



Despite playing a pivotal role in the overall health of the eyes, the eyelids tend to be overlooked in our quest to provide patients with optimal vision. Although eyelids are not often the primary cause of symptoms alone, they can cause ocular comorbidities.
Naturally, optometrists are critical in evaluating, identifying, and treating this oft ignored part of the anatomy. The eyelids contain the first line of defense from environmental elements—the eyelashes—as well as the muscles integral to replenishing the meibum layer of the tear film.1
The force of a blink also directs drainage towards the punctum, ensuring the tear film is evenly distributed while protecting the eye and enabling clear vision.1 The eyelid can also provide invaluable information about a patient’s systemic health.
Fortunately, diagnosing these conditions does not normally require advanced equipment. Most can be identified by simply using a keen clinician’s eyes, with a slit lamp as an invaluable assistant for dimensions. Anterior segment cameras and meibography can also help support the diagnosis and provide meaningful patient education.
This article aims to increase your confidence and comfort with recognizing common eyelid disorders.
Clinical feature: Red, swollen eyelids
When a patient presents with red, swollen eyelid(s), it is critical to quickly find the cause of this inflammatory response.
Most commonly, the root causes are:
- Blepharitis
- Chalazion
- Hordeolum
- Periorbital dermatitis
Anterior blepharitis
Blepharitis is a bilateral condition characterized by itchy, red-rimmed, crusty eyelids that are typically worse in the mornings. In severe, chronic cases, this can lead to lid edema.
Seborrheic blepharitis tends to feature greasy flakes with scalloped lid margins and can be associated with ocular rosacea, seborrheic dermatitis, and/or atopic dermatitis, especially in children.2 Co-management with dermatology is recommended to help treat the root cause of the seborrheic form of blepharitis.
Staphylococcal blepharitis presents with scaly flakes and dry skin of the eyelids. This form of blepharitis tends to have more corneal involvement and may lead to eyelid ulceration in severe cases.2
Figure 1: Slit lamp image of pronounced and symptomatic blepharitis.


Figure 1: Courtesy of Alan G. Kabat, OD, FAAO.
Treatments for anterior blepharitis include:2-4
- Microblepharoexfoliation
- Hypocholorous acid 0.01%
- Low light therapy with blue light
- Intense pulse light therapy (IPL)
- Radiofrequency
- Oral antibiotics, such as tetracyclines, for ocular rosacea
- Topical selenium sulfide (only available within dermatology)
- Topical combination antibiotic-corticosteroid eye drops and/or ointments for staphylococcal blepharitis
- 1000mg capsules of essential fatty acids three times/day
Anterior blepharitis treatment pearls:
- Blue light can help with the bacterial overload found on the eyelashes and improve the appearance of the eyelids.3
- Oral tetracyclines should never be used in children.
- A dosing regimen with azithromycin for 5mg/kg daily for 2 months has shown improvement in mild cases.2
Download the cheat sheet here!

Eyelid Disorders Differential Diagnosis Cheat Sheet
Use this cheat sheet to guide differential diagnoses for a wide variety of eyelid conditions.

Demodex blepharitis
Conversely, Demodex blepharitis (DB) will present with sleeving on the eyelash follicles (i.e., collarettes) and telangiectasia along the lid margins.5 In some dense cases, it can cause a misdirection of the eyelashes (i.e., trichiasis) due to the proximity to the infestation within the hair follicle.
During active episodes of trichiasis, patients often complain of a foreign body sensation. If the patient has fine eyelash hair, treatment may not be necessary, as eyelashes have a shedding cycle of between 2 and 4 weeks.5
Treatments for DB include:3,4
- Okra or tea tree oil-based lid cleansers
- IPL
- Epilation of the lashes, if trichiasis is present
- Lotilaner 0.25% ophthalmic solution (e.g., XDEMVY, Tarsus Pharmaceuticals)
Studies have demonstrated that IPL is an effective method to help eradicate Demodex mites while improving the ocular surface.2 Additionally, there is some consideration about the usage of topical azithromycin versus oral tetracyclines for the management of the meibomian gland dysfunction (MGD) associated with blepharitis.3,4
Figure 2: Slit lamp image of a patient’s lash margin with visible collarettes caused by Demodex blepharitis.

