


There is general agreement in glaucoma management that small changes in intraocular pressure (IOP) can significantly affect glaucoma progression. What if I told you that a 2 mmHg reduction in IOP could be achieved just by adjusting a patient’s sleep position with a new pillow? Do you believe that postural IOP changes associated with sleep position even exist? Is any of this based on evidence, or is this just hocus-pocus?
As clinicians, we spend a lot of time keeping up to date with scientific information regarding cutting edge medications and surgical procedures in order to give our glaucoma patients the best care. However, we may be overlooking an IOP phenomena and dismissing an effective low-cost treatment option.
In this article, I will present the evidence that postural IOP changes occur during sleep, and that these IOP changes are significant enough to cause progression of glaucoma. I will propose adopting an inclined sleep position to counteract these postural IOP changes. This understanding of postural IOP changes and the use of sleep position can be a powerful adjunctive tool in your glaucoma management arsenal.
Postural IOP changes in healthy patients
Back in 1978, a study by Krieglstein et al. measured the IOP in healthy individuals and found that a “change in body position from nearly upright to head down stepwise resulted in a non-linear increase in intraocular pressure.”1 They theorized that this IOP change was “roughly correlated to ophthalmic arterial pressure and to the episcleral venous pressure postural response.”1
In the years since, many studies have tried to confirm or disprove postural IOP changes in healthy patients. Lee et al. studied several sleeping positions and concluded that compared with the sitting position, all other sleeping positions resulted in IOP elevation.2 Seo et al. also measured IOP in various positions, including the prone position with a right and left head turn. They also found that IOP increased substantially, especially in the prone position, which they attributed to “compression of neck vessels by lateral-ward flexion of [the] neck in the low head position.”3
In 2019, Mayalı et al. found only a 0.7mm Hg difference between the sitting and supine position which was not determined to be statistically significant.4 Two subsequent studies by Najmanová et al.5 and Sobczak et al.,6 utilizing the same rebound tonometer used by Mayalı et al., found IOP’s statistically higher in the supine position.
The table below offers a summary.
Postural IOP Studies on Healthy Patients
| Study | Year | Positions | Statistical Postural IOP Changes Found |
|---|---|---|---|
| Krieglstein et al.1 | 1976 | 60°, 30°, 0°,-30° | Yes |
| Lee et al.2 | 2013 | 90°, RLDP, LLDP, R&L Prone | Yes |
| Seo at al.3 | 2015 | 90°, RLDP, LLDP | Yes |
| Mayali et al.4 | 2019 | Standing, 90°, 0° | No |
| Najmanova et al.5 | 2019 | 90°, 0° | Yes |
| Sobczak et al.6 | 2021 | 90°, 0° | Yes |
RLDP=right lateral decubitus position LLDP=left lateral decubitus position R&L Prone=prone with right and left head turn. 0°=supine.
Postural IOP changes are greater in glaucoma patients
Postural IOP changes seem to be more dramatic in glaucoma patients compared with healthy patients. A review done by Prata et al., examined the literature between 1960 and 2009 regarding glaucoma patients and posture induced IOP changes. They summarized that most studies were in agreement that glaucomatous patients had a greater IOP rise from the sitting to supine position.
The table below adapted from Prata et al. demonstrates a summary of studies evaluating postural changes with IOP variation (mm Hg) compared to sitting/upright position. 7
Studies Evaluating the Influence of Postural Changes on Intraocular Pressure
| Study | Sample Size (No. eyes) | Non-glaucomatous | Glaucomatous |
|---|---|---|---|
| Anderson et al. | 1234 | 0.3 ± 1.8 | 1.6 ± 1.8 |
| Chiquet et al. | 50 | 2.2 ± 2.9 | NI |
| Hirooka et al. | 44 | 3.1 ± 0.4 | 4.0 ± 0.2 |
| Jain et al. | 259 | 2.7 | 4.1 |
| Kiuchi et al. | 66 | NI | 3.8 ± 2.1 |
| Krieglstein et al. | 142 | 2.9 | 3.9 |
| Lin et al. | 24 | 16.3 ± 0.4 to 20.4 ± 0.4 | 19.6 ± 0.7 to 23.1 ± 0.7 |
| Longo et al. | 11 | 13 ± 1 to 17 ± 2 | NI |
| Parsley et al. | 140 | <2 mm Hg in 100% of cases | <2 mm Hg in 93% of cases |
| Tsukahara et al. | 45 | 5.6 ± 1.7 | 8.6 ± 3.5 |
| Yamabaiashi et al. | 57 | 4.4 ± 2 | 4.1 ± 1.8 |
| Carlson et al. | 41 | 2.4 ± 1.2 (position ± 15°) 11.2 ± 2.7 (position ± 50°) | NI |
| Linder et al. | 10 | up to 3X baseline | NI |
| Weinren et al. | 31 | 16.8 ± 2.8 ± to 32.9 ± 7.9 | 21.3 ± 2.3 to 37.6 ± 5.0 |
NI=Not Included. Values are given as mean ± standard deviation whenever possible.
