This is a non-sponsored, editorially independent article.
Eyecare is evolving at an exceptional pace. The diagnostic and therapeutic options available have surpassed even the most optimistic expectations from
eyecare practitioners. Advances in managing anterior segment disease have proven fruitful for patients who have had chronic issues.
Eyelid position, although oftentimes an overlooked component of the eye exam, is now critical to assess, because of an easily accessible treatment option.
The treatment for ptosis is primarily surgical, and both patients and physicians have some reluctance about this treatment option; in addition, this treatment is primarily offered by a small subset of physicians, further limiting treatment options for ptosis. Ptosis surgery is an effective treatment option, but, after several years, the benefit may be reduced in some patients, as patients may reacquire ptosis.
As of 2020, we have a pharmaceutical option, Upneeq®, that is available to treat acquired ptosis in adults, expanding the treatment options for patients and physicians alike. Here we will do a deep dive into understanding contemporary treatment options for treating blepharoptosis, including understanding the pathophysiology, discussing both pharmaceutical and surgical options, and helping shape the discussion with patients—along with case presentations to help illustrate the concepts discussed.
Blepharoptosis
Blepharoptosis, or what is more commonly simply referred to as ptosis, is a condition in which the upper eyelid rests at a lower level than is physiologically ideal. The etiology of ptosis stems from a number of underlying issues. Any problems with neurological innervation of the levator muscle, the function of the levator or Mueller's muscle, or aponeurotic changes can cause ptosis.
Ptosis can be caused by a variety of conditions:1,2
- Congenital ptosis is usually the result of either developmental myopathy of the levator muscle or an innervation abnormality.
- Horner’s syndrome is the result of a sympathetic innervation disruption resulting in ptosis with an ipsilateral pupil constriction. This can be caused by either trauma, stroke, or vascular disease.
- Myasthenia gravis is an autoimmune condition that presents with either unilateral or bilateral ptosis which can be associated with diplopia and strabismus.
- A cranial nerve III palsy can present with unilateral ptosis, diplopia, ophthalmoplegia, and a poorly reactive dilated pupil. Cranial nerve III palsies are usually the result of ischemic insult or aneurysm.
- Chronic progressive external ophthalmoplegia is bilateral ptosis accompanied by ophthalmoparesis.
- Aponeurotic changes are stretching or disinsertion of the muscles of the upper lid and is the most common reason for ptosis.
It is important to differentiate ptosis from pseudoptosis. Common conditions that need to be differentiated from ptosis include dermatochalasis, brow ptosis, superior sulcus deformity, microphthalmos, and hemifacial spasm.
The most common cause of pseudoptosis is dermatochalasis caused by excessive tissue on the upper lid creating the appearance of ptosis.1 At times, patients may have both a pseudoptosis and ptosis.
Ptosis can be measured using something called marginal reflex distance -1 (MRD1), which is the distance from the pupillary light reflex to the upper lid margin. Normal MRD1 is usually 4mm or greater.3 As MRD1 decreases, it can impact visual function.
As an example, an MRD1 of 2mm equates to 24-30%
visual field loss. A practical approach to assessing the lid position is to assess its position relative to the portion of the iris superior to the pupil.
Typically, if the lid encroaches on the pupil, it is considered severe. Moderate ptosis is if the lid position is between the upper pupil margin and half the distance from the pupil margin to the top of the vertical visible iris diameter. Mild ptosis is a lid margin that is positioned above this but below the top of the vertical visible iris diameter.
Risk factors that should be considered when evaluating the patient with ptosis include:4-8
Substantial clinical considerations should be taken to understand the impact of ptosis on patients. Many patients have concerns about their appearance and feel that they appear sleepy or tired. There is significant concern from patients who have an asymmetric appearance. Some patients experience anxiety and/or depression because of their appearance.9,10
Functional aspects of ptosis should not be overlooked either. Ptosis can cause blurred vision and an increase in higher-order aberrations creating difficulties performing everyday tasks, such as reading or watching TV.
