Continuous positive airway pressure (CPAP) devices are used in treatment of sleep apnea and allow patients to obtain a steady stream of air while they sleep.
1 Since sleep apnea is linked to cardiovascular disease, these devices can improve both sleep quality and overall
general health in patients suffering from sleep apnea.
It has become common for patients to complain of dry eye symptoms during or after use of a CPAP device since the airflow can leak or divert in the direction of the patient’s eyes. This article will present the possible complaints and exam findings associated with CPAP-induced dry eye syndrome and discussion points for you to cover with your patient. It will then present treatment and management options for you to better assist patients experiencing this issue.
What the research says
A 2020 study published in the Journal of Clinical Ophthalmology investigated the prevalence of
dry eye disease (DED) in the general population versus CPAP users. The results demonstrated that there was substantially more DED present in the latter than their non-CPAP using counterparts. Furthermore, the greater length of time the subject used a CPAP device (3 years versus 1 year, for example) the more likely they were to experience symptoms of DED.
A 2012 study in Cornea investigated the ocular surface integrity of subjects using CPAP devices by monitoring Shirmer testing, tear break up, corneal staining, and conjunctival impression cytology. These tests were performed at baseline and then repeated after the subject had been using a CPAP device for 4 months.
The results of this study showed demonstrable increase in evaporative dry eye and subjective ocular irritation. The study suggests the deterioration is attributed to changes in sleep position moving the mask or general mask displacement over the course of the night.3
A 2007 article in Optometry warned that eyecare providers need to know if patients are using CPAP devices because there is potential, albeit rare, for severe corneal compromise in some patients. The paper discussed a keratoconus patient who began using CPAP and subsequently developed limbal keratitis, a patient with pellucid degeneration who developed
chronic conjunctivitis and even a healthy patient who developed a
corneal ulcer attributed to onset of CPAP device use.
The authors suspect that bacteria trapped under the mask was being pushed onto the ocular surface by the airway pressure instigating these infectious conditions.4
Common signs and symptoms
Patients may complain of the typical ocular surface disease symptoms:
- Redness
- Burning
- Tearing
- Foreign body sensation
- Intermittent blurred vision
- Temporary light sensitivity.1
The key factor here is that the symptoms will be much worse during the night and in the morning (corresponding to use of the CPAP device). The second key factor, which may seem obvious, is that the symptoms will have started at the same time as or slightly after the patient started using the CPAP device.
If this condition is suspected, it would be ideal to evaluate the patient at a morning appointment when symptoms and signs are most prominent.
Dry eye testing such as tear breakup time and Shirmer testing would likely demonstrate an evaporative mechanism since the excess air flow is causing a faster-than-normal tear film evaporation process.
Additional factors may coexist with the DED-related ocular surface condition such as concurrent
meibomian gland dysfunction or aqueous deficiency - which should also be evaluated. Other ocular issues such as floppy eyelid syndrome or incomplete lid closure can also be exacerbated by the use of a CPAP device. Systemic inflammatory conditions can also make patients more susceptible to ocular surface disruption with a CPAP device.
Essentially, all factors potentially impacting ocular surface integrity should be evaluated to determine if the culprit is the CPAP device alone or its effects are in conjunction with other sources or underlying conditions.
Treatment and recommendations
CPAP devices come in several forms ranging from full face coverage to mouth/nose coverage to nose-only coverage. Which device is prescribed will be determined by the patient and his/her sleep doctor based on the condition and their comfort level. Patients should check their mask for any areas of leakage, especially around the nasal bridge that provides a route of airflow toward the eyes.
If major leaks are present the patient should return to their specialist for a refit or to add a nose pad that stabilizes the mask position.
The level of air pressure may also be adjusted; this is something the patient can discuss with their prescribing physician to find a balance of comfortable air flow while avoiding excessive air leakage. There are also options such as a “nasal pillow” device that is small and covers the nostrils only which tends to have a tighter fit or an oral device (a type of custom retainer) that may be indicated instead of the traditional mask.5
If the patient has achieved the best-fit possible for their CPAP device and is still showing related signs and symptoms, there are still measures they can take.
1) Ensuring adequate ocular lubrication and coverage is the next step—especially overnight. Higher viscosity artificial tears (gel drops) or lubricant ointments are the ideal option for overnight protection.
2) Environment can also play a role; patients should be cognizant to avoid additional air flow sources too nearby while they are sleeping such as air conditioners, air vents, or fans.
3) Lastly, patients should be completing proper mask hygiene by cleaning it regularly since oil buildup from skin can make the mask more likely to slip out of position.1
Patient case
A 34-year-old male presented for his comprehensive exam complaining of tearing in the left eye greater than the right. It occurred only in the mornings and was not associated with any redness, burning, itching or other symptoms. He felt he was constantly wiping tears from his eyes in the morning and was embarrassed by this at work; it had been ongoing for a few weeks.