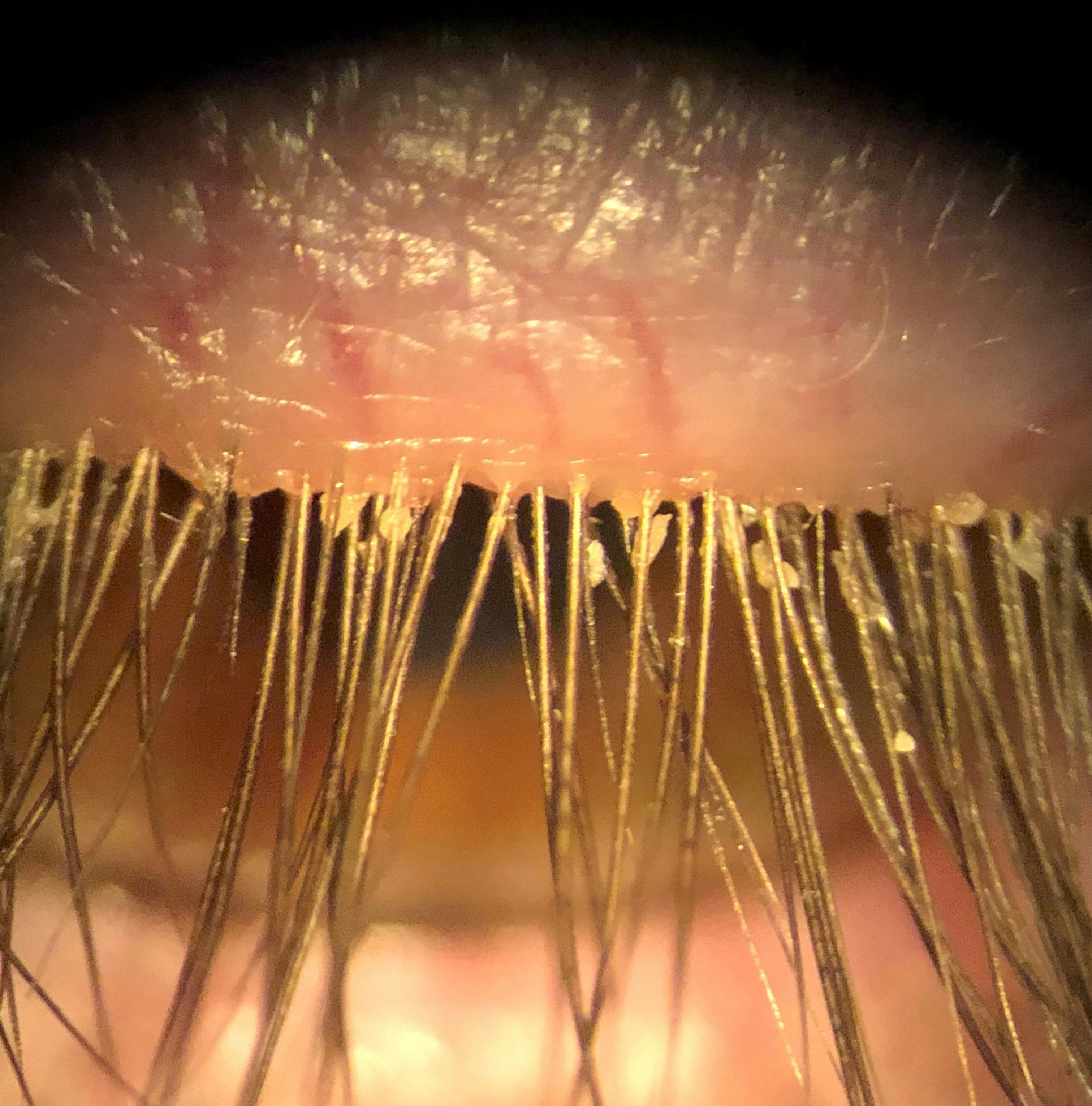
Figure 2: Courtesy of Cory Lappin, OD, MS, FAAO.
Lacrimal duct obstruction
Lacrimal duct obstruction(LDO), also known as dacryostenosis, is the congenital or acquired thinning of the lacrimal drainage system within the punctum.
The differences between congenital and acquired LDO are as follows:6
- Pediatric cases occur due to the failure of canalization of the valve of Hasner within the duct.6
- Acquired cases tend to have nonobstructive etiologies, such as dry eye and/or blepharitis or lacrimal pump failure secondary to ectropion or lid laxity.6
Epiphora is the most common presenting symptom of lacrimal duct obstruction. Prescribing a combination antibiotic-steroid ointment can be beneficial to help manage symptoms if the cause is related to blepharitis.6
Studies have further shown that a short-term dose of topical corticosteroids can help reduce tear secretion. If there is an active infection within the canaliculus, oral antibiotics (e.g., fortified amoxicillin or cephalosporins) have been useful in combination with topical antibiotic ointments (e.g., erythromycin).6
In order to confirm patency of the lacrimal duct, dilation and irrigation with a large cannula and saline solution can be performed.6 Chronic cases require a surgical solution as well as co-management with oculoplastics.
Chalazia and hordeola
A chalazion is easily differentiated from a hordeolum based on patient-reported discomfort. With hordeola, the patient typically complains about their eyelid being very tender to the touch. Whereas most chalazia can be present for weeks before a patient notices an issue, which can result in aggressively swollen eyelids.7
Figure 3: Slit lamp image of a patient with a hordeolum.