Additionally, it can cause neck pain, brow aches, headaches, and eyestrain secondary to compensatory mechanisms, such as tipping the head back or attempting to elevate the lids through active recruitment of the frontalis muscle.1,10
Utilizing Upneeq to treat eyelid ptosis
Before Upneeq was approved by the FDA, many physicians would leave ptosis unaddressed unless the patient complained or the condition was causing obvious impairment.10 Many patients assume that if their physician hadn’t addressed the ptosis, it was not severe enough to warrant attention, let alone treatment. Surgery was the only option regarding ptosis.
With the availability of Upneeq, the paradigm has changed and primary eyecare physicians can now be in charge of initiating treatment for acquired ptosis. For patients, it is a value add proposition with their eyecare physician, as this common and distressing condition can be addressed at a regular visit with their physician.
Ptosis typically progresses with time and may cause more distress to patients as time goes on.
Early to middle stages of acquired ptosis typically involve primarily cosmetic concerns, with eyes appearing “bored” or “sleepy.” Sometimes there is an asymmetry between ptosis levels in each eye which can also be cosmetically distressing.
As mentioned earlier, late stages typically bring about more medical symptoms that include:
- Visual impairment
- Eyestrain
- Brow ache
- Neck strain
- Fatigue
Some of these may occur even in earlier stages.
These symptoms can affect patients’ daily living and therefore quality of life. Activities such as watching TV, reading, driving, or fine manual work can become more difficult.
I now also pay much more attention to the possibility of acquired ptosis when I hear about fatigue or eyestrain before offering
lubricant eye drops. Upneeq has become my first-line treatment for acquired ptosis in adult patients who are candidates for the drop.
Because ptosis is a medical diagnosis and clinicians now have a treatment option for it with Upneeq, addressing it may increase the overall complexity of the visit, which may be helpful for documentation and reimbursement.
As ptosis can be a sign of more serious neurological or orbital conditions, the underlying etiology should always be investigated.
I have found that almost all patients are grateful to me for bringing awareness to the issue, explaining their symptoms, and acknowledging their cosmetic concerns. It is common for people to not even realize that they have ptosis, and that it may be a cause of their visual symptoms
Sampling of Upneeq is very important. I think that providing the patient with a sample is important so that both the physician and the patient can see how the treatment worked for the patient. It also is an opportunity for the patient to get an idea if Upneeq is a good treatment option for them prior to committing financially.
It’s important to keep in mind that Upneeq may not be right for all patients. Since Upneeq may impact cardiovascular status, I think physicians should tell patients with cardiovascular disease, orthostatic hypotension, and/or uncontrolled hypertension or hypotension to monitor their condition and call the clinic if it worsens.
My experience is that most patients with these conditions tolerate Upneeq well.
Interestingly, my oculoplastic colleague was concerned that Upneeq would reduce the number of consultations she received. Her consultations have actually increased because of the practice’s and patients’ greater awareness of acquired ptosis—highlighting the importance of that awareness and its benefits for comprehensive eye practices.
My oculoplastic colleague also consults with me on
dry eye patients, and I use Upneeq to test if patients will have an exacerbation of their dry eye with a surgical lid lift.
Let's take a deeper dive into Upneeq.
Who makes Upneeq?
Upneeq is made by RVL Pharmaceuticals, and received FDA approval in July of 2020.
What is Upneeq used for?
Upneeq is used for the treatment of acquired blepharoptosis in adults and is the first and only approved pharmacological treatment for acquired blepharoptosis.
It is dosed as one drop in the affected ptotic eye once daily.11
How does Upneeq work?
Upneeq is oxymetazoline hydrochloride ophthalmic solution 0.1%. Oxymetazoline is a potent alpha-adrenergic receptor agonist and it selectively activates alpha-adrenergic receptors in Muller’s muscle.11-13
How much does Upneeq lift the eyelid?
By activating the alpha-adrenergic receptors in Muller’s muscle, Upneeq raises the ptotic eyelid by 1 to 1.3 mm (in two clinical trials).14 Some patients will get a more dramatic effect than others and may even get some lower eyelid retraction making the eyes appear bigger.
