




Thyroid eye disease (TED) is a rare condition that affects about one in every 6,250 women and one in every 34,482 men, according to the National Organization for Rare Disorders (NORD).1
An autoimmune disorder, TED might be referred to as Graves’ ophthalmopathy since it occurs in up to 50% of individuals with Graves’ disease, a condition that causes the thyroid to overproduce thyroid hormones (hyperthyroidism).
About 80% of TED patients will present symptoms within 18 months of their Graves’ disease diagnosis2—but alternatively, TED may be the first sign of a thyroid condition.
A brief overview of thyroid eye disease
Even though it can be correlated with hyperthyroidism, TED is a distinct disease that does require a dedicated treatment protocol. While in Graves’ disease, the immune system attacks the thyroid, in TED, the immune system affects the extraocular muscles and orbital fatty tissues, resulting in inflammation behind the eyes. It’s believed that the mechanism of action involves autoantibodies that activate an insulin-like growth factor 1 receptor (IGF-1R)-mediated signaling complex on cells within the retro-orbital space.3,4 Therefore, treating hyperthyroidism alone may not alleviate the visual and systemic symptoms and signs of TED.
TED can be a difficult condition for patients because of the physical and emotional distress it can cause. Further, it’s also a challenging condition for ophthalmologists to diagnose due to the subtleties of certain signs and symptoms, as early signs can require blood work and lab tests that can be time-consuming, necessitate new billing and coding procedures, and may be at odds with a practice’s goal of streamlined workflow and greater efficiency.
Marguerite McDonald, MD, FACS, is a cornea, laser cataract, and refractive surgeon who sees patients at OCLI Vision in New York. “One of the most challenging aspects of diagnosing thyroid eye disease is that there is no definitive test for the condition,” she admits. “It requires a new set of tests we aren’t used to performing, and often, the signs and symptoms of thyroid eye disease are so subtle, they can be easily missed.”
Audrey Ko, an adjunct assistant professor at the University of Iowa and a staff physician at Wolfe Eye Clinic, specializes in thyroid eye disease. “What I always try to emphasize with my fellow doctors and colleagues is the impact thyroid eye disease can have on a patient's mental and emotional well-being,” says Dr. Ko.
“While thyroid eye disease definitely impacts eye health and vision, most afflicted patients I see also suffer from severe deficiencies in their quality of life. The restrictions, limitations, and pain thyroid eye disease introduces into their existence can cause them to feel isolated physically and emotionally. As a result, thyroid eye disease can negatively impact employment, relationships, and self-confidence, which perpetuates the cycle of social withdrawal," she adds.5,6,7
What causes thyroid eye disease?
Although the underlying mechanisms of action in TED are not completely understood, it’s presumed that orbital fibroblasts are activated by Graves’ disease-related autoantibodies, which could lead to the release of T-cell chemoattractants.
In turn, this initiates an interaction that can ultimately result in fibroblasts expressing extracellular matrix molecules, biologic materials proliferating and differentiating into myofibroblasts or lipofibroblasts, and the deposition of glycosaminoglycans, which bind water. As a result, an individual affected by TED may experience swelling, edema, extraocular muscle enlargement, and orbital fat expansion.8 This dramatic remodeling can lead to protrusion of the eye—also known as exophthalmos—which is a hallmark sign of TED.
Visual dysfunction can result from diplopia caused by extraocular muscle restriction or from visual loss from exposure keratopathy or compressive optic neuropathy.9 Even when the visual function is spared, TED can adversely affect the quality of life (QoL) with eye pain, photophobia, tearing, and cosmetic changes ranging from eyelid retraction to disfiguring proptosis.
However, by the time your patient exhibits these physical signs, the disease may be at an advanced state, which is why early detection is critical. While most patients diagnosed with Graves’ disease are advised to have a baseline eye exam with an ophthalmologist, it’s still very important to be on the lookout for signs of TED with all patients, as it might be the canary in the coal mine that alerts patients to an underlying thyroid disorder.
What does TED have to do with dry eye disease?
TED is often associated with proptotic (bulging) eyes, but according to Dr. McDonald, this symptom may not occur until the disease advances. Unlike glaucoma, which is often asymptomatic, thyroid eye disease tends to cause eye pain and grittiness that can be misdiagnosed as dry eye disease or eye dryness due to allergies.
