



With increasing demands for medical eyecare, optometrists today diagnose, treat, and co-manage a growing number of patients with ocular manifestations of systemic disease.
While some chronic diseases are more common than others, it’s vital for eyecare providers to understand the associated ocular sequelae of their patients’ systemic condition(s).
In this article, we’ll review what sleep apnea is and how it can impact the ocular and systemic health of our patients. We’ll look at common ocular findings these patients may present with, as well as treatment and management options optometrists can use to provide quality patient care.
What is sleep apnea?
Obstructive sleep apnea (OSA) is characterized by fragmented sleep, nocturnal arousal, and abnormal oxygen desaturation due to repetitive upper airway collapse while sleeping.1
Patients with OSA may experience chronic poor sleep quality, snoring, choking arousals, and neurocognitive impairment. Additionally, patients may even experience motor vehicle accidents due to fatigue or “micro sleeps” while driving. OSA has been shown to cause breathing cessation for as long as 2 minutes when sleeping.2
The burden of disease and decreased quality of life associated with OSA is a major public health concern. Approximately 30% of US adults between 30 and 70 years of age have some form of OSA.3
The prevalence is greater in males as compared to females. There is a higher prevalence of OSA among individuals with cardiometabolic co-morbidities like hypertension, type 2 diabetes, obesity, and coronary artery disease.1
Sleep apnea and retinal disease
OSA has been shown to increase the risk of various retinal pathologies, including vascular tortuosity, diabetic retinopathy, age-related macular degeneration (AMD), geographic atrophy, retinal vein occlusion, and central serous chorioretinopathy (CSCR).4,5
There are several proposed mechanisms for an increased prevalence of retinal vascular pathology with OSA. Prolonged periods of OSA cause a decrease in arterial oxygen levels while increasing carbon dioxide. Decreased oxygen saturation levels, increased hypercoagulable states, elevated lipoprotein levels, increased arterial blood pressure, and increased intracranial pressure are also present in OSA.4
Sleep disordered breathing has also been shown to promote the production of advanced glycation end products (AGEs) as well as cause inflammation, and oxidative stress.6 This leads to vascular endothelial dysfunction, which plays a role in many of the aforementioned retinal vascular pathologies.
Sleep apnea and retinal vein occlusion
Approximately 16.5 million people are affected by retinal vein occlusions globally.7 It has been shown that up to 77% of patients with retinal vein occlusion demonstrated sleep-disordered breathing consistent with OSA.13
Figure 1 highlights central retinal vein occlusion OD in a 68-year-old male with concomitant OSA, obesity, and type 2 diabetes. Of note, sleep apnea has been shown to promote hypercoagulability and increase arterial blood pressure—both likely mechanisms for an increased prevalence in retinal vascular occlusions with OSA.


Figure 1: Courtesy of Kevin Cornwell, OD. Taken with Topcon Maestro OCT/Fundus Camera.
Sleep apnea and CSCR
Patients with OSA also have increased sympathetic activity, which increases levels of circulating epinephrine and norepinephrine.10 When these molecules are present in excess, the risk of developing CSCR increases. It has been shown that patients with OSA are up to three times more likely to develop CSCR when compared to healthy controls.10
Figure 2 shows optical coherence tomography (OCT) imaging and a fundus photograph of CSCR OD in a 54-year-old male with sleep-disordered breathing. Sleep apnea can promote sympathetic activity and increase circulating epinephrine and norepinephrine, both of which can increase the risk of developing CSCR.

