


Optical coherence tomography (OCT) is a non-invasive diagnostic imaging tool that is becoming an essential part of any optometric practice. OCT captures ultrasound images to produce cross‐sectional detailed images at the microstructure level of the retina, including the macula.1
The most common macular scan protocols include raster, radial, and three‐dimensional (3D) scans (Figure 1.) The raster scans are parallel line scans that are of higher resolution. The radial scan is made up of 6-12 line scans arranged in equal angles with a common axis. And 3D scans consist of horizontal line scans that generate a 3D view of the image which enables morphology, thickness, and mapping analysis of the macula.1
In this article, we’ll be discussing clinical indications and common uses for OCT imaging in clinical practice, specifically as it pertains to macular pathology.
Figure 1 of common macular OCT scans: A-Raster scan, B-Radial scan, and C-3D scan.

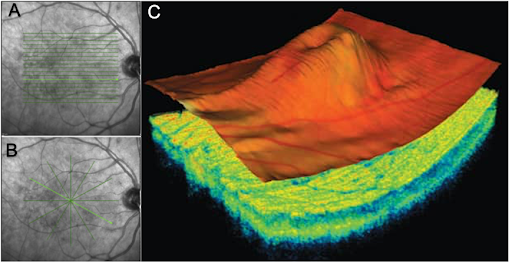
Figure 1

Download the Guide to Common Macula Findings with OCT
This easy-to-follow guide breaks down OCT findings, follow up, and treatment.

Macular hole
A macular hole is a separation of retinal tissue within the macula. It can be caused by aging, trauma, vitreomacular traction (VMT), or cystoid macular edema (CME). (2) Full-thickness holes involve all retinal layers to the retinal pigment epithelium (RPE), while lamellar holes only involve the inner macular layers and the photoreceptor layer is still intact.2
Patients with an imminent hole will often have minor visual symptoms and may experience metamorphopsia. Vision can range between 20/50 to 20/800 with full-thickness holes.2
The four stages of macular holes according to the Gass Classification system include:3
- Stage 1 - cystic foveal change indicating foveal detachment, vitreous attached at the fovea.
- Stage 2 - 100-300 micron full-thickness retinal defect with possible pseudo-operculum.
- Stage 3 - >400 micron full-thickness retinal defect with a persistent hyaloid attachment. No Weiss ring present. Positive Watzke’s sign is present.
- Stage 4 - stage 3 with complete posterior vitreous detachment (PVD)and Weiss ring present.
Observation of stage 1 holes is often appropriate due to these spontaneously resolving in 50% of cases. If there is progression beyond stage 1, referral for vitrectomy, epiretinal membrane peel, and/or fluid-gas exchange procedures should be considered.3
Figure 2 illustrates the four stages (A-D) of macular hole.

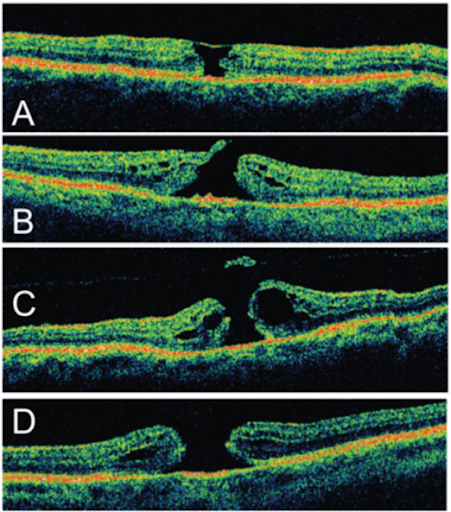
Figure 2
Dry age-related macular degeneration
Dry age-related macular degeneration (AMD) begins with drusen, which are yellow subretinal pigment epithelial deposits in the macula (Figure 3). The risk of developing visual symptoms is higher when there are several, large drusen, and the drusen is associated with increased RPE disruptions.
Advanced dry AMD can develop into central geographic atrophy where vision loss is caused from RPE degeneration and loss of photoreceptors in the macula.4,5
AMD risk factors include:4,5
- Advanced age
- Family history
- Smoking
- High cholesterol
- Fat intake
- Abdominal obesity
- Ultraviolet light exposure
Figure 3 demonstrates dry AMD (top image) and exudative AMD (bottom image).