“Often when a patient is in an early stage of proptosis, they experience eye dryness due to nocturnal lagophthalmos, which is the inability to close their eyes all the way during sleep,” says Dr. McDonald. “Patients don’t know this is happening, but they experience eye dryness due to the fact that their corneas are exposed at night. This feeling of dryness is exacerbated as proptosis increases, which causes patients to believe they are just suffering from dry eye disease, especially if they haven’t yet been diagnosed with hyperthyroidism.”
One of Dr. McDonald’s favorite questions to ask her patients is, “When are you most miserable?” If they answer that their eyes hurt most in the morning, then this may be an indication of nocturnal lagophthalmos, which occurs as the rectus muscles elevate the globe and proptosis progresses.
How does thyroid eye disease present in the early stages?
Drs. Ko and McDonald encourage all eyecare providers to look for signs of thyroid eye disease in all patients while conducting routine eye exams.
“If you are doing a retina exam and see these red and inflamed rectus muscles which move the eyes from side to side, then you want to get to the bottom of that,” says Dr. McDonald. “It can be easy to speed through these basic tests, but it’s really important to look for any indication of redness or swelling in the eye, as it’s typically a sign of a pathology.”
Case #1: A TED suspect
A 54-year-old female presented with a 6-month history of bilateral pain, swelling, pressure, and headache around both eyes. She was treated for dry eyes and allergies, but symptoms did not improve. Her past medical history was significant for hyperthyroidism, but currently, she was hypothyroid.
Figure 1 is an image of a TED suspect patient with a medical history of hyperthyroidism.


Figure 1: Courtesy of Audrey Ko, MD, with patient permission.
External and slit lamp examination findings:
- Best-corrected visual acuity (BCVA): 20/20 bilaterally
- Pupils: Round and reactive without APD
- Intraocular pressure (IOP): 27mmHg OD and 28mmHg OS
- Color vision was intact bilaterally
- Extraocular motility was full bilaterally
- Exophthalmometry measured bilateral exophthalmos of 26mm OD and 27mm OS
- Clinical examination was remarkable for bilateral exophthalmos, upper eyelid retraction, mild chemosis, and caruncular edema
This patient's examination was suspicious for thyroid eye disease, and therefore additional workup was obtained. Thyroid autoantibody testing showed elevated thyroid stimulating immunoglobulin (TSI). Further, the computed tomography (CT) scan of the orbits illustrated bilateral exophthalmos associated with mild thickening of the inferior and medial rectus muscles, as well as fat stranding within the orbit. Visual field and retinal nerve fiber layer (RNFL) testing demonstrated healthy nerve function.
Consequently, she was diagnosed with thyroid eye disease and subsequently underwent monoclonal antibody treatment and bilateral upper eyelid retraction repair. Notably, after thyroid eye disease treatment (Figure 2), the IOP normalized to within normal limits after the thyroid eye disease was under control.
Figure 2 shows the same patient after undergoing TED treatment with monoclonal antibody treatment and bilateral upper eyelid retraction repair.

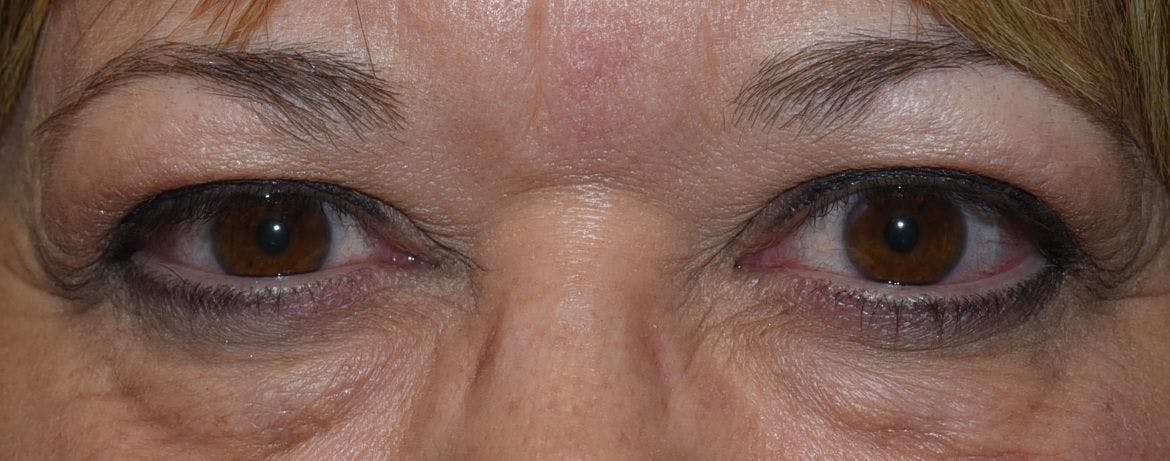
Figure 2: Courtesy of Audrey Ko, MD, with patient permission.