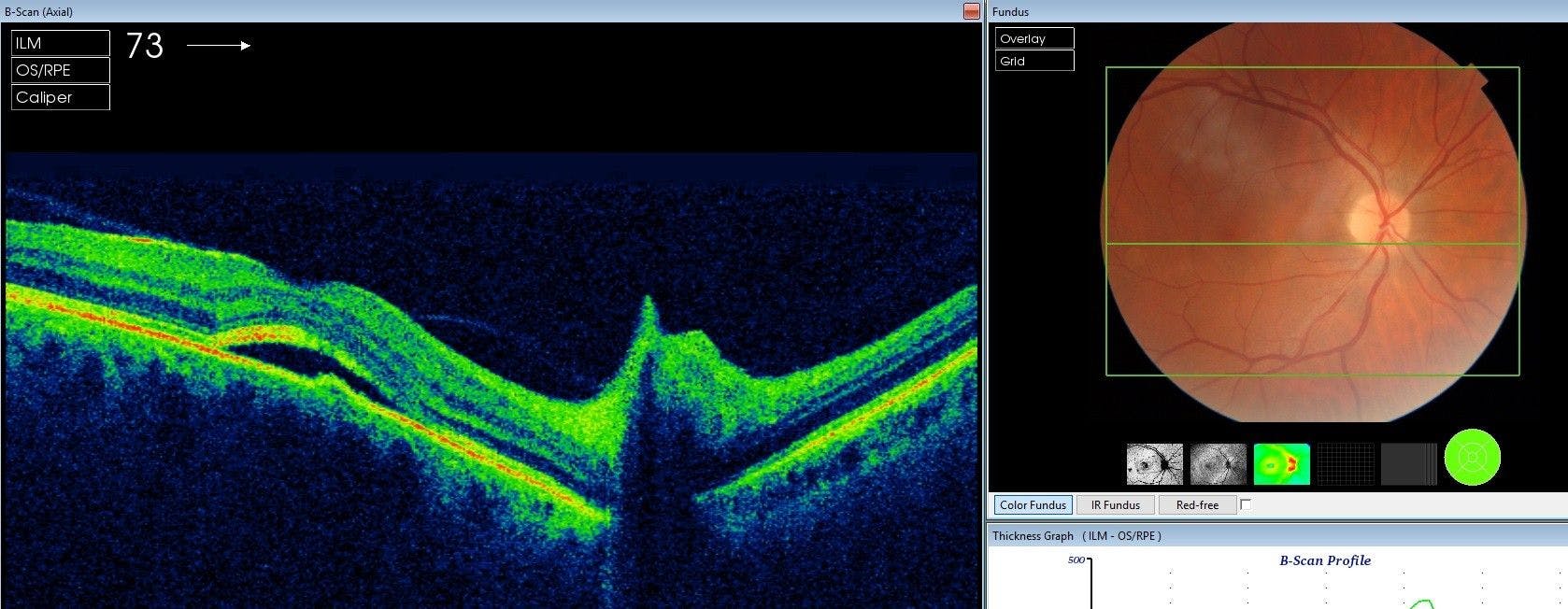
Figure 2: Courtesy of Kevin Cornwell, OD. Taken with Topcon Maestro OCT/Fundus Camera.
Sleep apnea and diabetic retinopathy
OSA is independently associated with an increased risk of developing sight-threatening diabetic retinopathy. OSA and diabetes ultimately lead to pathologic retinal ischemia—setting the stage for increased vascular endothelial growth factor (VEGF) levels and subsequent retinopathy and neovascularization.
Patients with diabetes and concomitant severe OSA are up to 15 times more likely to develop advanced diabetic retinopathy.11
Figure 3 demonstrates severe non-proliferative diabetic retinopathy OU in a 63-year-old female with OSA. Sleep apnea-induced retinal ischemia can promote VEGF release and increase the risk of developing sight-threatening retinopathy in patients with diabetes.

