into the Schlemm’s canal, which helps to increase the outflow of fluid, reducing IOP. These procedures can be performed at the time of cataract surgery or as standalone procedures.
- STREAMLINE Surgical System (New World Medical): This device creates a micro-goniotomy in the TM and then delivers viscoelastic into Schlemm’s canal to dilate the canal and collector channels. Surgeons can create multiple goniotomies over a range of clock hours.
- OMNI Surgical System (Sight Sciences): This device creates a small goniotomy to introduce a catheter into Schlemm’s canal and then releases viscoelastic to dilate the canal and connector channels. The catheter can also be used to perform a trabeculotomy. Both the canaloplasty and trabeculotomy are titratable.
- iTrack microcatheter system (Nova Eye Medical): A surgical device to deliver viscoelastic into Schlemm’s canal to dilate the distal outflow pathway.
- Goniotomy: These procedures incise and partially remove trabecular meshwork to create an opening into Schlemm’s canal.
- KDB GLIDE (New World Medical): This next-generation device (original Kahook Dual Blade) utilizes enhanced dual blades with a rounded heel, tapered sides, and a smaller footplate to incise and remove the TM.
- TrabEx (MST): This device also has two blades to incise and remove the TM.
- SION Surgical Instrument (Sight Sciences): This device is a bladeless instrument used to access the TM and excise the tissue.
Subconjunctival Space
- Xen Gel Stent (Allergan): This procedure involves the implantation of a small device into the anterior chamber, which drains fluid into the subconjunctival space. This procedure can be performed at the time of cataract surgery or as a standalone procedure and is indicated for refractory glaucoma.
- VisiPlate (Avisi Technologies): This technology in development is meant as an alternative to trabeculectomy that is designed to create a low-profile subconjunctival bleb.
Suprachoroidal Space
- No devices are currently available. The CyPass (Alcon) device was recently removed from the market in 2018, and a biotissue stent (Allopass, Iantrek) is currently in development.
Inflow procedures
These procedures treat the inflow system and reduce the production of aqueous to help lower the IOP.
- Endocyclophotocoagulation (ECP) (BVI): This procedure uses laser endoscopy to treat the ciliary processes, slowing the production of aqueous, and as a result, can lower the IOP. This procedure can be performed at the time of cataract surgery or as a standalone procedure.
Post-operative management for MIGS procedures
The post-operative care for
MIGS procedures will vary depending on the specific procedure that was performed. However, there are a few general guidelines that apply to most MIGS procedures.
Following up with patients after the MIGS procedure
Most MIGS patients are seen 1 day, 1 week, and 1 month following the procedure. Based on the severity of glaucoma, patients are then seen on a routine basis that varies from 3 months to 6 months. Below is an outline of what to look out for at the various visits.
Post-Op Day 0
Patients can have fluctuations in their vision and a small amount of irritation from the procedure itself. Blood reflux from the procedure can also cause visual haze. The IOP is variable at this time point.
Post-Op Day 1
Visual acuity is dependent on glaucoma and lens status. In general, vision is slightly worse than it was pre-op due to some mild corneal edema and any residual red blood cells that can be lingering. Occasionally there will be a microhyphema. This is normal from reflux bleeding and will usually clear on its own but can make the vision a bit hazy while it resolves.
Additionally, IOP is variable—it can be low, high, or normal. This can be traced back to what the IOP was at the end of the procedure, the presence of residual viscoelastic, or if any red blood cells are clogging the TM. The key is not to get too hung up on post-op Day 1 IOPs, but to be aware of any
IOP spikes and treat them accordingly.
