





Retinal imaging is a valuable tool in comprehensive ophthalmic exams that helps clinicians diagnose ocular diseases and monitor their progression.
Optometry and ophthalmology offices, and more recently, primary care offices (e.g., family medicine), often use it in managing various diseases such as diabetes, as diabetic retinopathy (DR) is one of the leading causes of blindness in middle-aged adults in the United States.
Over the past few years, non-mydriatic (i.e., undilated) teleretinal imaging has improved overall patient compliance with retinal screening exams. However, it is still only a screening tool that should be utilized in addition to regular slit-lamp and dilated fundus examinations.
Here, we discuss the advantages of teleretinal screening programs and some pitfalls in clinical cases that remind us that teleretinal images should be used as screening rather than an all-encompassing tool.
Advantages of teleretinal screening
General recommendations from different societies encourage diabetic retinal exams 5 years after diagnosis for type 1 diabetes and at the time of diagnosis for type 2 diabetes. However, the compliance rate for these exams was very low until recently, teleretinal imaging was developed to provide an initial patient assessment in the primary care setting.
This has a positive impact on meeting quality metrics like Healthcare Effectiveness Data and Information Set (HEDIS) and Medicare Advantage Stars.
Using teleretinal screening to assess for diabetic retinopathy
Teleretinal programs provide a way to screen diabetic patients for retinopathy in a primary care setting. Trained medical assistants and office staff use non-mydriatic digital cameras to capture retinal images. These cameras only require basic training, which makes teleretinal screening an easy-to-integrate program for non-ophthalmologists across the country.
Subsequently, trained providers interpret the images. Primary care physicians receive a copy of the interpretation with further recommendations. Some specialists, like endocrinologists, also offer patients in-office teleretinal screening options.
Another model of using teleretinal screening is capturing these images in ophthalmology or optometry offices. After interpretation, the office staff calls the patient with further provider recommendations. A less commonly used practice pattern involves a video call while simultaneously taking photos of the retina with immediate diagnoses and counseling for patients.
Protocols to evaluate patients for diabetic retinopathy
For patients with evidence of diabetic retinopathy, teleretinal screening can be further classified by the evidence of non-proliferative or proliferative diabetic retinopathy disease. Retinal images can detect the presence of hemorrhages, retinal scars, and retinal detachments.
Images can detect lipid exudates and cotton wool spots, which are also seen in patients with high blood pressure. The retinal images also give a clear view of the optic nerve, which could be a quick screening tool for glaucoma suspects or patients with optic nerve edema.
“In images without evidence of retinopathy, the recommendation is annual re-imaging.”
For patients with evidence of mild to moderate retinopathy, a referral to an ophthalmologist for further evaluation and more frequent monitoring is recommended. Patients with severe diabetic retinopathy are often referred to retina specialists directly, depending on local demographics.
The role of artificial intelligence (AI) in screening for DR
There are now artificial intelligence diagnostic systems like IDx-DR that can recognize diabetic retinopathy and categorize teleretinal images into no-mild and moderate-severe. These systems automatically recommend re-imaging in 1 year and referral to ophthalmologists, respectively.
Some drawbacks are that the system does not indicate the level of urgency for patients in the moderate-severe group, which would mistakenly result in a patient with less severe retinopathy being prioritized over patients with more severe disease. AI systems also do not recognize other retinal pathologies, such as choroidal lesions, macular degeneration, or glaucoma.
Limitations of teleretinal imaging
Over the past few years, teleretinal screening has increasingly helped improve clinical outcomes as more patients are being screened and referred to specialists for further care. During the COVID-19 pandemic, some clinics in underserved communities were unable to provide patients with their regular visits and monitoring exams.
This emphasized the importance of telemedicine screening for diagnosing and monitoring disease progression. Overall, teleretinal screening has helped improve patient compliance; however, we present two cases highlighting some limitations of teleretinal imaging.
Case 1: Dense medial opacity on wide-field fundus photograph
A 70-year-old male with a history of cataract surgery of the left eye presented to the clinic with complaints of decreased/blurry vision in the left eye. His best-corrected visual acuity was 20/20 OD and 20/40 OS.
