



Myopia, already the most common worldwide ocular disease, has a prevalence that is expected to increase dramatically in the next 30 years.1 Ocular morbidity from myopia is expected to significantly impact ophthalmology over the coming decades and the challenges to management and effective prevention strategies need to be addressed in order to minimize myopia morbidity. Here, we present an update on the prevalence, risk factors, pathology and prevention of myopia.
The growing myopia problem
Myopia is the leading worldwide cause of visual impairment in children.1 In myopia, the spherical equivalent objective refractive error is less than or equal to –0.50 diopters in either eye. High myopia, representing advanced pathology and worse prognosis, is defined as a spherical equivalent objective refractive error of less than or equal to –5.00 diopters in either eye.
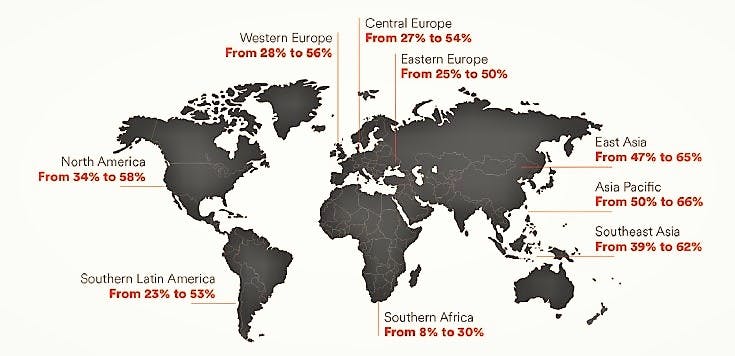
In 2010, an estimated 1.9 billion people (27% of the world’s population) were myopic; of these, 70 million (2.8%) had high myopia.2 Myopia prevalence worldwide was 22% in 2000 and this is expected to grow to 52% by the year 2050 (Figure 1).3 With respect to high myopia, and its increased disease severity, worldwide prevalence was 2.2% in 2000 but is expected to grow nearly five times, to 10%, by the year 2050.3 Eye physicians need to be aware of the myopic disease burden given the expected increasing prevalence.
Figure 1, below, illustrates he current and projected prevalence of myopia by worldwide region.3

Myopia etiology and myopigenic behaviors
Although the exact mechanism of myopia pathology—ocular axial length elongation—is unknown, recent research continues to emphasize the major role of environmental factors while attributing a minor role to genetics.4 The Consortium for Refractive Error and Myopia (CREAM), the largest international genome-wide study of myopia and refractive error ever conducted, identified 24 genomic variations associated with a 10-fold increase in myopia prevalence suggesting a multifactorial pathophysiologic basis for myopia.5
Moreover, the projected increase in myopia and high myopia worldwide by 2050 is too rapid to be explained by genetics alone.
The primary risk factors for myopia are related to the myopigenic behaviors of time indoors and schooling.6 The current global novel coronavirus pandemic, which has led to increased digital screen time, near work and limited outdoor activities secondary to lockdown measures for infection control, has been shown to be associated with the onset and progression of myopia.7 Contrastingly, outdoor time—irrespective of activity engagement —has been shown to reduce the prevalence of myopia suggesting light exposure as a major protective factor in myopia prevention.8
Clinical features and complications of myopia
It is critical to emphasize myopia is not a benign or stationary condition. Once established, the condition progresses with increasing refractive error. Pathologic myopia occurs when there is posterior segment pathology from axial elongation and is found in 1-3% of Asians and 1% of whites.3 Myopia progression is the primary cause of blindness and low vision in 12-27% of Asian populations and 7% of those of European descent.3
Myopia-related vision loss can be attributed to multiple pathologic entities. Macular choroidal neovascularization (CNV) is one of the most frequent complications that leads to loss of central vision in patients with pathologic myopia. Myopic CNV develops in 10% of highly myopic patients; additionally, 30% of myopic patients who have a CNV in one eye eventually develop CNV in the other eye.6 While myopic CNV is not intensely active and has a tendency to regress spontaneously, progression from an active exudative phase to macular scarring is common and results in irreversible loss of central vision. Consequently, the prognosis of myopic CNV is poor.
Natural history studies show that, at onset of myopic macular CNV, 70% of patients have a visual acuity better than 20/200; however, at 5 and 10 years after onset, visual acuity decreases to 20/200 or less in 89% and 96% of patients, respectively.9
“The need for early recognition and treatment is imperative.”