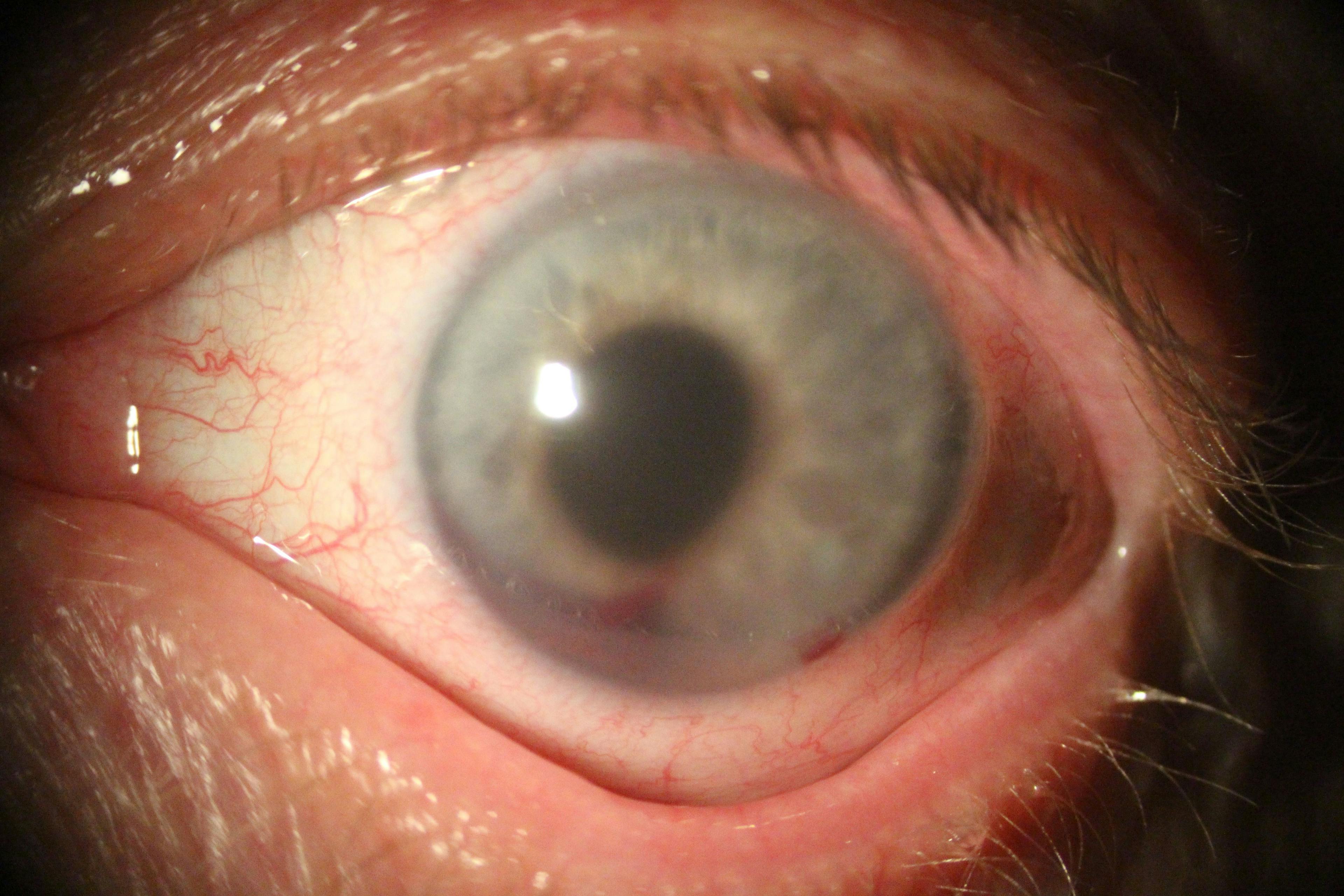
Figure 2 is a clinical image of microhyphema following a MIGS procedure.
Figure 2: Courtesy of Mitch Ibach, OD, FAAO
Post-Op Week 1
By this time, vision has usually stabilized and returned to pre-operative vision, or better if combined with
cataract surgery. The IOP can still fluctuate to some degree, and adjustments to medications may be needed if higher than desired. Remember, most commonly steroid medication is on the eye at this time point and could be contributing to the IOP fluctuations.