Here, the wide-field fundus photo (below) shows fluffy hazy media with indistinct borders and dense medial opacity obscuring visualization of the posterior pole.
Figure 1 shows wide-field Optos fundus photography of the right eye with dense medial opacity.

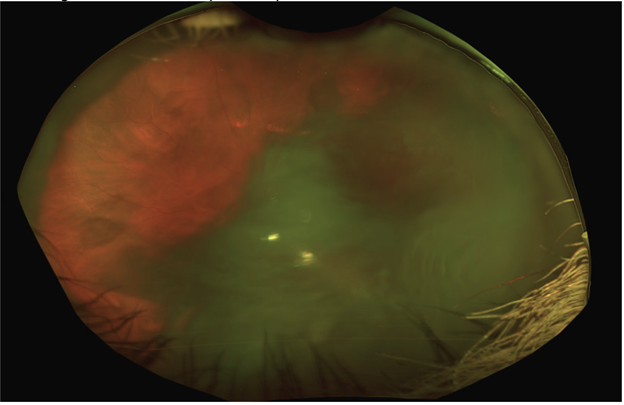
Figure 1: Courtesy of Eric K. Chin, MD.
Upon initial evaluation of the photograph, old chronic vitreous hemorrhage was one of the differential diagnoses, which would prompt intervention. However, on further evaluation, the slit-lamp exam shows a partially and superonasally subluxated intraocular lens (IOL) with moderate posterior capsular opacification and Soemmering’s ring (below), which caused the dense media opacity on fundus photograph. The dilated fundus exam confirmed no vitreous debris or hemorrhage present.
Figure 2 shows a slit lamp photograph of a superonasally subluxated IOL with dense Soemmering’s ring and inferotemporal posterior capsular opacification.

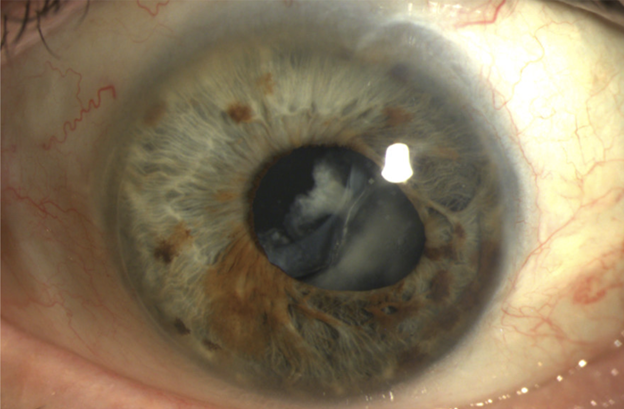
Figure 2: Courtesy of Eric K. Chin, MD.
Case 2: Multiple linear artifacts on wide-field fundus photography
A 75-year-old male with 20/50 vision OU. He is pseudophakic and has a history of epiretinal membrane peel OD, and radial keratotomy (RK) surgery OU. At first glance, this fundus photo is concerning for peripheral retinal pathology. However, this patient had past radial keratotomy OU for myopia, which caused artifacts on the retinal photos.
Figure 3 highlights Optos photograph of the right eye, showing radial whitening and darkening, secondary to corneal scarring from past RK surgery.