The preferred treatment for myopic macular CNV consists of intravitreal vascular endothelial growth factor (VEGF) inhibitors, with 40% of patients experiencing significant visual improvement of three lines or more at one year follow-up. Although myopic CNV recurs, typically within 6 months of initial treatment, the number of anti-VEGF injections ranges from 2.4 to 4.9 annually.9
The risk of developing a retinal detachment is approximately five to six times greater in people with high myopia compared to those with low myopia.10,11 Given the increased likelihood of retinal breaks and detachment in myopic eyes, ophthalmologists and retinal specialists need to be proficient in examination of the peripheral retina. Ophthalmologists in general need to be cognizant of the sequelae of myopia and to be aware of the need for prompt referral of cases of myopia given the elevated risk of retinal detachment.
Preventing myopic progression
The 2017 American Academy of Ophthalmology (AAO) Myopia Report states, “Level I evidence supports the use of atropine to prevent myopic progression. Although there are reports of myopic rebound after treatment is discontinued, this seems to be minimized by using low doses (especially atropine 0.01%).”12 The first clinical trial of atropine for myopia was published in 1979 and involved 1% atropine in 62 children.13
The results showed treated eyes had reduced or stable myopia; this provided the initial rationale for using atropinization to impede myopic progression. Atropine, a muscarinic receptor antagonist at the ciliary muscle, prevents accommodation. Although atropine’s mechanism of action remains not fully understood, evidence suggests atropine prevents myopia in humans and animal studies.14
Although debate continues on whether atropine is a viable and safe real-world option, the available evidence and the AAO Myopia Report indicate that treating myopia progression with atropine is promising. Additional studies are needed to better elucidate the mechanism of action and the ideal dosing paradigms to best stymie the growing myopia disease burden.
In terms of environment and myopia prevention, children should be encouraged to spend more time outside and less time on screens. Given that schooling is associated with increased myopia, policymakers need to address opportunities to mitigate risk factors that lead to myopic progression during school years. Eye physicians are best suited to serve as patient advocates to address these issues.
Raising awareness among parents, children, and government agencies is key to mitigating myopigenic behaviors that may become entrenched during this period.
Conclusions
Eyecare professionals, from optometrists and ocularists to ophthalmologists, need to be aware of myopia risk factors in order to provide their patients with appropriate counseling and disease awareness. Given the potential disease burden of myopia in the decades ahead, policymakers, too, need to be made aware of the risk factors. Although cautious optimism with respect to treatment of the underlying pathogenesis of myopia, as well of its complications is encouraging, emphasis on prevention continues to best serve patients at this time.
References
- World Health Organization, “Impact of Increasing Prevalence of Myopia and High Myopia the Impact of Myopia and High Myopia,” 2015.
- Fricke TR, Jong M, Naidoo KS, Sankaridurg P, Naduvilath TJ, Ho SM, Wong TY, Resnikoff S. Global prevalence of visual impairment associated with myopic macular degeneration and temporal trends from 2000 through 2050: systematic review, meta-analysis and modelling. Br J Ophthalmol. 2018 Jul;102(7):855-862.
- Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, Wong TY, Naduvilath TJ, Resnikoff S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016 May;123(5):1036-42.
- Morgan IG, French AN, Ashby RS, Guo X, Ding X, He M, Rose KA. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res. 2018 Jan;62:134-149.
- Carr BJ, Stell WK. The science behind myopia. In: Kolb H, Nelson R, Fernandez E, Jones B, eds. Webvision: The Organization of the Retina and Visual System. University of Utah Health Sciences Center. https://webvision.med.utah.edu/book/part-xvii-refractive-errors/the-science-behind-myopia-by-brittany-j-carr-and-william-k-stell. Accessed 13 February 2021.
- Dolgin E. The myopia boom. Nature. 2015 Mar 19;519(7543):276-8.
- Wong CW, Tsai A, Jonas JB, Ohno-Matsui K, Chen J, Ang M, Ting DSW. Digital Screen Time During the COVID-19 Pandemic: Risk for a Further Myopia Boom? Am J Ophthalmol. 2020 Jul 30;223:333-337.
- Rose KA, Morgan IG, Ip J, Kifley A, Huynh S, Smith W, Mitchell P. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008 Aug;115(8):1279-85.
- Ryan's Retina (6th Edition). Editors: SriniVas Sadda. Elsevier 2017.
- Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012 Nov;31(6):622-60.
- Ohno-Matsui K, Lai TY, Lai CC, Cheung CM. Updates of pathologic myopia. Prog Retin Eye Res. 2016 May;52:156-87.
- Pineles SL, Kraker RT, VanderVeen DK, Hutchinson AK, Galvin JA, Wilson LB, Lambert SR. Atropine for the Prevention of Myopia Progression in Children: A Report by the American Academy of Ophthalmology. Ophthalmology. 2017 Dec;124(12):1857-1866.
- Bedrossian RH. The effect of atropine on myopia. Ophthalmology. 1979 May;86(5):713-9.
- McBrien NA, Stell WK, Carr B. How does atropine exert its anti-myopia effects? Ophthalmic Physiol Opt. 2013 May;33(3):373-8.