Medical history was unremarkable aside from a history of mild sleep apnea. Ocular history was remarkable for a foreign body injury of the left eye several years ago that did not leave any scarring or visually significant sequelae. Uncorrected vision was 20/20 in both the right and left eye. On an anterior segment slit lamp exam, a very faint inferior superficial keratitis was present in both eyes and tear break up time was reduced at 4 seconds in the right eye and 3 in the left; all other exam testing was normal.
On further discussion of the patient’s daily routine, especially sleep habits, since morning symptoms were occurring, I learned he started using a CPAP nose-only mask for treatment of mild sleep apnea a few months prior, as seen in Figure 1.
Figure 1
I mentioned the possibility of the sleep mask leaking air causing his eyes to dry out overnight. I suggested he check the fit and be cognizant of the mask’s position upon waking. I prescribed the patient
Refresh Celluvisc® gel eye drops, two drops in each eye before bed and
Refresh Classic® as needed in the morning and afternoon. I asked him to follow up in a few weeks for a re-evaluation.
A month later, his condition had improved. The lubricant drops had made him much more comfortable and prevented most of the tearing. He did say that occasionally when he woke up the mask was out of place and on those occasions, he did have more tearing on “the side where the air was leaking out.”
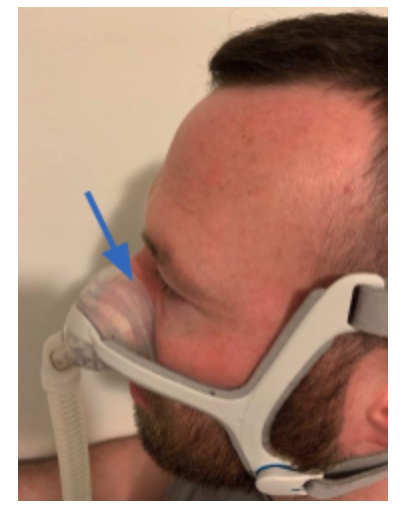
Figure 2 illustrates with an arrow the common culprit of CPAP air leakage: poor enclosure around the nasal bridge.
Figure 2
After noticing this and understanding the relationship between the device and his eye condition, the patient had also followed up with his sleep specialist to make sure this was the best treatment option. It turned out a newer type of device, a “nasal pillow,” was prescribed to replace it.
As seen in Figure 3, the new device was much smaller with two nozzles that entered the nostrils and stayed in place more reliably.
Figure 3
He rarely needed the lubricant eye drops at this point. He said only once he “woke up with the air nozzle pointed straight in my eyes” within the first few days of switching but has learned to secure it better since then. On those rare occasions he did experience a flare up of symptoms, the lubricant drops did the trick.
Conclusion
This case was a great example of how awareness and a simple discussion can bring CPAP-induced dry eye to light. Explaining the correlation between the two, addressing the ocular surface implications and managing discomfort can make a big difference for patients dealing with sleep apnea. By managing these secondary sequelae of CPAP devices, our patients won’t need to trade a poor night’s sleep for ocular surface disease any longer.
References
- Repasky, D. (2021, August 5). Dry eyes with CPAP? (reasons, causes, and solutions). CPAP.com Blog. Retrieved December 28, 2021, from https://www.cpap.com/blog/dry-eyes-cpap-reasons-causes-solutions/
- Matossian C;Song X;Chopra I;Sainski-Nguyen A;Ogundele A; (n.d.). The prevalence and incidence of dry eye disease among patients using continuous positive airway pressure or other nasal mask therapy devices to treat sleep apnea. Clinical ophthalmology (Auckland, N.Z.). Retrieved December 28, 2021, from https://pubmed.ncbi.nlm.nih.gov/33116388/
- Hayirci, E., Yagci, A., Palamar, M., Basoglu, O. K., & Veral, A. (2012, June). The effect of continuous positive airway pressure treatment for obstructive sleep apnea syndrome on the ocular surface. Cornea. Retrieved December 28, 2021, from https://www.ncbi.nlm.nih.gov/pubmed/22410644
- S;, H. W. P. N. K. Anterior segment complications secondary to continuous positive airway pressure machine treatment in patients with obstructive sleep apnea. Optometry (St. Louis, Mo.). Retrieved December 28, 2021, from https://pubmed.ncbi.nlm.nih.gov/17601573/
- Tamara K SellmanJune 28, 2021, Matt Gentry Moderator July 6, 2021, & Tamara K Sellman Moderator July 18, 2021. (n.d.). Might CPAP therapy contribute to dry eye disease? SleepApnea.Sleep. Retrieved December 28, 2021, from https://sleepapnea.sleep-disorders.net/living/cpap-dry-eye-disease