Post-Op Month 1
At this time, IOP is usually starting to find its new normal; however, if a patient is still on or has recently stopped using steroids, this may be impacting the IOP. Again, assess the patient and make any adjustments as needed.
Co-managing glaucoma patients and MIGS procedures
As stated, safety combined with minimal trauma are hallmarks of MIGS, but as a co-managing doctor, knowing when to ask for help or refer the patient back to the surgical practice is key. In short, follow past experiences with managing patients post-cataract surgery for vision, anterior chamber inflammation, and the worst-case scenario of intraocular infection/
endophthalmitis.
MIGS procedures can add more volatility to post-operative IOP. If the co-managing doctor cannot get the IOP into a comfortable zone with
topical glaucoma medications or oral medications, then referring the patient back to the surgeon is suggested.
How to manage non-resolving hyphema after a MIGS procedure
Non-resolving hyphema that is visually obstructing is another scenario warranting referring a post-op MIGS patient back to the surgical practice.
If at any time during the post-operative follow-up, there is extensive hyphema from reflux bleeding resulting in decreased vision or elevated IOP, it is important to discuss this with the patient and let them know there will be ups and downs during the healing phase, but that you and/or the surgeon will take good care of the patient.
Most of the time, the hyphema will resolve on its own with no intervention needed, other than topical IOP lowering drops if the pressure is too elevated for that patient. On rare occasions, an anterior chamber wash-out can be performed to remove the hyphema.
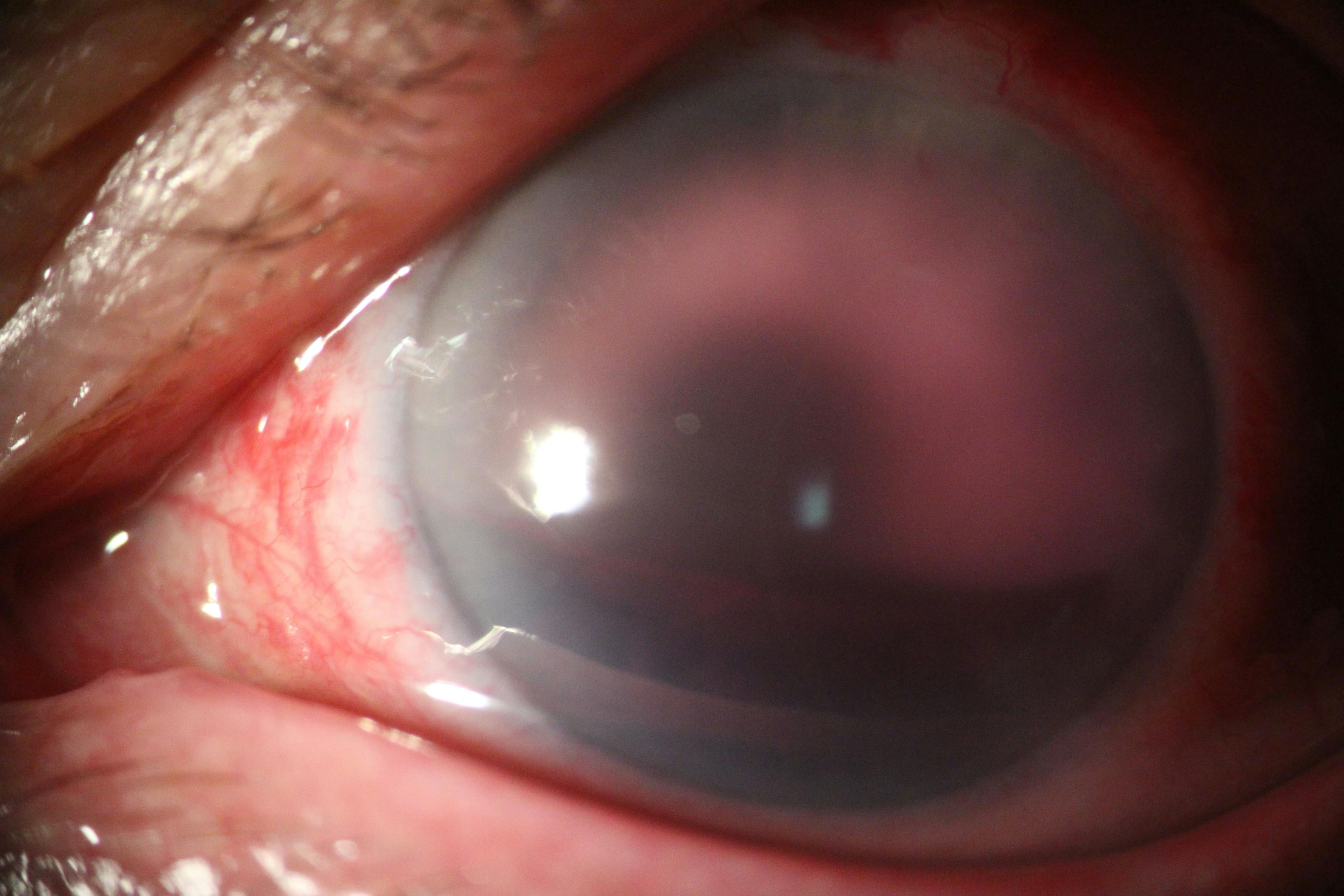
Figure 3 is a clinical image of a patient with macrohyphema following minimally invasive glaucoma surgery.
Figure 3: Courtesy of Mitch Ibach, OD, FAAO
Glaucoma medication addition and/or removal
This can vary greatly based on doctor preference and the severity of the
glaucoma. Some patients will need to continue their IOP-lowering medications throughout the post-op period and then start to reduce them as the IOP stabilizes, whereas others may stop their drops completely and then add them back on as needed.
