


Myopia is the leading cause of visual impairment in children worldwide, prompting numerous studies on risk factors, as well as in control and management.1 Adult myopia onset and progression are not as prevalent as childhood onset and progression, but are contributing to the global burden of disease, and will continue to impact patients and their lives.
Trends in myopia prevalence
In their well-referenced study, Holden et al. predicted that by 2050 worldwide almost 50% of the population will be myopic (refractive correction greater than or equal to -0.50) and almost 10% will have high myopia (refractive correction greater than or equal to -6.00).2 This will be a 46% increase in myopia and a 28% increase in high myopia from levels recorded in 2000.
Figure 1 illustrates the predicted increase in the prevalence of myopia and high myopia between 2000 and 2050.

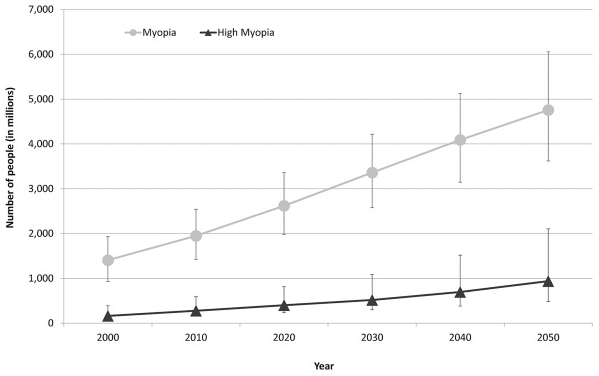
Figure 1: From Holden et al, Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016 May;123(5):1036-42.
While the overall percentage of the population with myopia will grow, there will also be a significant shift in the percentage of people with myopia in adult age groups versus those under 19. This increase in the percentage of the adult population dealing with myopia will impact eyecare providers and healthcare systems worldwide.3
Figure 2 shows the predicted prevalence of myopia in each age group between 2000 and 2050.

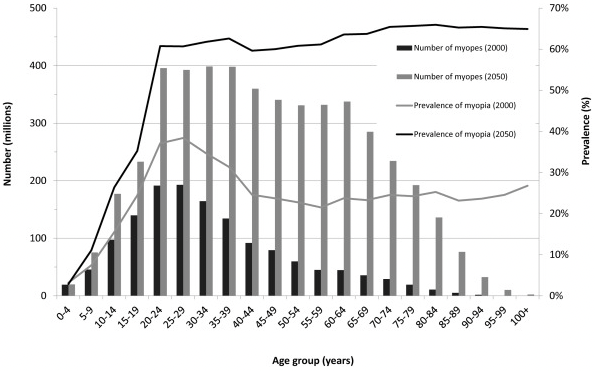
Figure 2: From Holden et al, Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016 May;123(5):1036-42.
Defining the goal of myopia control and management
We often see “myopia control” and “myopia management” used interchangeably. I would say that the compound term “myopia control and management” is most appropriate for describing how eyecare providers approach this condition. Based on the definitions of the two words, this compound term better reflects our goals in treatment choice and the science used to develop treatments.
According to Merriam Webster control, a transitive verb, includes in its definition:
- To exercise restraining or directing influence over; regulate
- To have power over; rule
- To reduce the incidence or severity of, especially to innocuous levels
While management, as the noun describing the act of the transitive verb manage, includes in its definition:
- To handle or direct with a degree of skill
- To work upon or try to alter for a purpose
Our goal in slowing the progression of myopia in patients of all ages is to “reduce the incidence or severity of, especially to innocuous levels” by “directing” treatment “with a degree of skill.” This compound term may also do a better job of conveying to our patients the scope and complexity of creating an individual treatment program for them to protect their ocular health and vision.
A deeper dive: myopia progression versus onset
Adult progressive myopia is defined as any increase in myopic correction over the age of 18, while adult-onset myopia is defined as myopia that presents initially after the age of 18.
In his study on adult-onset myopia, Hans C. Fledelius found that the range of myopia was a little lower in adult-onset versus early-onset (mean values -3.24 and -4.91D, respectively), but high myopia was encountered in both groups (peak values -10 and -10.5D).4
He also found that axial elongation was the main triggering event in both groups, although the suspected stimulus for axial elongation was not noted. Fledelius observed that the eye has the potential for restarting growth years after the presumed normal cessation of ocular growth in late adolescence, contrary to what was previously believed to be true.
It was found in the COMET study that, without any intervention measures, myopia progression stabilizes (change in refraction year over year ≤ ± 0.50D) in almost 50% of childhood-onset myopia patients.5
Figure 3 demonstrates the frequency of myopia progression over time.
Figure 3
For those that do progress, a statistically significant portion goes on to progress between 0.75 and 1D.6
Figure 4 illustrates the stabilization of myopia according to age.