


Glaucoma remains one of the most prevalent forms of irreversible vision loss that eyecare practitioners (ECPs) will regularly encounter.1 Roughly 3 million Americans are currently affected by primary open-angle glaucoma (POAG), with the expectation for that number to double by the year 2050.2
As such, the need for providers to evaluate, monitor, and treat these patients is growing, and optometry stands to play a key role in the management of this disease. Implementing glaucoma care is essential for any medically-focused practice with significant benefits for both you and your patients.
Top tools for glaucoma diagnosis
Managing glaucoma starts with having the necessary equipment to properly diagnose the condition and subsequently monitor it in the years to come to ensure that progression is not taking place. While upfront costs may be expensive, the tools needed to properly manage glaucoma are useful for other conditions as well and stand to be a net positive for your practice.
Essential items for glaucoma management outside of the basic slit lamp with tonometer setup include:
- Pachymetry (either standalone or built into other equipment)
- Gonioscopy lenses to assess angle anatomy
- Fundus photography
- Automated visual field (VF)
- Optical coherence tomography (OCT)
- Corneal hysteresis
These tools are all necessary to establish the patient’s anatomy (pachymetry, gonioscopy, photography), intraocular pressure (tonometry), optic nerve structure (OCT), and optic nerve function (VF). Corneal hysteresis is a newer addition to this list since there is growing evidence that corneal biomechanics may play a role in accurately measuring intraocular pressure (IOP), providing further insight into the vulnerability of the optic nerve head.3
Utilizing these tests together gives a comprehensive evaluation of each patient to make an initial diagnosis and guide care for the years ahead.
Tip: Remember, glaucoma is not a condition where one test gives a “yes” or “no” answer to diagnosis. Instead, each test plays an essential role in evaluating the risk factors and monitoring for morphological changes to the optic nerve over time.
Identifying glaucoma suspects
Once equipment for proper glaucoma management has been procured, the next step is getting these patients into your practice. The easiest way to start building this base is to find those patients in your existing base who are glaucoma suspects.
This may include the following as a starter list stratified into patient history and clinical findings:4
Patient History
- Positive family history
- Race and ethnicity
- Previous history of trauma
- Cardiovascular disease
- Sleep apnea
- History of general anesthesia
- Certain autoimmune conditions (i.e., rheumatoid arthritis)
- Chronic steroid use
Clinical Findings
- IOP—Either high or asymmetric (>3mmHg between eyes)
- Optic nerve characteristics
- Increased cup-to-disc ratio
- Rim notching
- Cup-to-disc asymmetry
- Disc hemorrhage (Drance)
- Narrow angles
- Pigment dispersion or pseudoexfoliation
- Hypermature cataracts
- Recurrent uveitis
- Keratoconus
- Myopia
- Neovascularization of the iris (NVI)
- Iridocorneal endothelial (ICE) syndrome
This broad list contains historical and clinical findings observed in open-angle (primary and secondary) along with angle closure (primary and secondary) glaucoma.
In Figure 1, the optic nerve shows notching of the rim of the optic nerve inferior to inferior temporal aspect of the nerve. This nerve is highly suggestive of glaucoma, and the patient should be informed of the need for a full glaucoma evaluation.

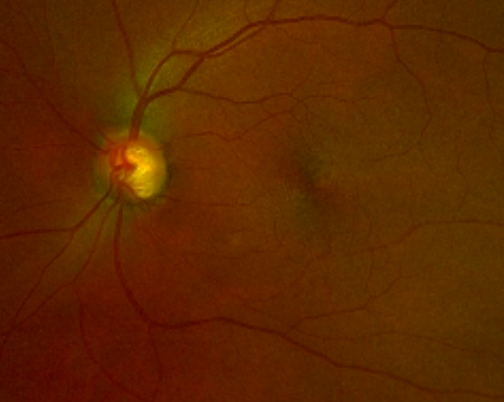
Figure 1: Courtesy of Chris Kruthoff, OD, FAAO.
Further, carefully evaluate the optic nerve of each patient who comes to see you for an annual exam. If they meet one or more of these risk factors, a follow-up visit to evaluate for glaucoma with the above tests is prudent. This initial evaluation may vary from practice to practice depending on clinic flow and patient volume.
Expanding your glaucoma patient base
Once you have a subset of glaucoma patients, build off this group by recommending visits and screenings for family members. Family history is a risk factor for most types of glaucoma,5 and at a minimum, direct relatives should have a comprehensive eye exam which may elicit further need for glaucoma evaluation.
Expanding your glaucoma patient base beyond this takes a more active approach. Consider engaging with local primary care providers to let them know that you have the requisite testing equipment to manage glaucoma patients. Highlight any advanced training and experience you may have, including any contributions you have made in the literature, research, or lecture realms. This may be extended further to optometrists who work in settings that are not equipped with OCT or VF and want to collaborate with an optometric colleague in their patient’s care.
Lastly, find and partner with glaucoma specialists and comprehensive ophthalmologists who are willing to comanage patients who require surgical care, depending on your comfort with managing more advanced stages of this disease. This will require regular communication in the early stages to build trust between all parties, but in the long run, this partnership can optimize patient care and be another avenue to grow your practice.
Patient education on POAG
Given the “silent” nature of POAG (unless significantly advanced), educating patients can often be challenging for this condition. Those who have family members with glaucoma may not need any convincing of the potentially serious nature of their disease as they may have seen firsthand the potential effects. Conversely, patients who have no prior knowledge of the disease may be skeptical that there is any issue to address, making it a tougher climb to buy into their diagnosis.
It is recommended to leverage imaging studies with patients to “prove” what you are concerned about and any areas that are problematic that would warrant treatment. I find showing patients areas of thinning on their OCT that show up in red or any defects that may appear on their VF to be especially key in helping patients see that there is an issue that needs to be addressed with appropriate treatment.
The patient in Figure 2 has asymmetric glaucoma damage. These images can be shared with the patient, highlighting areas such as retinal nerve fiber layer (RNFL) thinning, which shows as yellow and red on the Deviation Map as well as quantitative monitoring in the RNFL Quadrant and Clockhours displays at the bottom of the printout.