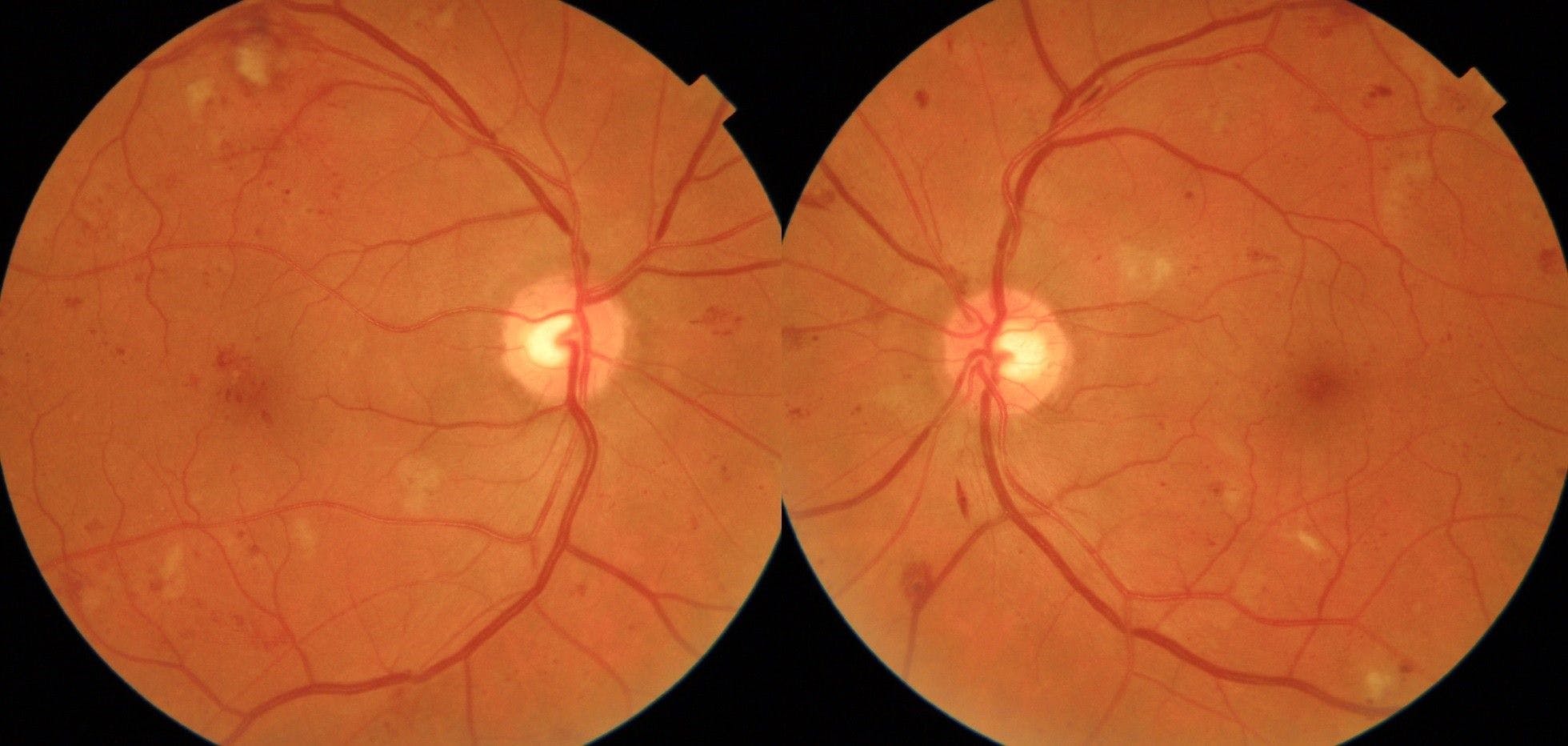
Figure 3: Courtesy of Kevin Cornwell, OD. Taken with Topcon Maestro OCT/Fundus Camera.