Figure 3: Hordeolum©Courtesy of Kotek1986. Tsca.bot. Image used under CC BY-SA 3.0.
If a chalazion is persistent, surgical intervention or steroid injection may be necessary to address it. Both conditions can be easily treated with combination antibiotic-steroid topical ointments, oral tetracyclines, and/or a combination of the two, for more inflamed cases.7
Warm compresses with digital massage should be included in the treatment regimen to facilitate mechanical expression of the problematic meibomian glands.
Treatment pearls for chalazia and hordeolum:7
- Tetracyclines should only be used in adult cases.
- Penicillins and cephalexin are a safer profile for children under 12 years of age.
Preseptal and orbital cellulitis
Differentiating patients with a unilateral eyelid edema from chalazion or hordeolum versus preseptal cellulitis is vital. Preseptal cellulitis is not an ocular emergency; however, it can be a precursor to orbital cellulitis if left untreated.8
Most orbital cellulitis patients will present with grotesque and diffuse eyelid swelling. The excess fluid may be so pervasive as to prevent the patient from opening the affected eye upon waking. In these patients, it is prudent to assess ocular motility, body temperature, and perform pupil testing. In addition, patients with orbital cellulitis may present with fever, pain, and diplopia.8
Conversely, these symptoms are absent in patients with periorbital cellulitis. Once it is confirmed that orbital cellulitis is not the culprit, these patients can be treated with fortified amoxicillin for 7 days until resolution.8 If the patient has a penicillin allergy, tetracycline can be an effective alternative.
Figure 4: Slit lamp image of a pediatric patient with orbital cellulitis.