In addition, oxymetazoline has some eye whitening effects that can make eyes appear whiter. However, this is just my observation as eye whitening was not studied in the clinical trials.
How long does Upneeq take to work?
It works as soon as 5 minutes and reaches peak effect at 2 hours post-instillation.
Even by 15 minutes post-instillation, patients will have a significant response. This makes it ideal to do in-office trials with patients, which can be more effective than sampling. Often, patients in consultation with a physician will appreciate the “wow” effect of Upneeq more as pictures and MRD data can be shared with patients.
Does Upneeq improve superior visual field defects?
In two clinical trials, Upneeq significantly improved superior visual field deficits.14
How long does Upneeq last?
Although the response may vary, most patients get about 8 hours of eyelid lift with the use of Upneeq.
Who can prescribe Upneeq?
Upneeq can be prescribed by any eyecare physician and is available either through phone, fax, or e-prescribing directly to the RVL pharmacy in New Jersey. Some physicians may carry Upneeq in their office, and it may be available for patients to purchase from their physician’s office.
What are the common side effects of Upneeq?
I have patients who use Upneeq daily, and even after 1 to 1 1/2 years of usage have not had any significant tachyphylaxis and continue daily use.
I also have some patients who are “weekend warriors'' with Upneeq and use it only on weekends and special engagements. The use is easily customized to individual patient needs and concerns.
The side effects of Upneeq usage are, in general, mild and comparable to the vehicle in clinical trials and are well tolerated.
Side effects include, but are not limited to:
- Instillation site discomfort and irritation
- Headache
- Punctate keratitis
- Dry eye
These were seen in 1-5 % of patients. In the FDA studies, over 95% of patients felt it caused no discomfort.11,15
The other primary treatment for acquired blepharoptosis is surgical with ptosis repair, with or without blepharoplasty. Many patients are reluctant to have surgery or have had surgery in the past on their eyelids and are not anxious to redo the surgery, so Upneeq is a great non-surgical option.
Patient case #1
A 50-year-old Caucasian female presented to the office for her yearly eye exam. She currently wears gas permeable (GP) multifocal lenses to correct both her
myopia and
presbyopia. She is a high myope and her dilated internal ocular exam was unremarkable.
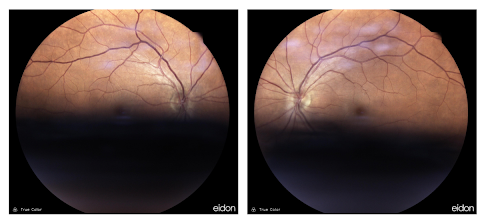
Her fundus photos demonstrated a significant shadow on the lower portion of the picture corresponding to the severe ptosis the patient displayed (Figure 1). It is not uncommon to see ptosis more frequently in an individual wearing GP lenses.
Figure 1 demonstrates demonstrates confocal scanning imaging of a patient with bilateral ptosis.
Figure 1
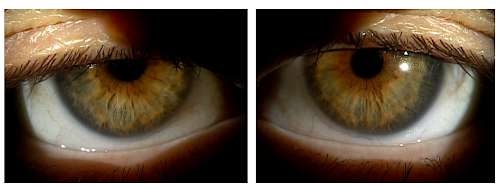
As seen in Figure 2, the patient's upper lid position, at the slit lamp, can easily be seen to be interfering with her vision.
Figure 2
Upneeq was placed in the patient's eyes. Fifteen minutes later, the patient noted a significant difference in the appearance of her upper lid position. She also noted an improvement in her vision.
Fundus photos were then taken after Upneeq and there was significantly improved quality of the pictures with almost a complete absence of the shadow towards the bottom of the picture (Figure 3).
Figure 3 demonstrates confocal scanning imaging of a patient with bilateral ptosis 15 minutes after Upneeq instilled OU.
Figure 3
This case demonstrates both the functional and cosmetic benefits of Upneeq for patients.
Patient case #2
A patient presented who had recently had
cataract surgery with multifocal implant lenses. She was post-op at 1 month 20/25 distance and J1 near and was thrilled with her new eyes and was thrilled with her decreased dependence on glasses.
