



A 47 year old South Asian male presented complaining of central blurred vision in the right eye for one week. He reported that the blurred vision was constant, present at distance and near, and stable since onset. His previous examination was with another provider 4 months ago, at which time his reading glasses were updated and he was scheduled to follow up in 1 year. The patient had no pertinent medical history. He denied any family history of ocular disease but both his parents were diagnosed with diabetes and hypertension.
Pertinent Findings
During his self-directed evaluation for central blurred vision in the right eye, entering uncorrected visual acuities were 20/40 in the right eye and 20/20 in the left eye; right eye vision improved to 20/25-2 on pinhole. Manifest refraction was +0.50 right eye (VA 20/25-2) and plano-0.50x180 left eye (VA 20/20+). External examination and the anterior segment were unremarkable. Dilated fundus examination revealed a clear serous detachment of the right macula and pigmentary changes superior to the macula in the left eye.
Macular OCT imaging confirmed the serous retinal detachment in the right eye. The small area of pigmentary changes in the left eye corresponded to mild retinal pigment epithelial degeneration. No evidence of pigment epithelial detachment or choroidal neovascularization was noted in either eye. After the examination, the patient was re-questioned about any antecedent events and did admit to being laid off from his job several weeks prior.

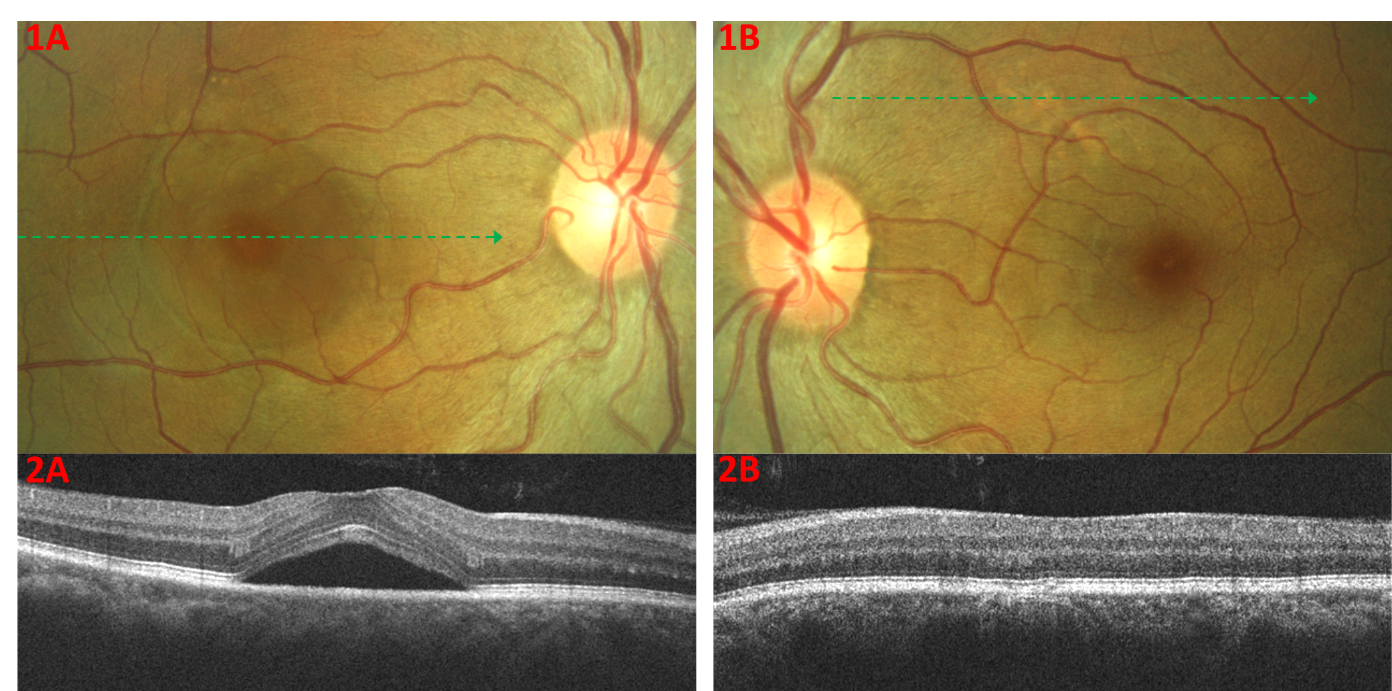
Figure 1: 1A: Fundus photo of a serous retinal detachment centered on the right eye fovea; 1B: Fundus photo of mild pigmentary changes superior-nasal to the macula in the left eye; 2A: OCT scan confirms the serous retinal detachment; 2B: OCT scan reveals mild retinal pigment epithelium degeneration without fluid
Diagnosis and Treatment
Due to the patient’s relatively young age and the presence of a unilateral serous retinal detachment, central serous chorioretinopathy was the main working diagnosis. Signs of age related macular degeneration and choroidal neovascularization were ruled out with ophthalmoscopic and OCT evaluation. There was no evidence of inflammation, neoplastic disease, or diabetic retinopathy. The presence of pigmentary changes in the unaffected left eye were consistent with pachychoroid pigment epitheliopathy; a common finding in fellow eyes of acute central serous chorioretinopathy.