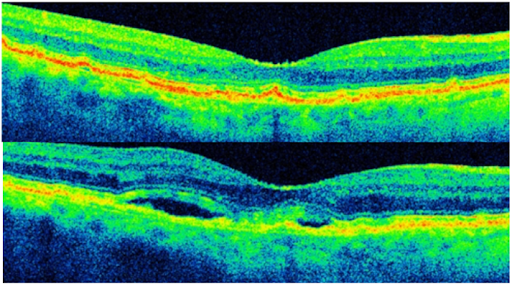
Figure 3
Dry AMD can be managed with appropriate education of risk factors, vitamins, and regular follow-up exams with OCT and dilated fundus exams.4,5
Exudative age-related macular degeneration
Exudative AMD causes vision loss due to abnormal blood vessel growth in the choriocapillaris that breaks through Bruch's membrane. The proliferation of abnormal blood vessels in the retina is stimulated by increased levels of vascular endothelial growth factor (VEGF).4,5
The new vessels are fragile, often leading to blood and protein leakage below the macula. This causes hemorrhagic pigment epithelial detachments (PEDs) when observed on OCT (Figure 3).6 These unstable blood vessels can cause irreversible damage to the photoreceptors and vision loss if left untreated.4,5
Patients should be referred to a retinal specialist as soon as possible for treatment options, such as anti-VEGF ocular injections and/or photodynamic therapy (PDT) whenever exudative AMD is suspected.4,5
Cystoid macular edema
CME is the accumulation of fluid in the outer plexiform layer with possible intraretinal cysts secondary to irregular perifoveal capillary permeability (Figure 4).7 Patients can present with symptoms of reduced central vision, monocular diplopia, and/or metamorphopsia.
Figure 4 illustrates CME.

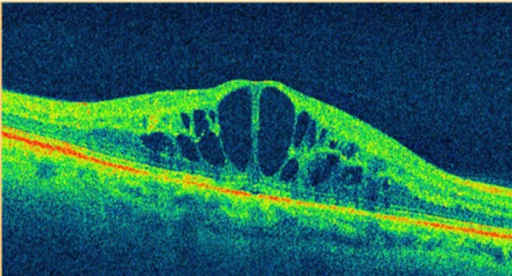
Figure 4
Common causes for CME include:7
- Diabetes
- Ocular inflammation
- Retinitis pigmentosa
- Irvine-Gass syndrome
- Retinal Venous occlusion
- Retinal detachment
- Sarcoid
Since many factors can cause CME, effective treatments will vary depending on the severity and the cause of the condition.7
Epiretinal membrane
Epiretinal membranes (ERM) are often idiopathic and can be seen in patients with no previous medical history or visual complications. They can be associated with PVDs, prior retinal tears or retinal detachments, retinal vascular diseases, intraocular inflammation, and trauma.8
ERMs are mild to severe distortions of the natural macular architecture. They can occur from changes in the vitreous that cause glial cells to multiply between the posterior vitreous and the internal limiting membrane of the retina.8
A mild ERM will present with increased wrinkling, and distortion of retinal capillaries, and possibly with mild metamorphopsia. Vision is often 20/40 or better. Mild ERMs can be monitored as long as vision is not significantly affected. In more advanced cases, a macular pucker shows severe distortion of the retinal vessels and a retinal appearance of wrinkling with possible intraretinal thickening and edema (Figure 5).8
If follow-up care shows progression or worsening in functional vision, a referral for vitrectomy and/or membrane peel may be recommended.8
Figure 5 illustrates macular pucker.

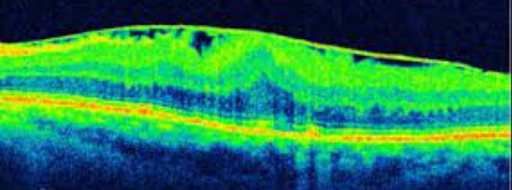
Figure 5
Vitreomacular traction
VMT is commonly caused by age-related degeneration of the vitreous humor. Other risk factors include high myopes, women with declining post-menopausal estrogen levels, exudative AMD, diabetic retinopathy, and retinal vein occlusions.8
In age-related vitreous changes, fluid pockets form within the vitreous causing loss of volume and eventual vitreous contraction. The vitreous interface subsequently weakens and can detach, commonly causing a PVD. Vitreous detachments that are incomplete at the macula cause vitreomacular adhesions, and these adhesions can progress to VMT.9
All the following must appear on OCT for classification of a VMT:9
- Perifoveal vitreous detachment from the retina.
- Macular attachment of the vitreous interface within a 3‐mm radius of the fovea.
- Distortion of the foveal surface and/or intraretinal structural changes, but no full‐thickness disruption along all retinal layers.
Figure 6 represents vitreomacular traction.