What are the emotional implications of thyroid eye disease?
A recent study found that patients’ quality of life, as evaluated by US physicians, is highly impacted by the activity and severity of TED.10 Additionally, mental health issues were more frequently reported by patients with TED than in the general US population. Ocular pain, strabismus, and diplopia appear to be the main drivers of physician-perceived QOL impairment in this sample of US patients with TED.
“Some doctors find it hard to manage thyroid eye disease,” says Dr. Ko, “I understand, as this can be a challenging condition to diagnose. Plus, patients who are in pain experience a greater level of stress and the emotional impact of their changing appearance. As doctors, we can really make a difference by understanding what a patient may be dealing with and proactively advocating and providing solutions for them.”
What questions should doctors ask patients they suspect may have TED?
If Dr. Ko believes a patient may be suffering from TED or she receives a referral from an optometrist, she begins her initial consultation with questions that provide deeper insight into a patient’s history, current medications, supplements, and any recent medical diagnoses.
“Some patients I see already have a diagnosis of thyroid dysfunction, so I also take care to ask about any changes in their thyroid medication or any recent or new diagnoses,” says Dr. Ko. “Many are also on supplements. Some take diet pills or an exogenous thyroid hormone, and I want to know about all of those additions to their basic routines as well as any radioactive iodine treatments or thyroidectomies they may have already undergone."
"I take rigorous notes about their procedures and the timeline so I can get a better picture of how their symptoms may be related. Now that smoking and vaping are on the rise, I also ask about those habits as they can affect so many systems in the body," she added.
What many doctors may not be aware of is the pain that TED patients experience on a regular basis. Sometimes, the pain is a constant deep ache behind the eyes,11 and other times, the patient experiences a more gritty feeling of discomfort on the ocular surface. Combined with a change in their appearance, TED can impact a patient’s self-esteem, cause stress at home, and lead to problems in their careers, especially if they are restricted from driving.
Factoring in the chronic nature of thyroid eye disease
“Patients with TED often forget that not everyone suffers the way they do,” says Dr. Ko. “What’s been remarkable to me is how variable the pain and symptoms are. Sometimes, it’s day-to-day, and other times, it’s hour-to-hour. That’s why I always ask them, ‘How’s it going today—is it a good day or a bad day?’ A chronic disease like TED develops over time, and often, patients just learn to put up with it," explains Dr. Ko.
"They don’t complain until it’s actually really bad, so I always try to see how they are doing on the day that they see me and get a deeper insight into how that relates to what they experience regularly. I really want to know what their ‘normal’ is like.”
Dr. Ko also follows up by asking for more details about their best and worst days or whether they see swelling and redness, any blur to their vision, or are experiencing dry eye symptoms. Alternatively, a patient may have inflammation of soft tissue or very minimal changes to their eyelids. Other patients might not have any visible inflammation at all but have progressive symptoms indicated by double vision, dry eye symptoms, visual field changes, or photophobia.
“It is important to distinguish between ocular surface versus deeper orbital issues,” she adds. “So I try to follow up with questions to distinguish whether it’s more a sandy, burning, or dry feeling versus a deep dull, aching pain behind their eyes that may worsen when they move their eyes.”
If Dr. Ko is seeing a patient who has chronic TED, she conducts a visual field test to detect any aberrations in optic nerve function, which can indicate a more severe form of TED. “I’ve had quite a few patients in this category who are experiencing visual field loss secondary to optic nerve compression, and they didn’t even know it because otherwise, they were asymptomatic,” says Dr. Ko.
Labs and images to order if you suspect TED
“When I’m assessing TED severity and activity, I obtain laboratory testing, orbital imaging, and optic nerve testing,” says Dr. Ko. “The laboratory testing is focused on determining the thyroid function and detecting autoantibodies associated with TED, such as TSI and thyroid stimulating hormone (TSH)-binding inhibitory immunoglobulin (TBII).
Orbital imaging allows for visualization of how large the extraocular muscles are, and if the optic nerve is being compressed or stretched as a result of the enlargement. Finally, visual field testing and RNFL measurements give me an idea of whether the optic nerve is currently or has previously undergone damage.”
Dr. McDonald also looks for elevated T3 and T4 levels and low TSH. “Patients with thyroid eye disease are often making so much thyroid hormone that their TSH levels are lower than normal,” she says. “So one set of values is higher than normal, and the other is lower.”