Sleep apnea and AMD
Figure 4 highlights OCT imaging and fundus photographs of moderate non-exudative AMD OU in a 71-year-old female with OSA. Having a diagnosis of OSA also increases one’s risk of developing macular degeneration by up to 40%.9

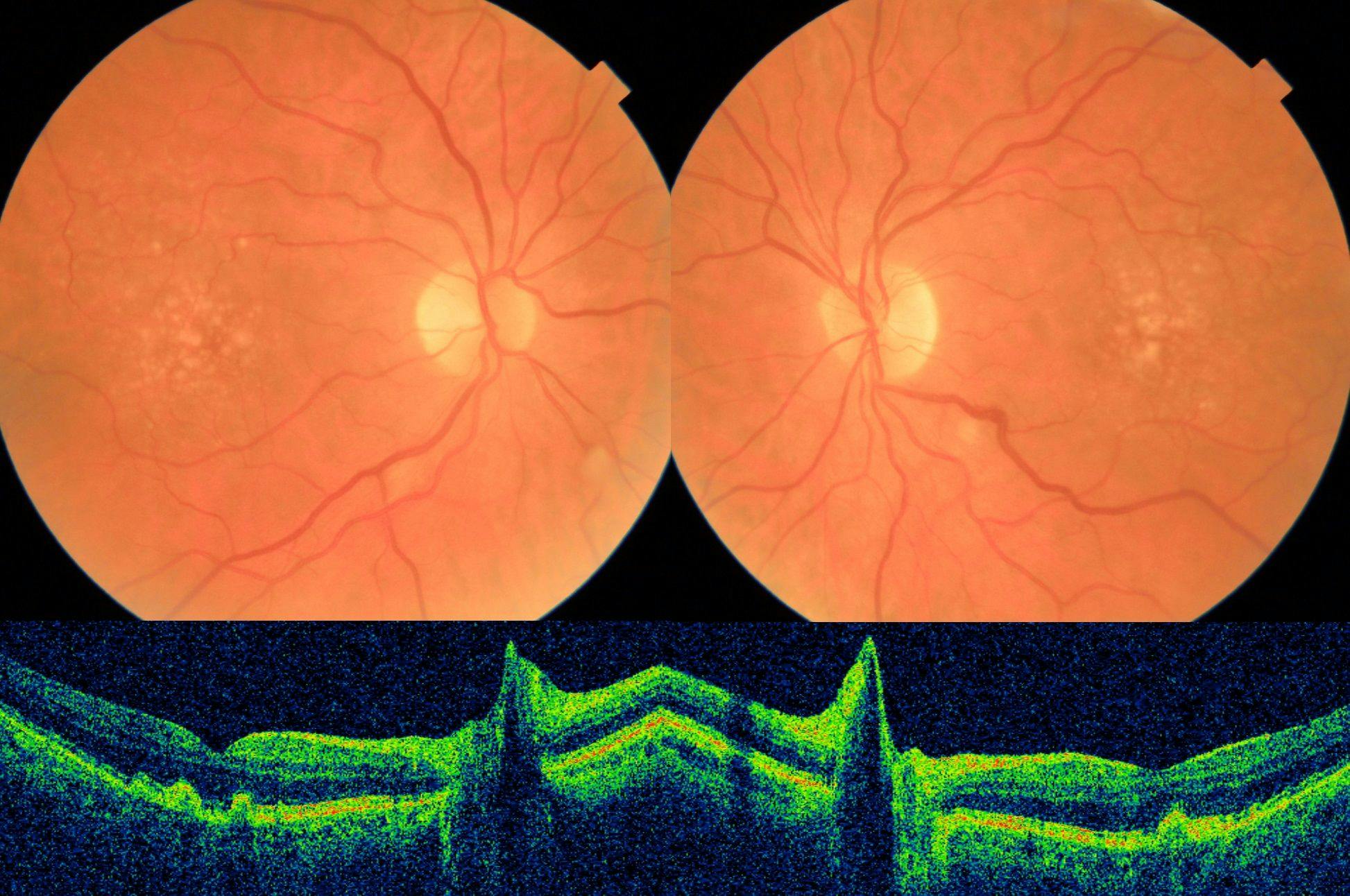
Figure 4: Courtesy of Kevin Cornwell, OD. Taken with Topcon Maestro OCT/Fundus Camera.