The patient was apprised of all findings and the often self-limiting nature of the disease was discussed in length. The patient was educated on the use of an Amsler grid to self-evaluate his vision and a 4 week re-evaluation was scheduled. At follow up, the patient reported that his vision had returned to baseline. His refraction reverted to plano-0.50x180 in the right eye, giving him 20/20 vision again. The serous retinal detachment had resolved and only mild focal retinal pigment epithelial degeneration was noted with OCT in each eye. Since the serous retinal detachment had resolved spontaneously, a follow up for 3 months was scheduled to ensure that there was no recurrence of subretinal fluid.
Central Serous Chorioretinopathy Classification
Central serous chorioretinopathy has several clinical presentations with overlapping signs and possibly differing pathogeneses. Though no widely accepted classification criteria exist, the “classic” form of central serous chorioretinopathy is thought to be that of an acute serous retinal detachment with or without retinal pigment epithelial detachment. Patients often present complaining of blurred vision or metamorphopsia, but the majority of patients will have good best corrected vision. Dilated fundus examination reveals a serous retinal detachment with or without a retinal pigment epithelium detachment. Serous fluid is often clear without hemorrhage, but a mild turbidity may be noted in a minority of cases. This form of central serous chorioretinopathy makes up the majority of cases and has a good prognosis. Most cases will have spontaneous resolution within 3-4 months with mild sequelae. Minimal retinal pigment epithelial atrophy can be noted in >90% of patients corresponding to mild visual symptoms of reduced contrast sensitivity, metamorphopsia, and blurred vision.1 Generally, greater pigmentary changes are associated with a longer period of retinal detachment or greater number of recurrences. More serious sequelae of central serous chorioretinopathy include severe retinal pigment epithelial atrophy, outer retinal degeneration, and choroidal neovascularization which can greatly reduce visual acuity.
Reoccurrence of central serous chorioretinopathy occurs in up to 50% of cases depending on follow up length and evaluation method (clinical vs imaging).2 The recurrent serous retinal detachment is often of smaller size but visual prognosis is generally poorer due to the higher incidence of retinal pigment epithelium atrophy.
The chronic form of central serous chorioretinopathy is found in a minority of patients. Patients tend to be older but a temporal relationship may exist with younger patients with acute central serous chorioretinopathy eventually progressing to the chronic form. Recurrent or persistent retinal detachment with resultant retinal and retinal pigment epithelium atrophy may play a role in the pathogenesis of this form of central serous chorioretinopathy though longitudinal evidence for this theory is lacking. These patients will present with reduced vision, diffuse retinal pigment epithelium and retinal atrophy, and/or chronic shallow serous retinal detachments. Due to its markedly different late stage appearance, some believe that chronic central serous chorioretinopathy may have a different etiology as compared to the “classic” unilateral, self-limiting form of central serous chorioretinopathy.
Central Serous Chorioretinopathy Classification Summary3
- Acute: Serous retinal detachment with or without a serous pigment epithelial detachment lasting 3-6 months.
- Persistent or nonresolving: Patients with acute central serous chorioretinopathy lasting more than 3-6 months but with minimal pigmentary changes or retinal atrophy.
- Recurrent: New onset serous retinal detachment in a patient with a history of central serous chorioretinopathy.
- Chronic: Cases with longstanding serous retinal detachment may develop multifocal retinal pigment epithelium alterations and retinal atrophy. Eventually the serous fluid may resorb but the retinal pigment epithelium alterations and retinal atrophy will remain.
- Inactive: Patients without serous retinal detachment but with a history of central serous chorioretinopathy.