Note: A conservative, very acceptable approach is to be cautious or avoid removing topical ocular hypotensive agents in a MIGS patient until the post-op steroid medication has washed out of the ocular system (4 to 6 weeks).
Establishing a new baseline for glaucoma patients
As patients finish the global period from their respective surgery, establishing a new baseline/target IOP, baseline VFs/OCTs, and developing a long-term management plan are the next steps.
- Intraocular pressure: Establishing a new target IOP is highly varied based on the patient's glaucoma severity and pre-surgical IOP. At a foundational level, a post-MIGS patient is still a glaucoma patient, and the VF/OCT/CH should help dictate the target.
- Expected IOP and medication decrease: IOP reduction is varied by procedure and target area of intervention. MIGS procedures done at the time of cataract surgery are expected to decrease IOP measurements more than the same procedure done in stand-alone fashion.
- In a 2019 meta-analysis of MIGS procedures, the IOP decrease ranged from 4 to 10mmHg, and the therapeutic reduction ranged from 0.7 to 2.35 medications.10
- New VF/OCT: Depending on the level of glaucoma, but in general, at 4 to 6 months post-operatively, a new VF and OCT should be acquired. This timeline is commonly earlier in severe POAG patients.
Note: This is not a rigid framework of MIGS, but rather included to provide a loose template of expectations for MIGS in the stand-alone space.
Building collaborative care
Effective
co-management practices with MIGS can greatly improve patient outcomes and ensure the best possible care. The hallmarks of these collaborative relationships rely upon consistency and cadence within the partnership.
Below are key principles for good co-management practices with MIGS procedures.
Eyecare practitioner communication
Great communication between the ophthalmologist and the patient's primary eye doctor is essential for successful MIGS treatment. The primary eye doctor can indicate their comfort level with caring for patients who have had MIGS procedures so that if the patient wishes to return to them following their surgery, everyone is in a good spot.
The ophthalmologist should provide the primary eye doctor with
regular updates on the patient's progress and what to look for in the post-operative period, as mentioned above.