Both doctors acknowledge that because TED might arise independently from hyperthyroidism, there may also be incidences where you are convinced that a patient has TED, but the clinical tests are negative. “In those instances, I also order magnetic resonance imaging (MRI) of the orbits to see if the extraocular muscles are enlarged or inflamed. This may allow for detection of TED in patients with subtle or early presentation of the disease,” says Dr. Ko.
Dr. McDonald also relies on MRI scans of the orbit. “CT scans are not nearly as useful as an MRI in terms of looking at the rectus and oblique muscles.”
Case #2: Smoldering symptoms to acute presentation of TED
A 70-year-old diabetic male presented with a 1-year history of eye pain and irritation. He had been treated for dry eye with artificial tears but continued to have the sensation of grittiness, which never fully went away. Within the last couple of months, he started noticing blurry vision that progressed to double vision within the last couple of weeks.
His past medical history was significant for a history of radioactive iodine (RAI) therapy 2 years ago. He experienced some eye dryness and puffiness after this treatment, but it went away without intervention within a couple of months.
Figure 3 depicts a patient prior to TED treatment with a medical history of RAI therapy and persistent ocular grittiness that advanced to double vision.


Figure 3: Courtesy of Audrey Ko, MD, with patient permission.
External and slit lamp examination findings:
- BCVA: 20/25 bilaterally
- Pupils: Round and reactive without APD
- IOP: 16mmHg OD and 17mmHg OS
- Color vision was intact bilaterally
- Extraocular motility showed mild right abduction and adduction limitations, and mild left abduction limitation
- Exophthalmometry measured 22mm on the right and 21.5mm on the left
- Clinical examination was remarkable for caruncular edema, chemosis, and mild periocular fullness
Although common clinical signs associated with active thyroid eye disease (marked upper and lower eyelid retraction, periocular skin redness, marked periocular fullness, or exophthalmos) were not present on examination, the patient's history of thyroid dysfunction, RAI, development of diplopia, and clinical finding of chemosis pointed to an orbital process suspicious for TED.
Laboratory testing showed TSH, T3, and T3 within normal limits, but thyroid autoantibody testing showed an elevated TSI. A CT scan of the orbits showed bilateral extraocular muscle enlargement, more severe on the right compared to the left.
Figure 4 features a coronal CT scan of the patient.

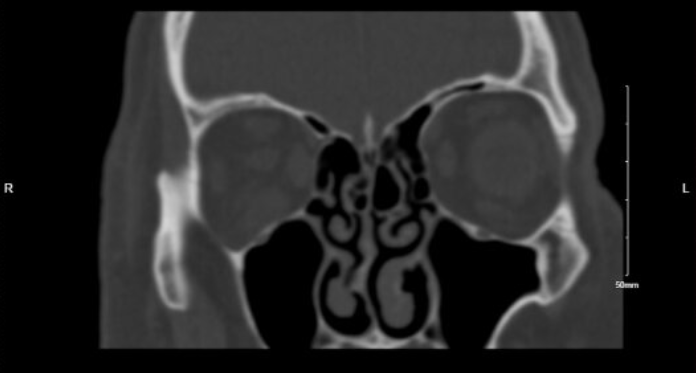
Figure 4: Courtesy of Audrey Ko, MD, with patient permission.
He was started on steroid treatment and had moderate control of symptoms and inflammation while he was on higher doses; however, the disease would flare at lower doses. After the failure of disease control on steroids, he was started on monoclonal antibody therapy. Marked improvement was seen after the second infusion, with a total treatment course of eight infusions. The patient had resolution of all symptoms and felt he had returned to the pre-disease baseline appearance.
Figure 5 shows the patient following a TED treatment composed of infusions of monoclonal antibody therapy.


Figure 5: Courtesy of Audrey Ko, MD, with patient permission.
What to look for in follow-up appointments with TED patients
“At a patient’s initial consultation for a possible diagnosis of TED, I explain that it is a heterogeneous disease that presents differently in each patient. Therefore, I will need to look at all the laboratory results and orbital imaging in the context of the clinical examination before making a diagnosis,” says Dr. Ko.
“Patients can get worried after not hearing back after a portion of their workup is completed, so I make it a point to explain that we need all the information back before making a diagnosis. This is important to rule out other diseases that can present similarly, such as orbital tumors or idiopathic orbital inflammation (IOI).”