Recent studies have confirmed that postural IOP changes are more pronounced in glaucoma patients compared with healthy patients. Katsanos et al. examined normal patients, treated primary open angle glaucoma (POAG) patients and untreated POAG patients in various positions. Their findings showed that all groups showed an IOP rise as the patients moved away from the sitting position.
Further, they found that “compared to controls, the magnitude of posture-induced IOP changes [was] greater in eyes with POAG irrespective of treatment.”8 In 2021, the team of Ireka et al. concluded that the “[g]reatest variations in posture induced IOP occurred in POAG patients” compared to healthy patients and that this IOP variation was ”lowest in the sitting position and highest in the supine flat position.”9
Postural IOP changes in glaucoma subtypes
While most studies concur that postural IOP changes are exaggerated in glaucoma patients, there is some uncertainty as to whether certain glaucomatous pathologies are more susceptible to postural IOP changes. Various studies have examined postural IOP changes in patients with POAG, primary angle closure (PAC), and pseudoexfoliation glaucoma (PXG). Despite some correlative overtones, no definitive statistical differences were found in these studies.10,11,12,13
However, regarding pigment dispersion syndrome and pigment dispersion glaucoma patients, Sedgewich et al. felt so strongly that the IOP increases they found were so significant in magnitude that they recommended that all pigment dispersion patients should avoid sleeping in the prone position.14
Postural IOP changes and visual field loss
Postural IOP changes can translate to actual glaucoma progression, especially in the side sleeping position, or the lateral decubitus position (LDP). Kim et al., detected a correlation between the LDP and asymmetric visual field loss. They studied glaucoma patients that already had asymmetric Humphrey visual field loss and noted that 75.5% preferred to sleep in the LDP, of which 75.7% actually preferred to sleep on the side of the eye with the more significant visual field loss.
Statistically, this preference of sleeping in the LDP on the side of the worse visual field applied to 57.1% of all the patients studied. They concluded that glaucoma patients seemed to be partial to the LDP in particular, and that the LDP was associated with asymmetrical visual field damage.15 Manambe et al. further suggested that postural IOP changes associated with the LDP could “cause glaucomatous superior paracentral visual field defect[s].”16
One final consideration in the LDP is concerning ocular compression by pillow during sleep. A couple of studies pointed out that ocular compression by a pillow in side sleepers can result in marked IOP elevation that could be potentially damaging in glaucoma patients.17,18 Thus, they both urged clinicians to rule out any ocular compression during sleep, and Korenfeld even recommended a rigid fox shield for patients that exhibited high exophthalmometry readings.18
Postural IOP changes, sleep positions, and pillow considerations
Several studies have estimated the IOP reduction that is possible with the inclined sleep position compared with the supine position.
Lazarro et al. found 83.3% of all patients had lower nocturnal IOP’s in the 20o position compared with the supine position. Glaucoma and non-glaucoma patients had IOP reductions of 9.33% and 8.67% respectfully.19 A study by Buys et al, compared the supine and 30o position in glaucoma patients and discovered that 94.1% of the patients had lower IOP’s at 30o and that the reduction in IOP was 20% or more in over one third of the patients.20
Both studies used wedge pillows.