Sleep apnea and optic nerve pathology
Patients with OSA are at an increased risk for developing various ocular diseases of the optic nerve as well. These include normal tension and primary open-angle glaucoma, non-arteritic ischemic optic neuropathy (NAION), papilledema, and idiopathic intracranial hypertension.5
Up to 50% of patients with glaucoma have been shown to have OSA.5 Further, patients with OSA are over twice as likely to develop glaucoma when compared to someone without sleep-disordered breathing.13
Similar to OSA and retinal pathology, there are similar proposed mechanisms for an increased prevalence of optic nerve pathology with OSA. Nocturnal hypoxia to the optic nerve from sporadic cessations in breathing and increased diurnal intraocular pressure (IOP) fluctuations with the use of a continuous positive airway pressure machine (CPAP) are two common theories.5
Figure 5 shows primary open-angle glaucoma OU in a 68-year-old male with a history of obesity, type 2 diabetes, and OSA. Sleep apnea-induced ocular ischemia can increase the risk of developing both normal tension and primary open-angle glaucoma.

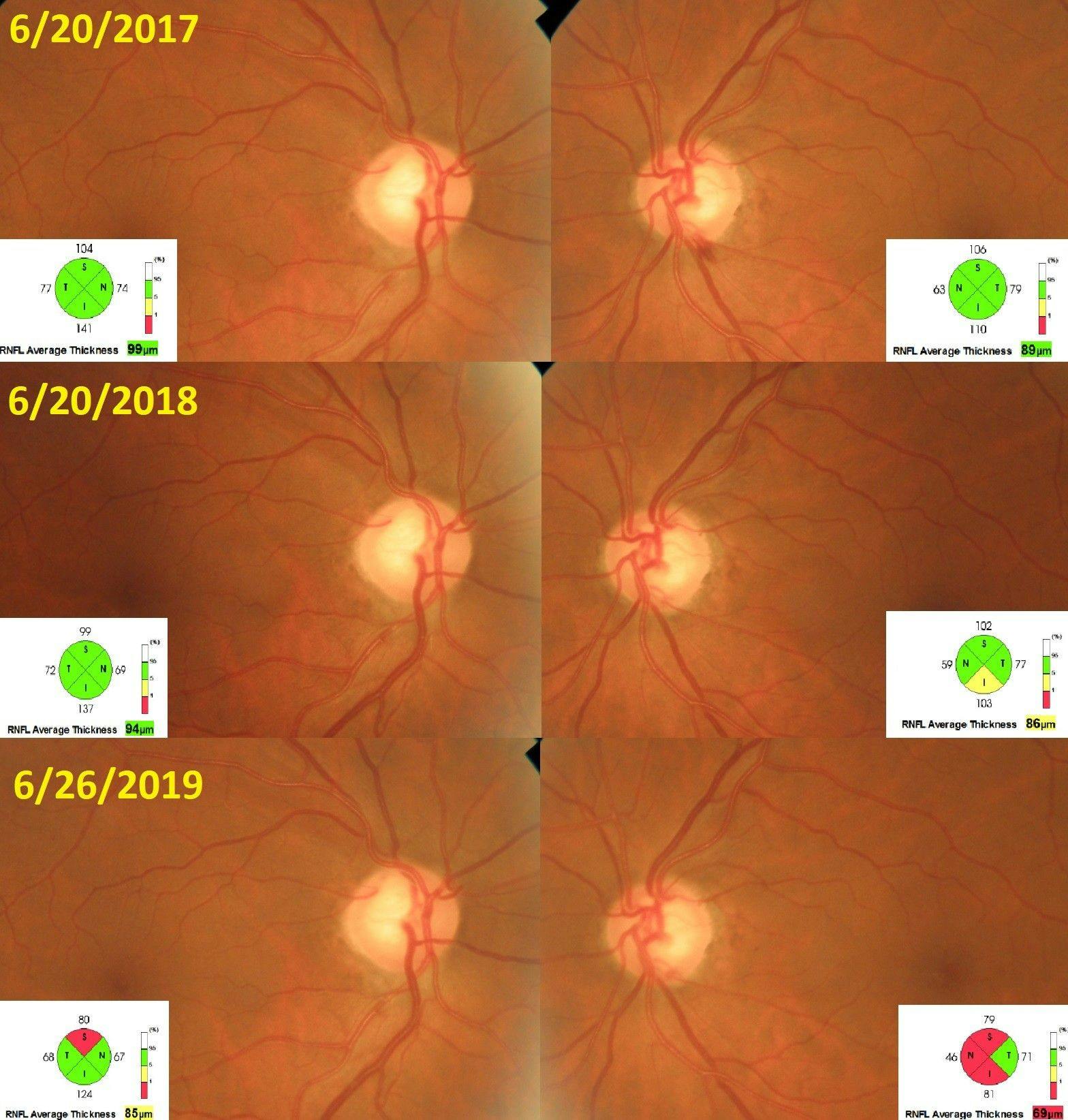
Figure 5: Courtesy of Kevin Cornwell, OD. Taken with Topcon Maestro OCT/Fundus Camera.
Co-managing sleep apnea
Clinicians may opt to follow their patients with OSA more closely, given their increased risk of various ocular diseases and progression. Patients need to be educated on the basic pathophysiology of their ocular condition and understand how chronic disease(s) can potentially jeopardize their ocular health status.
When referring OSA patients for any ocular surgery, it is important to accurately document their systemic and ocular histories. Patients with OSA are more likely to have floppy eyelid syndrome and subsequent dry eyes.13
These OSA-related ocular sequelae of the anterior segment may pose a potential challenge for the surgeon. Additionally, routine use of a CPAP machine can also lead to severe dry eye symptoms and should be managed accordingly.
While optometrists do not directly treat and manage OSA, it is important to understand what resources are available for patients. Patients suspected of having ocular findings associated with OSA should immediately be referred to their primary care physician for polysomnography sleep testing.