The script Dr. Ko relies on for the second appointment is simple and to the point. “I usually thank them for getting the tests and coming back in for a follow-up. I tell them I’ve had a chance to review their results, and then I get right to it and let them know if they have a TED diagnosis or not.”
Both doctors share imaging results with their patients and emphasize the importance of educating patients and enabling them to visualize what is happening with their eyes.
“I show the patient their orbital scan images. It is helpful for patients to see the extraocular muscle enlargement and understand why they are having double vision and exophthalmos. I also discuss their labs, optical coherence tomography (OCT) analysis of their RNFL, and visual field tests,” adds Dr. Ko. “At this stage, the conversation is about how we can prevent what is happening from progressing and safeguard their vision.”
Discussing at-home monitoring and TED treatments with patients
Dr. McDonald sometimes asks a patient to see an older photo or their driver’s license because the disease can progress so slowly a patient might not even notice how their eyes are changing.
“I advise patients to be proactive in checking vision at home. An easy way to monitor for optic nerve compromise is to routinely and informally check their vision—one eye at a time—and conduct a basic red desaturation test, which assesses the integrity of the optic nerve by testing the ocular sensitivity to the color red,” says Dr. Ko.
“This is an easy test that patients can do at home by looking at a bright red target, such as red nail polish. It’s a quick and dirty color vision test they can do to make sure each eye is detecting the same level of brightness in response to color. I make sure they know to let me know of any changes they are seeing.”
Treatment options are typically discussed in follow-up appointments, which can include artificial tears and dry eye medications, steroids, radiation, or medications delivered via infusion. If a patient has an active TED case without optic nerve compression, Dr. Ko likes them to return in 3 to 6 months, but if a patient has a more stable condition, she may see them annually.
“It can be easy to let patients with quiescent thyroid eye disease slip through the cracks, so I make sure to see them every 6 to 12 months and follow up with their optometrists,” says Dr. Ko. “They can go years and years without evaluation and slowly lose vision. I’m very proactive with reaching out to their ODs and love co-managing because I know someone is always keeping an eye on them.”
What co-management and follow-up strategies are most effective for TED patients?
Many referrals to thyroid eye disease specialists often come from optometrists, some emanating from endocrinologists, and a few patients who self-refer themselves who might have been misdiagnosed as having dry eye disease in the past but who suspected something more serious.
“In regards to managing these patients with their regular eyecare providers, I find it very easy,” says Dr. Ko. “Patients are excited to be able to continue seeing their regular eye doctor for disease monitoring closer to home. Routine testing such as RNFL, visual field testing, and color vision testing allow for close regular monitoring of optic nerve function. That allows for early detection of any changes, and therefore earlier intervention as well.”
In Dr. Ko’s practice, she makes sure that her TED patients see one of two staff members who have a special interest in thyroid eye disease. She believes this helps the patient feel more comfortable when they have consistent contact with specific staff members who are coordinating their care with their primary care physicians, optometrists, and endocrinologists.
Finally, she recommends sending an official letter to a patient’s other providers that informs them about:
- The TED diagnosis
- The treatment plan and possible side effects
- The potential for disfiguring effects and vision loss
What therapies are currently available to treat TED?
As with diagnosing TED, knowing which treatments to recommend can be challenging for ophthalmologists. Reconstructive surgery is typically reserved for inactive TED or as an emergent vision-preserving measure for compressive optic neuropathy. Oral and intravenous glucocorticoid therapy has been used for decades with variable efficacy in acute TED, but results may be temporary and side effects significant. Nonsteroidal oral immunosuppressive agents offer modest benefits in TED.
Several immunomodulatory monoclonal antibodies, including rituximab and tocilizumab, have shown efficacy in inactivating TED. Recently, teprotumumab, an IGF-1R inhibitor, has demonstrated significant improvement in proptosis, clinical activity score (CAS), diplopia, and quality of life in patients with active TED, with favorable tolerability.12
Final takeaways
For ophthalmologists treating patients they suspect might have TED, Dr. McDonald and Dr. Ko have three recommendations:
- Ask about eye dryness and pain—and whether it’s worse upon waking.
- Look for red and inflamed rectus muscles on the retina exam.
- Don’t be afraid to order blood work to assess thyroid function.
While proptosis may be the most recognizable sign of TED, it is not usually the earliest to appear, and these more subtle signs and symptoms might be crucial to early diagnosis and treatment options.
“Thyroid eye disease is a challenging condition for both doctors and patients,” says Dr. McDonald. “I don’t think enough ophthalmologists know about the condition currently, and I hope that changes.”