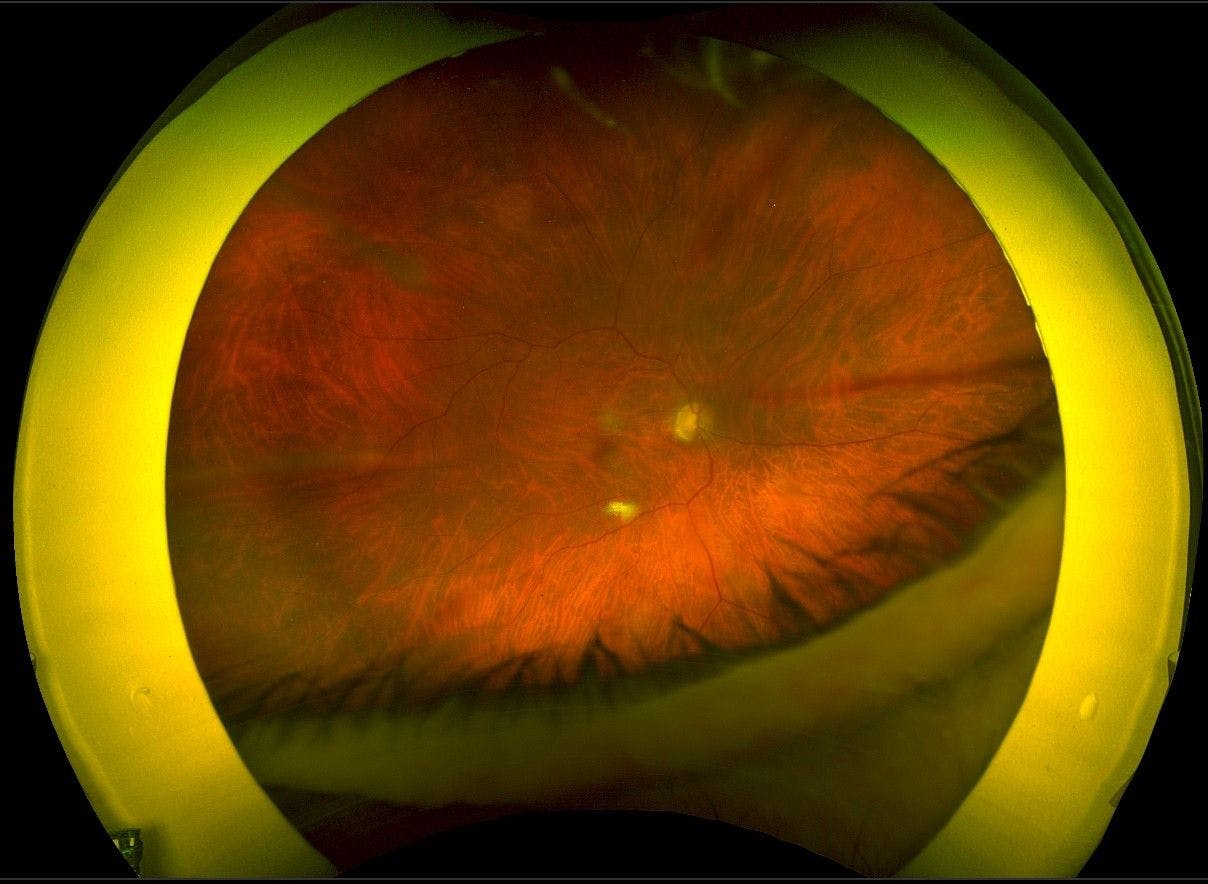
Figure 3: Courtesy of Eric K. Chin, MD.
Understanding the limits of teleretinal imaging
The two cases presented here are examples of pitfalls that may limit the utility of teleretinal imaging. In addition, it is sometimes difficult to precisely measure the retinal surface area to estimate the size and dimension of retinal lesions.
“This can hinder accurate diagnoses and precise treatments for patients.”
Also, as presented above, anterior segment abnormalities can be captured and falsely present concerning retinal findings. Scars from previous procedures like RK can also look like retinal lesions. IOLs with posterior opacification, when displaced, can similarly be misattributed to retinal pathology through the wide-field images.
These pitfalls are important to recognize as they can lead to poor patient care and outcomes. In serious cases, like melanoma, this can lead to metastasis and poor prognosis. It can also lead to unnecessary visits and treatments and overall increased usage of healthcare resources.
In conclusion
Teleretinal screening is a useful tool to provide patients with a less burdensome means of regular retinal exams. Programs have shown their effectiveness in improving screening rates for diabetic patients, especially through their primary care providers. However, the cases we presented above illustrate that teleretinal screening should not be a substitute for regular slit-lamp exams by ophthalmologists.
Rather, teleretinal screening adds a layer of protection to ensure that patients have initial assessments. This can help expedite appointments with retina specialists for moderate-to-severe diseases, and also reduce the patient burden on retina offices from those without the progressive disease who would otherwise only need regular exams.