Figure 4: Child with left orbital cellulitis© Dayakar Yadalla et al. Image used under CC BY-NC-SA 4.0.
Facial palsy
It is important to note that patients with acute facial palsy can present with bilateral eyelid edema, facial drooping on the affected side, and difficulties with eyelid closure. Be certain to test for eyelid closure by evaluating the functional blink. Modern technology enables computerized analysis of blink rates, blink quality, and the blink mechanism.9
Most facial palsies will self-resolve within 6 to 8 weeks without any lasting effects. Treatment for comorbidities, such as evaporative dry eye disease or MGD, is recommended.9 Referral should be made to a neurologist if there is no resolution. If there is chronic exposure keratopathy, a cornea specialist is indicated to help preserve the integrity of the cornea.
Ocular surface treatment in facial palsy patients can include:9,10
- Topical perfluorohexyloctane (MIEBO, Bausch+Lomb) for evaporative dry eyes comorbidity
- Topical anti-inflammatory agents (e.g., cyclosporine, lifitegrast) for any increased tear osmolarity indicated in chronic cases
- Radiofrequency thermal treatment (RFFT)
- Autologous serum tears for severe exposure keratitis
- Taping of the eyelids or moisture chamber goggles may be indicated if severe
Recent studies have indicated that off-label RFFT can help with incomplete blink closure and lid laxity by fortifying the collagen bonds of the periorbital skin.10
Periorbital dermatitis
In periorbital dermatitis, patients present with diffusely red, flaky eyelids on both upper and lower eyelids, making it particularly challenging. In some very severe cases, both lid edema and an overall swollen facial appearance can be noted.11 These patients are likely to complain about itching and tearing throughout the day.
The key to treatment is finding the cause of the allergy. After cessation of the irritant, most cases will resolve naturally in a couple of weeks.11 Finding the source often requires delving into the patient’s lifestyle to determine contributing factors, such as having acrylic nails applied at a salon, utilizing any new makeup or skincare products, or letting their animals sleep in the bed with them. Finding the allergen is crucial for recovery.
Cold compresses offer some temporary relief from the itchiness. However, for more chronic cases with very symptomatic patients, treat with triamcinolone acetonide 0.1% topical ointment, oral antihistamines, and/or topical tacrolimus 0.1% ointment.11
Acute, severe cases may require oral steroids. Note that, depending on state laws, it may be required that the patient’s primary care physician prescribe the oral steroid. If symptoms persist after 6 to 8 weeks, suggest allergy testing.11
Note: In patients who have glaucoma, beta-blockers and carbonic anhydrase inhibitors can cause periorbital dermatitis, which normally resolves in 2 to 3 weeks after discontinuation.11
Don't forget to check out the Eyelid Disorders Differential Diagnosis Cheat Sheet!
Clinical feature: Droopy eyelids
As patients begin to mature, so do the skin and muscles that compose the eyelids. It is important to differentiate between etiologies related to aging versus more severe systemic conditions.
Dermatochalasis is a condition in which the skin around the eyelids starts to sag, thereby touching the eyelashes, and is associated with involutional changes of the maturing eye. Diagnosis requires perimetry testing, such as a visual field.12 Visual fields should be performed first with the patient in a natural setting and then repeated with eyelids taped.
Entropion and ectropion
Ectropion refers to the outward drooping or turning of the eyelid margin, while entropion is marked by the inward turning of the eyelid margin. Ectropion tends to be more involutional, associated with Bell’s palsy and chronic rubbing of the eyelids from allergies. Entropion is linked to chemical burns, infections—such as trachoma or herpes simplex or zoster—and blepharospasm.13,14
All these conditions require lid repairs by an oculoplastics ophthalmologist. Most procedures involve sutures and can take up to 4 to 6 weeks to completely heal or for the lid to return to its normal posture.13,14
Figures 5 and 6: Slit lamp images of ectropion and entropion, respectively.


Figure 5: Courtesy of Leonid Skorin, DO, OD, MS, FAAO, FAOCO.


Figure 6: Courtesy of Leonid Skorin, DO, OD, MS, FAAO, FAOCO.
Blepharospasm
Blepharospasm is caused by unconscious contractions of the orbicularis oculi muscles and is a neurological disorder that affects the patient’s blinking, twitching, or closure.15
Blepharospasm can have some systemic implications, such as previous damage to the facial nerve (e.g., Bell’s palsy), vascular compression, injury to the brainstem, or muscular dystonias of the lower face and/or neck (e.g., Meige syndrome).15
Studies have suggested that this condition is more prevalent in:15
- Females, especially in menopausal patients
- Individuals with anxiety and/or depression
Floppy eyelid syndrome
Floppy eyelid syndrome is often misdiagnosed, unless the clinician manually flips the eyelids to reveal red, irritated palpebral conjunctiva. This is frequently associated with mild mucous discharge upon awakening.16
This condition is more common in males than females and is frequently associated with stomach sleepers and/or patients who may have possible obstructive sleep apnea.4
If the patient has not been diagnosed, but sleep apnea is suspected, a sleep study is warranted. It is important to note that when left untreated, sleep apnea can lead to hypoxia of the optic nerve and increased risk of normal-tension glaucoma.16
Figure 7: Clinical image illustrating the excessive lid laxity present in patients with floppy eyelid syndrome (FES).