Pachychoroid and Central Serous Chorioretinopathy Pathogenesis
The etiology of central serous chorioretinopathy is not well defined, but choroidal dysfunction is thought to play a key role in its pathogenesis. The associations of exogenous and endogenous hypercortisolism, stress, and type A personalities with central serous chorioretinopathy have been known for many years, but direct pathophysiological links have still not been ascertained. Recent multimodal investigations have emphasized choroidal hyperpermeability with subsequent retinal pigment epithelium decompensation (whether physical or biochemical) and exudation into the subretinal space as the causative factor in central serous chorioretinopathy. The cause of choroidal hyperpermeability is believed to be secondary to focal choroidal ischemia with subsequent increased hydrostatic pressure. The choroidal dysfunction has been found to be bilateral but asymmetric giving credence to the theory that central serous chorioretinopathy belongs to the pachychoroid disease spectrum. This family of diseases includes pachychoroid pigment epitheliopathy, pachychoroid neovasculopathy, and pachychoroid aneurysmal type 1 neovascularization (previously known as polypoidal choroidal vasculopathy). The pachychoroid disease spectrum is characterized by diffuse or focal thickening of the choroid, choroidal hyperpermeability, dilated vessels within Haller’s layer of the choroid, inner choroidal atrophy, and reduced fundus tessellation.4
Pachychoroid Disease Spectrum Common Features
| Funduscopy | Reduced fundus tessellation |
| OCT | Diffuse or focal choroidal thickening Pachyvessels (dilated choroidal vessels of Haller’s layer) Thinning of choriocapillaris and Sattler’s layer overlying pachyvessels Atrophy of inner choroidal layers overlying pachyvessels can lead to the contradictory absence of a thickened choroid |
| OCT Angiography | Reduced choriocapillaris and Sattler’s layer flow signal |
| Fluorescein Angiography | ICGA is preferred |
| Indocyanine Green Angiography | Dilated choroidal vessels Choroidal filling defects Choroidal vascular hyperpermeability |
| Fundus Autofluorescence | Variable |
Central Serous Chorioretinopathy Management
Though there is no standardized approach to central serous chorioretinopathy management and treatment, some clinical tendencies do exist. Spontaneous resolution is noted within several months in a majority of cases of acute central serous chorioretinopathy. For this reason, even if there is suspicion that the current presentation may be a reoccurrence or a foveal presentation of previously extramacular disease, observation is usually the first choice in management. In cases of exogenous hypercortisolism, discussion with the patient’s prescribing physician should be initiated to discontinue or taper glucocorticoid treatment. It is important to rule out secondary choroidal neovascularization in these cases as that may require more rapid treatment.
In cases of persistent, recurrent, or chronic serous detachment, angiographic investigation can help guide treatment. Depending on symptoms, signs, chronicity of fluid, and the “type” of central serous chorioretinopathy various treatment protocols including laser photocoagulation, photodynamic therapy, and mineralocorticoid receptor antagonists have been used with varying degrees of success.
There is much that we still do not understand about central serous chorioretinopathy. Fortunately, the majority of patients with central serous chorioretinopathy will follow a self-limiting disease course with minimal sequelae. As the ever evolving pachychoroid disease spectrum is better elucidated, hopefully improved classification systems and treatment protocols will be developed to better manage this relatively common chorioretinal condition.
In a Nutshell
- Central serous chorioretinopathy belongs to the pachychoroid disease spectrum
- Classification of central serous chorioretinopathy is difficult due to the significant overlap of subdivisions
- Acute central serous chorioretinopathy is the most common form and is most often self-limiting without significant sequelae
- Treatment protocols vary significantly based on the subtype of central serous chorioretinopathy
References
- Liew, Gerald, et al. "Central serous chorioretinopathy: a review of epidemiology and pathophysiology." Clinical & experimental ophthalmology 41.2 (2013): 201-214.
- Kitzmann, Anna S., et al. "The incidence of central serous chorioretinopathy in Olmsted County, Minnesota, 1980–2002." Ophthalmology 115.1 (2008): 169-173.
- Singh, Sumit Randhir, and Jay Chhablani. "CSCR Classification and Its Fallacies." Central Serous Chorioretinopathy. Academic Press, 2019. 27-34.
- Cheung, Chui Ming Gemmy, et al. "Pachychoroid disease." Eye 33.1 (2019): 14-33.