Coordination of care
Effective coordination of care is important to ensure that the patient receives the appropriate care following their procedure. The surgeon and primary eye doctor should work together to develop a comprehensive treatment plan that includes regular follow-up visits and monitoring of the patient's glaucoma.
Patient education
Patients undergoing MIGS need to be fully informed with reasonable expectations given about the procedure and the post-operative care they will receive. The surgeon and
primary eye doctor should work together to educate the patient consistently on the importance of regular follow-up visits, adhering to their medication regimen, and monitoring for potential complications.
Monitoring for adverse effects
MIGS is a relatively safe and well-tolerated procedure, but like any surgical procedure, there is a risk of complications. The ophthalmologist and primary eye doctor should work together to monitor the patient for adverse effects, such as infection or inflammation, and provide prompt treatment when necessary.
Refractive management
Although not common, MIGS can impact the patient's refractive status, and in some cases, they may require a change in their glasses prescription or might need to wear
contact lenses.
Patient case 1: cataract surgery with viscocanaloplasty
Patient LF is a 76-year-old white female who presented to our practice with concerns of “washed-out” vision and struggles with night driving. LF’s best corrected visual acuity was 20/40 OD, and OS with bright acuity testing (BAT) reduced to 20/80 OD and 20/70 OS. On two ocular hypotensive drops, IOP measured 19mmHg OD and 22mmHg OS by CATS tonometry.
Baseline
corneal hysteresis was low in both eyes at 8.4 OD and 8.2 OS (reference 10.5 as normal). On continued ancillary glaucoma testing, gonioscopy is open to the ciliary body 360 degrees, and central corneal thickness (CCT) was 550 μm OD and OS.
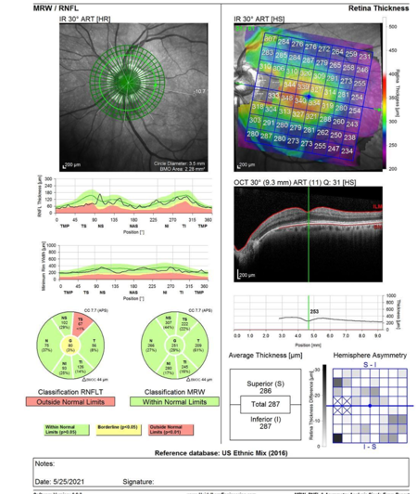
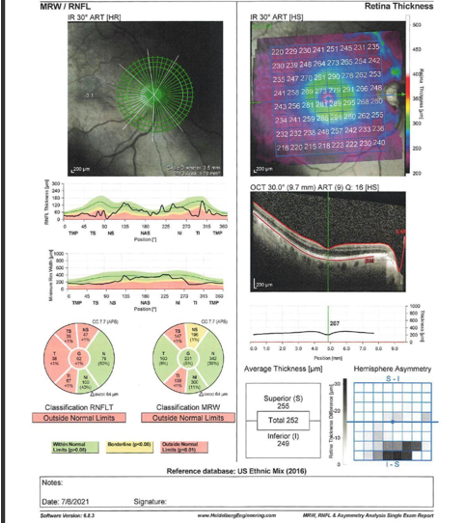
On the anterior segment exam, LF had no remarkable findings outside of visual significant nuclear sclerotic cataracts in both eyes. The posterior segment exam revealed vertical cupping of 0.70 OD and 0.75 OS, which matched RNFL thickness loss on OCT (Figure 4).
Figure 4 is a posterior segment exam revealing vertical cupping of 0.70 OD and 0.75 OS, which matched RNFL thickness loss on OCT.