Recommended treatments for sleep apnea
According to the American Academy of Sleep Medicine, several treatment options exist for patients with OSA, both surgical and non-surgical.6 A CPAP machine is recommended as first-line therapy for adults with symptoms of OSA and any major upper airway anatomic abnormality.11
Interestingly, CPAP treatment has been shown to decrease plasma VEGF concentrations.12 Many times, a patient’s primary care doctor can order polysomnography testing and prescribe CPAP therapy.
Referral for upper airway surgery may also be an option for patients who are intolerant to or show poor compliance with CPAP treatment. These procedures are typically performed by an ear, nose, and throat surgeon. Referral to a bariatric surgeon may also be warranted in adults with OSA and obesity (BMI ≥35kg/m2) who have poor responses to CPAP treatment.11
Conclusion
With today’s optometrists providing more medically-based eyecare, it’s crucial for them to understand the systemic diseases their patients present with. Sleep apnea is one of many chronic diseases patients may present with to their optometrist.
It is important that optometrists and eyecare providers understand the nature of sleep apnea, as well as the ocular sequelae that may occur. Each of these downstream effects of OSA can further exacerbate the aforementioned ocular pathologies that optometrists diagnose and manage.
Clinicians should pay close attention to their patients with OSA, especially with concern for ocular diseases like glaucoma or retinal pathology, and consider monitoring them more closely. Ocular findings indicative of sleep apnea may precede a formal diagnosis of OSA.
When managing these patients, they must address their underlying co-morbidities in addition to standard-of-care treatments for their ocular disease. It is crucial to share any pertinent eye exam findings with the patient as well as other key healthcare providers. Co-management with primary care, pulmonology, and other medical specialists may be necessary.
Building a doctor-patient relationship with these patients is a great way to establish rapport and meet their eyecare needs.