Figure 7: Courtesy of Cory J. Lappin, OD, MS, FAAO.
Blepharoptosis
Blepharoptosis, or drooping of the upper eyelid, can be unilateral or bilateral. Ptosis is largely congenital or stress-driven; however, some cases can be associated with systemic implications, such as Horner syndrome, oculomotor nerve palsies, myasthenia gravis, or tumors of the eyelids or orbits.17
Patients with congenital ptosis will demonstrate an absent crease, while those with acquired ptosis will possess a heightened crease. Myasthenia-gravis-instigated ptosis presents with varying ptosis positions that fluctuate based on the patient's fatigue.18 A simple ice pack test will improve the ptosis. Blood work to confirm abnormal levels of AChR antibodies is needed.
Figure 8: Slit lamp image of unilateral blepharoptosis.


Figure 8: Blepharoptosis©Courtesy of Marian Pauly et al. Image used under CC BY-NC-SA.
If the condition is severe, it can lead to superior visual defects or diplopia, if neurologically induced.17 Diagnosis typically requires assistance from other specialties; most patients should undergo a neurological work-up with CT or MRI scans to confirm neurological involvement.
Ptosis associated with Horner syndrome demands diagnosis in a timely manner, as this syndrome perpetuates ptosis accompanied by anisocoria with ipsilateral pupil constriction with possible anhydrosis of the face.19 The diagnosis can be confirmed with apraclonidine 0.5% or 1%, wherein the Horner pupil is larger than the normal pupil after instillation.5
Clinician’s top differential diagnoses for ptosis should be:17
- Multiple sclerosis
- Pancoastal tumors
- Cavernous sinus involvement
- Internal carotid dissection
Treatment of neurologically involved ptosis requires a multidisciplinary approach. Surgical involvement may be required if it is causing superior visual defects or the patient complains of poor cosmesis.17
Note: Any ptosis from inflammatory causes, such as myasthenia gravis, cannot be surgically treated.17
Clinical feature: Eyelid retraction
Eyelid retraction is the abnormal positioning of either upper or lower eyelids wherein the sclera is more visible, even in a relaxed state. It is commonly an indicative sign of thyroid eye disease.
Thyroid eye disease
Thyroid eye disease (TED) is an autoimmune condition associated with Graves’ disease. In fact, studies have suggested that patients with Graves’-disease-associated hyperthyroidism will develop TED within 2 years.20
TED is more common in females and affects 15 to 30% of patients in Asian populations.20 However, severe, sight-threatening cases of TED tend to occur more often in males aged 50 years and older.21
TED patients may present with conjunctival and/or periorbital edema due to the overproduction of cells within the fibrofatty space of the eyes. Patients with significant lid retraction may suffer from exposure keratitis, variable levels of diplopia, and/or lagophthalmos.20
Figure 9: Close-up of a TED suspect patient with a medical history of hyperthyroidism.