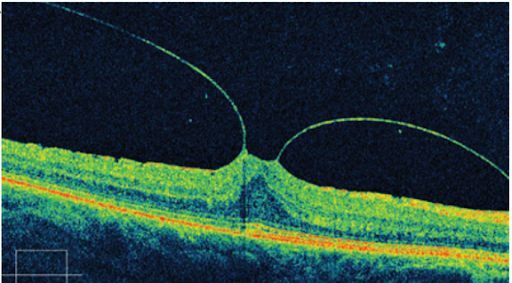
Figure 6
Since the progression of VMT is variable, regular monitoring with OCT is necessary. VMT can progress quickly, affecting visual function, and sometimes can resolve spontaneously. Significant VMT can cause an increased risk of a full thickness macular hole.9 For the patients whose visual symptoms and signs are severe, referral to a retinal specialist is advised.
Treatment for VMT can include vitrectomy and/or ocriplasmin intravitreal injections which cause protein fibers attaching the vitreous to the macula to dissolve.9
Central serous retinopathy
Central serous retinopathy (CSR) occurs when fluid accumulates under the retina, causing an increase of subretinal fluid and a macular serous detachment that commonly leads to reduced vision (Figure 7).10 This macular condition is typically seen in type-A males that report blurring or distortions of their central vision.10
Figure 7 displays CSR.

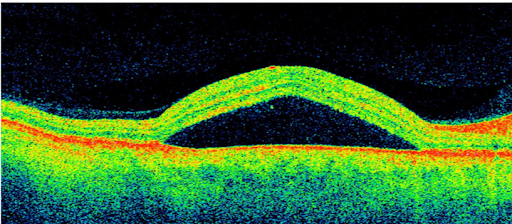
Figure 7
CSR has been associated with systemic exposure to corticosteroids and in patients that are frequently in emotional distress due to the body’s increased production of natural corticosteroids.10 Corticosteroids are thought to alter RPE and choroidal circulation by causing the RPE pump to malfunction or increase the vascular permeability of the choroid.9
Other risk factors include having a relative that has been previously diagnosed with CSR and patients with high blood pressure and heart disease.10
CSR is generally a self-limiting retinal condition and visual recovery often occurs within a few weeks to 6 months without treatment.10 Management includes regular monitoring and patients taking corticosteroids should be advised to discontinue their use if safe to do so.10 If the CSR becomes chronic, depending on the severity of the patient’s symptoms, referral may be the best option where several therapies, such as oral medications, laser treatments, and ocular injections can be offered.10
Hydroxychloroquine retinopathy
Administration of hydroxychloroquine (Plaquenil) is commonly used in treating numerous autoimmune diseases. Patients experiencing the early stages of hydroxychloroquine retinal toxicity commonly do not experience any visual symptoms. Subtle visual symptoms can include difficulty adjusting to darkness, reduced vision, and atypical color vision. Most patients usually notice symptoms only after paracentral scotomas have become severe.11
On examination, the RPE of the macula that gives the appearance of a “bull’s-eye” is considered a late finding, and early toxicity can show no visible signs, though bilateral visual field and OCT changes may be detected.11 OCT findings can show disruption of the outer ellipsoid zone, perifoveal thinning of the outer nuclear layer, and the typical “flying saucer sign” that is created by the intact outer retinal layers within the central foveal, surrounded by perifoveal loss of the ellipsoid zone and outer nuclear layer degeneration (Figure 8).11
Figure 8 illustrates a “flying saucer” observed on OCT in late-stage hydroxychloroquine-induced maculopathy.

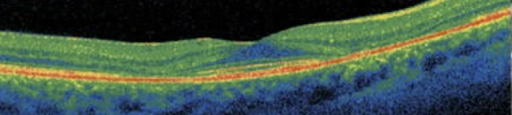
Figure 8
Hydroxychloroquine-induced retinal toxicity risk factors include:11
- Daily dose greater than 400mg, or a daily dosage over 6.5 mg/kg ideal body weight, or total cumulative dose of more than 1,000g.
- Over 5 years of medication use.
- Renal or liver disease.
- Underlying maculopathy.
During regular monitoring, if hydroxychloroquine-induced retinal toxicity is suspected and confirmed with reproducible findings, it is critical to inform these findings to the patient's prescribing physician so the medication can be discontinued, unless it is medically critical and the patient has been informed of the visual risks.11
Don't forget to download the Common Macula Findings Cheat Sheet!
Conclusion
As eye care providers, it is critical to become comfortable with diagnosing and managing these common macular conditions. Accurate interpretation of OCT findings improves the clinician’s ability to convey accurate information to patients regarding their diagnosis, follow up care, and recommended treatment options.