Upon conversation, she mentioned that, in some dim lighting situations, she felt that she could not read as well. In addition, she mentioned that now she could see the wrinkles on her face and noticed her heavy eyelids.
On external exam, she was noted to have mild dermatochalasis with moderate eyelid ptosis with an MRD of 2.0 mm in both eyes. We discussed options to help her ptosis, including Upneeq. She was excited to try Upneeq, so we agreed to put a drop in her eyes, and she waited in the waiting area for about 15 minutes.
After being brought back into the room, both she and I were impressed with her lid lift, as she appeared to gain 1.5 mm of eyelid lift at 15 minutes. She immediately reported some improvement reading in dim lighting while waiting in the dilating area.
In theory, if heavy lids are blocking the amount of light to the eyes, lifting may help some patients particularly as there is a component of light splitting with
multifocal IOLs. I had taken a picture pre-Upneeq and post-Upneeq, and she was thrilled with her appearance and excited to try Upneeq.
Patient education
It is critical to educate patients on the options available to treat the conditions that they present with. Clinically, this is a two-part process. The first is identifying and educating the patient about their condition. The second is discussing the treatment options and putting a plan in place with the patient.
Prior to the advent of a pharmaceutical agent, Upneeq, being available for treating ptosis, we rarely brought this up to patients unless they asked us about it. Much of the reason we rarely discussed it with patients was the sheer fact that we didn’t have a convenient treatment for patients. The only treatment previously available was surgical intervention.
The availability of a convenient pharmaceutical agent delivered to the eye through a preservative-free eye drop has changed the discussion in a positive way for patients.
When patients initially present to the office, there are several points throughout the exam process where ptosis may be identified. These include:
- Difficulty acquiring auto-refraction measurements because of lid position
- Difficulty with superior visual field on screening
- Shadows noted either superiorly or inferiorly on fundus photos (depending on the type of fundus camera, see Figure 1)
- The patient's head tilts backward
- Asymmetry in the eyelid position between the two eyes
- Eyelid position during slit lamp examination
- Difficulty with internal ocular assessment, secondary to ptosis
Additionally, some patients will present to the office with a chief complaint of ptosis. This may be a direct complaint such as, “I have droopy lids. Is there any treatment for it?”
Often patients will present with other complaints. They may have gotten used to the appearance of their upper lids so will complain of symptoms consistent with ptosis without direct complaints of their eyelid position. Some will come in complaining of neck issues.
This is often a complaint that accompanies patients utilizing
traditional progressive addition lenses, as opposed to a computer lens design that allows them to utilize intermediate ophthalmic correction in the lens without tilting their head back. For the patient with ptosis, it may be a compensatory head tilt back to ease the burden of seeing below the low lying, ptotic lid.
Since patients may develop compensatory habits, that create the kind of symptoms mentioned earlier, it is critical to pay particular attention to these more subtle complaints that may be secondary to ptosis.
Proactively bringing up the discussion with patients may be a difficult one for clinicians to have because of the cosmetic component that low-lying eyelids can have. Beginning this conversation early can help prevent many of the psychological and functional concerns that these patients may manifest. As such, it is critical to begin these discussions early with patients and provide them with appropriate treatment options.
Although there is no single best way to educate patients about ptosis, we’ve found that customizing the approach to the clinical findings often will provide the patient with the information that they need to make the most appropriate decisions for their eye health needs.
A few examples are the patient with visible eyelid asymmetry. For those individuals, a simple question such as, “Do you ever feel like there is a difference with your eyelid height between the two eyes?” will often begin the discussion around the patient’s unilateral ptosis. These patients are rarely aware that a pharmaceutical treatment for ptosis exists and are happy to discuss this treatment option.
Another example is a patient who has had fundus photos and is demonstrating a shadow at the bottom of the picture (corresponding to something blocking light from entering the superior pupil). For these patients, we ask, “Do you ever feel your eyelids get in the way of your vision?” or “Do your eyelids feel heavier as the day goes on?” This begins a functional discussion about the pharmaceutical option available to treat ptosis.