Figure 9: Courtesy of Audrey Ko, MD.
Diagnosing and co-managing TED
In terms of diagnostics, a positive Korb-Blackie test can indicate this issue if the patient has incomplete lid closure. Hertel exophthalmometry is used to measure the degree of proptosis.20
A normal degree of proptosis is considered to be <21mm and ranges from 15 to 20mm based on ethnicity, sex, and age.20 A degree of proptosis >3mm from the normal range is considered clinically significant. Clinicians can determine a patient's clinical activity score (CAS) to aid in diagnosing and grading active TED.
The CAS comprises seven items, with each receiving a score of one point if present, as follows:20
- Spontaneous retrobulbar pain
- Pain on attempted up or lateral gaze
- Redness of the eyelids
- Redness of the conjunctiva
- Swelling of the eyelids
- Inflammation of the caruncle and/or plica
- Conjunctival edema, also known as chemosis
Take note that a CAS score ≥3 usually indicates active TED. Progression of TED signs and symptoms—based on worsening of vision, soft tissue inflammation, motility, or proptosis—is suggestive of active TED independent of the CAS.20
Treatment for TED can include:20,21
- Nighttime lubrication and/or sleep mask noted for lagophthalmos
- Chemodenervation with Botox
- Intravenous infusion of biological modulators (e.g., rituximab, tocilizumab, teprotumumab)
- Intravenous glucocorticoid (IVGC) therapy for moderate-to-severe cases
- Surgical intervention, dependent on optic nerve comorbidities or strabismus
- Ground prisms or sectoral occlusion with spectacle lenses for chronic strabismus or diplopia cases
Treatment pearl: Cigarette smoking cessation is recommended to reduce the risk of development and/or progression.21
Short on time? Download the Eyelid Disorders Differential Diagnosis Cheat Sheet for quick reference!
Clinical feature: Abnormally bumpy eyelids
While an uneven appearance or texture is usually benign in nature, on occasion, this presentation may be insidious in nature, making further investigation necessary.
Papilloma vs. molluscum contagiosum
Papillomas and molluscum contagiosum can be easily confused in practice. Variants of the human papillomavirus (HPV) cause papillomas, which are skin abnormalities commonly referred to as skin tags or verrucae.22 If there is growth or enlargement of a verruca, it is best to send for a biopsy, as squamous cell carcinomas can present similarly.
Conversely, molluscum contagiosum is a manifestation of poxvirus that occurs in children and immunocompromised patients. These patients present with chronic follicular conjunctivitis on the eye with lid lesion.23
All abnormalities are benign in nature and can easily resolve spontaneously or with surgical removal by an ophthalmologist. Elevated areas of discoloration along the eyelid margins can be common in darker-skinned individuals; however, should never be dismissed.24
For eyelid lesions, it is best to utilize the ABCDEs of melanoma:25
- Asymmetry
- Borders (which should be even)
- Coloration
- Diameter
- Evolution
Progression associated with eyelid lesions includes telangiectasia, increased redness due to feeder vessels, and madarosis or discoloration within the lesion.26 Feeder vessels are often engorged or prominent vessels that supply the lesion or abnormalities. Any neoplasm >6mm in diameter is very suspicious for malignancy.26
Benign eyelid lumps
Benign eyelid bumps include the following:26
- Hidrocystomas: Clogged sweat glands within the eyelid
- Translucent when light shines within the sac
- Dermoid cysts: Smooth, hard nodules
- Do not grow in size, and will not be translucent
- Xanthelasma: Yellow, smooth bumps found only in the medial part of the eyelid
- Associated with patients with high cholesterol
- Can be indicative of heart disease
These lesions do not require surgical intervention unless causing an inflammatory response, which is typically rare. Normally, when surgical excision is performed, it is for cosmetic reasons.
Figure 10: Slit lamp image of a patient with xanthelasma.


Figure 10: Xanthelasma©Courtesy of Klaus D. Peter. Image used under CC BY 3.0 DE.
Malignant eyelid bumps
The most common malignant eye lesion is basal cell carcinoma, with squamous cell carcinoma to follow. The rarer of the malignant eye lesions are sebaceous carcinoma and melanomas.
Basal and squamous cell carcinomas
Basal cell carcinomas have a pearly nodular appearance with an ulcerated center (with or without pigment and telangiectasia).26 Conversely, squamous cell carcinomas can present as scaly, flat lesions that are diffuse and not elevated in appearance, making them more challenging to identify.
Although less common than basal cell carcinomas, squamous cell carcinomas tend to be more aggressive in causing orbital involvement, along with sebaceous carcinomas.26
Figure 11: Slit lamp image of a patient with basal cell carcinoma of the lower eyelid.


Figure 11: Basal Cell Carcinoma©Courtesy of Eva Chou. Image used under CC BY-NC-ND 4.0.
Sebaceous carcinoma
Sebaceous carcinoma presents as a hard nodular lesion associated with madarosis of the eyelashes. These are commonly mistaken for recurrent chalazia or intractable blepharitis.26
Regional metastasis is the typical course for these lesions; however, studies have demonstrated that some sebaceous carcinomas can have systemic repercussions.26 For more involved lesions, dermatological intervention may be required to perform a MOHS procedure or reconstruction of the eyelid after surgical removal.
Let’s put a lid on this
In summary, the eyelids play a critical yet often underappreciated role in ocular surface health, visual function, and the detection of systemic disease.
A thorough clinical evaluation—supported by slit lamp examination and appropriate ancillary testing—allows optometrists to efficiently differentiate benign, inflammatory, infectious, neurologic, and malignant eyelid conditions.
Early recognition and targeted management can reduce morbidity, prevent progression to more serious pathology, and improve patient comfort and outcomes.
By maintaining a high index of suspicion and collaborating with other specialties when indicated, optometrists can significantly enhance comprehensive eyecare through vigilant eyelid assessment.