Figure 4: Courtesy of Mitch Ibach, OD, FAAO
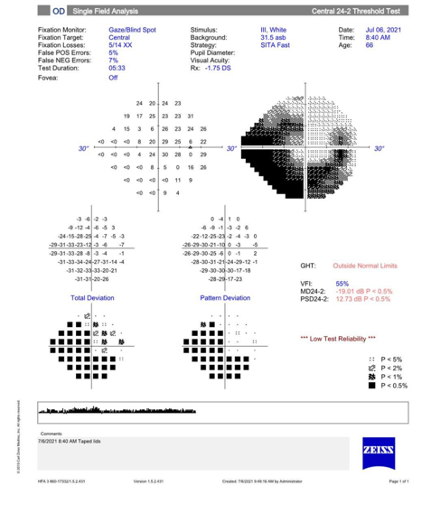
Figure 5 features optic nerve cupping/OCT RNFL loss correlated with functional loss and a superior paracentral VF defect OS.
Figure 5: Courtesy of Mitch Ibach, OD, FAAO
Patient case 1 surgical video and takeaway
In both authors’ opinions, this represents a rather clear path for this patient to be a candidate to couple cataract surgery and a combined
MIGS surgery. After thorough patient counseling, this patient elected to do standard monofocal cataract surgery along with a viscocanaloplasty (STREAMLINE, New World Medical), which was the glaucoma MIGS procedure chosen.
Viscocanaloplasty with STREAMLINE Surgical System video
Video courtesy of Michael Greenwood, MD
Takeaway: Post-operatively this patient’s IOP was consistently lower than baseline, measuring 16mmHg OU with the added benefit that the patient was able to reduce her topical drop burden by one full medication.
Patient case 2: Excisional Goniotomy plus ECP
WP is an 82-year-old Hispanic male who was referred to our practice for progressing
primary open-angle glaucoma OD. WP previously had successful cataract surgery with monofocal IOLs placed in the posterior capsule. His best-corrected acuity was mildly reduced to 20/30 OD, likely due to central VF loss (see Figure 7 below), and OS was 20/20-.
Corneal hysteresis was low OD>OS at 7.4 and 9.2, respectively. The IOP measured 29 mmHg OD and 22 mmHg OS while on a prostaglandin analogue and a combo medication. For gonioscopy, the angles were observed to be open to the ciliary body 360 degrees OU and pachymetry was 545μm OD and 565μm OS. The slit lamp exam was unremarkable outside of mild punctate keratitis OS>OD.
Figure 6 is a posterior segment exam, and with dilated fundus examination, glaucomatous cupping was observed OD>OS with grading at 0.9 OD and 0.70 OS. Figure 7 features the recorded visual fields of the patient.
Figures 6 and 7: Courtesy of Mitch Ibach, OD, FAAOUsing the referral doctor’s provided
VFs and OCTs as a reference point, it was determined that OD illustrated signs of structural and functional progression while OS remained stable over the past few years. In talking with WP, he voiced questionable compliance with glaucoma drops relating 5 to 6 days per week where he had “perfect” usage of the medications, as well as stinging/burning upon instillation.
Patient case 2 surgical video and take-home message
With both glaucomatous progression combined with ocular surface disease partially due to chronic topical IOP-lowering medications, the decision to move forward with MIGS (OD only) was made. In this patient, excisional goniotomy with KDB GLIDE (New World Medical) was partnered with ECP (BVI) to target both improving aqueous outflow while reducing aqueous inflow.
Excisional goniotomy with KDB GLIDE video
Video courtesy of Michael Greenwood, MD
Takeaway: After the MIGS procedure in the right eye only, this patient achieved an IOP in the high teens OD, and we were able to stabilize both the OCT and the VF. Once the IOP fully stabilized at the 3-month mark, both medications were altered to preservative-free options, which lessened side effects associated with ocular surface disease burden.
Final thoughts
In summary, effective co-management practices with MIGS require close collaboration between the surgeon and primary eye doctor to ensure that the patient receives the best possible
glaucoma care. Communication with a detailed referral letter, treatment target, and intentions in the post-operative period is a starting guide for the referring doctor.
Next, the surgeon and his team should relay to the patient any surgical surprises that might have occurred and the next steps to manage their care. Finally, clearly delineated expectations for the
post-operative follow-ups to maximize achievable outcomes with treatment goals inclusive of IOP reduction and potentially VF/OCT imaging stability.