Another interesting clinical finding is that some patients will have a mental hurdle connecting the fact that an eye drop can increase the position of their upper eyelids. Some have thought that they would need to somehow rub it on their lids for the lids to elevate. An appropriate explanation and demonstration that clearly shows that a drop on the ocular surface will elevate the lids are critical for patient understanding and patient success.
Conclusion
Advances in eyecare have provided us with exceptional technologies to manage ocular conditions. Blepharoptosis can now be pharmaceutically managed with Upneeq which is intended to be utilized once a day.
Understanding the pathophysiology and appropriate differential diagnosis is critical to appropriately identify this condition. Taking into consideration the functional and potential psychological aspects of the condition helps us clinically realize the importance of identifying these patients. Appropriate strategies to help with discussing the condition and treatment options are critical.
We are at a time when we have an effective pharmaceutical treatment for patients with ptosis. Appropriately prescribing for these patients will provide the necessary relief these individuals need with a non-surgical option. It is critical to keep all of this in consideration when providing appropriate treatment for these patients.
The views expressed in this independent article belong to the authors and not Eyes On Eyecare. While we make every effort to provide accurate information that is helpful to your eyecare practice, this information may contain errors and is not to be used in place of your own professional medical judgment. Under no circumstances shall the authors or Eyes On Eyecare be responsible for damages arising from use of this information.
References
- Josef Finsterer. Ptosis: causes, presentation, and management. Aesthetic Plast Surg. May-Jun 2003;27(3):193-204.
- Custer PL. Blepharoptosis. In: Yanoff M, Duker JS, eds. Ophthalmology. 3rd ed. St Louis, United States: Elsevier; 2008
- Reinhard E, et al. The OD’s Guide to Ptosis Workup. Review of Optometry. April 15, 2020: 68-73.
- Forman WM, et al. A community survey of ptosis of the eyelid and pupil size of elderly people. Age Ageing. 1995;24:21-24
- Hashemi H, et al. The prevalence of ptosis in an Iranian adult population. J Curr Ophthalmol. 2016;28:142-145
- Kim MH, et al. Prevalence and associated factors of blepharoptosis in Korean adult population: The Korea National Health and Nutrition Examination Survey 2008–2011. Eye (Lond). 2017;31:940-946.
- Wang Y, et al. Incidence and risk of ptosis following ocular surgery: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2019;257:397-404.
- Steinsapir KD, et al. Blepharoptosis treatment as a complication due to botulinum toxin application. Dermatol Surg. 2015;41:833-840. 10.
- Richards HS, et al. The psychological well-being and appearance concerns of patients presenting with ptosis. Eye. 2014;28:296-302
- Bacharach J, et al. A review of acquired blepharoptosis: prevalence, diagnosis, and current treatment options. Eye. 2021;35:2468-2481
- Upneeq® (oxymetazoline hydrochloride ophthalmic solution), 0.1%. [Prescribing Information]. RVL Pharmaceuticals, Inc. 2020
- Esmaeli-Gutstein B, Hewlett B, Pashby R, Oestreicher J, Harvey J. Distribution of adrenergic receptor subtypes in the retractor muscles of the upper eyelid. Ophthalmic Plast Reconstr Surg. 1999;15(2):92–99.
- Haenisch B, Walstab J, Herberhold S, et al. Alpha-adrenoceptor agonistic activity of oxymetazoline and xylometazoline. Fundam Clin Pharmacol. 2010;24(6):729-739.
- Slonim CB, Foster S, Jaros M, et al. Association of oxymetazoline hydrochloride, 0.1%, solution administration with visual field in acquired ptosis: a pooled analysis of 2 randomized clinical trials. JAMA Ophthalmol. 2020;138(11):1168-1175.
- Wirta DL, Korenfeld MS, Foster S, Smyth-Medina R, Bacharach J, Kannarr SR, Jaros MJ, Slonim CB. Safety of once-daily oxymetazoline HCl ophthalmic solution, 0.1% in patients with acquired blepharoptosis: results from four randomized, double-masked clinical trials. Clin Ophthalmol. 2021;15:4035-4048