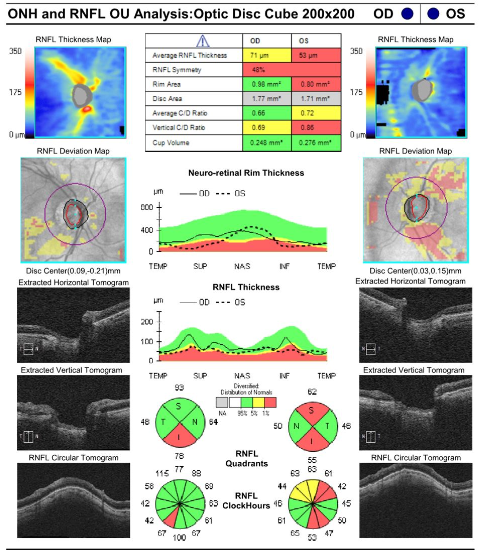
Figure 2: Courtesy of Chris Kruthoff, OD, FAAO.
Figures 3 and 4 illustrate OCT and VF findings for a patient with mild POAG OD and severe POAG OS. These images can be used to show the extent of damage OS, the presence of early damage OD that the patient may be unaware of, and comparisons to previous visits to track progression.

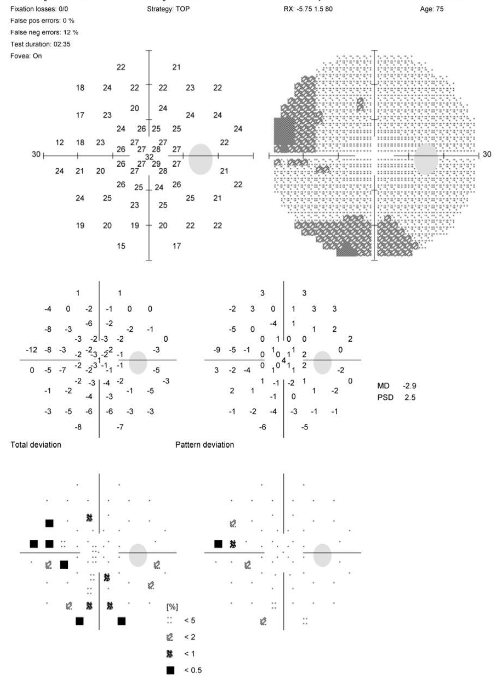

Figures 3 and 4: Courtesy of Chris Kruthoff, OD, FAAO.
It is important to share the potential ramifications of glaucoma, if not properly managed, including the potential for total vision loss. While this may not be the norm, it is important that patients are aware of the potential consequences of glaucoma and the importance of regular follow-up visits. Reassure them that, while the condition is not curable, treatments exist to slow the progression of their disease and that you will be there every step of the way to keep vision loss at bay.
Tip: Being direct and confident with this information helps to build trust from your patient and ensure that they remain diligent with their follow-up care.
Know your treatment options
Once a diagnosis has been made, treatment options to lower IOP and protect the optic nerve will require discussion to decide the next step in the patient’s care. This may include medications, selective laser trabeculoplasty (SLT), or surgical intervention depending on the stage of the condition and the level of IOP lowering needed.
Get yourself familiar with each of these options, including the major risks and benefits, so that this information is readily available when your patients ask. It is critical to keep up to date on new and emerging treatment options and trends to provide the best care for your patient.
Between new medications (such as latanoprostene bunod and netarsudil),6,7 the emergence of SLT as a frontline option,8 and the continued rise of microinvasive glaucoma surgery (MIGS),9 there has been an exciting amount of growth in the offerings we have for our patients.
This also brings the responsibility to know the pros and cons of these options and how to manage them in the short and long term. Comfort in these discussions will grow with experience and inspire confidence in your patients and comanaging providers, which will further help grow your glaucoma base.
Tip: Keep your knowledge base up to date with journals, trade publications, and conferences, seeking out courses focused on glaucoma diagnosis and management.
Benefits of establishing glaucoma care
Establishing glaucoma care in your practice is an essential part of the medical optometry model and can be a very rewarding experience. Given that glaucoma is not a curable condition, even in the most mild and controlled cases, these patients will still require a minimum annual visit, but more often will be monitored every 3 to 6 months to ensure against significant progressive damage to their optic nerve.
This allows for rapport to form with your patients as you fight to preserve their vision together. Some of my biggest word-of-mouth referrals have come from happy glaucoma patients, as we’ve developed a strong relationship due to the regular intervals of their care. These regular visits, in combination with the necessary testing to manage glaucoma, might also have a positive impact on revenue generation in your clinic.
Conclusion
As glaucoma continues to move toward an interventional model, optometrists will continue to play a vital role in the evaluation and ongoing monitoring of these patients.
Establishing yourself as a capable and willing provider for these patients will allow you and your practice to grow and thrive.