Figure 1 represents the wedge pillow set up used by Buys et al.20

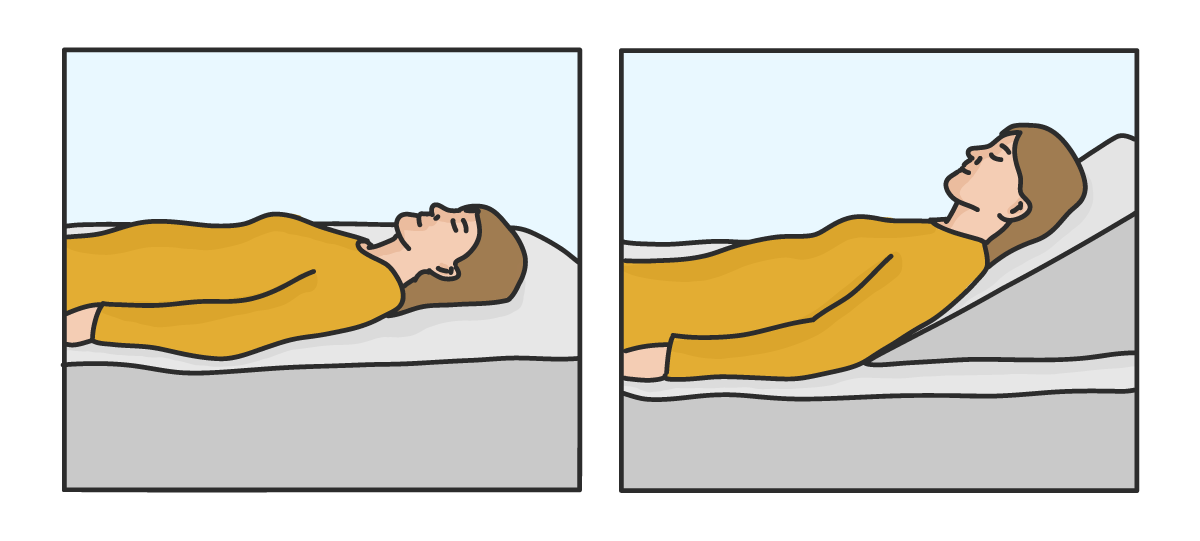
Figure 1
Other studies have investigated the use of multiple pillows compared to a bed adjusted on an incline. Yeon et al. and Park et al. showed sizeable decreases in IOP with the 30o position achieved by the bed, but both studies noted that the use of multiple pillows to prop the head up was not as effective due to craniocervical flexion and compression of the neck vessels.21,22 Park et al. placed particular importance on elevating the upper torso rather than just elevating the head.22
Figure 2 demonstrates the different supine sleep positions and neck flexion by pillows.22


Figure 2
The table below provides a summary of studies on IOP and incline.
Summary of Studies, IOP and Incline.
| Study | Incline | Average IOP Change | Pillow/Bed Considerations |
|---|---|---|---|
| Lazorro et al.19 | 20° | -1.51mmHg | Wedge Pillow |
| Buys et al.20 | 30° | -3.20mmHg | Wedge Pillow |
| Yeon et al.21 | 30° | -2.80mmHg | Bed adjusted with incline |
| Park et al.22 | 30° | -2.00mmHg | Bed adjusted with incline |
Pillow considerations
Sleeping on an incline, also known as inclined bed therapy, elevated head sleeping, or sleeping inclined, has been recommended for acid reflux and other conditions such as snoring. Other than investing in a bed that can provide upper body inclination, the easiest and most cost effective solution would be to purchase a stiff wedge pillow.
There are almost an infinite amount of wedge pillow sizes and shapes, as well as firmness and luxurious material options, that range in cost from $30 to $100+. I bought this wedge pillow for $50: It is moderately firm and has an egg crate type surface that is fairly comfortable.
Figure 3, below, represents the author's pillow choice: a foam wedge pillow measuring 22’’ long, 19’’ wide with a 12’’ rise height giving a 28.6o angle of inclination.


Figure 3
It should be noted that changing one’s sleep position can take a bit of effort, and may require some trial and error with different pillow set ups. Patients may have rigid sleep habits and preferences so they should be gently encouraged to persist in adjusting their sleep position if any resistance is encountered.
Using sleep position as an adjunctive tool for glaucoma management
The evidence has shown that postural differences affect IOP, with increasing IOP changes occurring from the sitting to various supine positions. Given that we spend much of our lives in the supine position during sleep, it would be totally valid to consider IOP increases at night affecting glaucoma patients. This can be especially important in patients that profess medication compliance and display low IOP measurements in the office, but show progression of their glaucoma.
As clinicians, we know that even small IOP changes, higher or lower, can influence glaucoma progression. If most glaucoma medications deliver a range of 20-30% reduction in IOP, utilizing a 30o sleep position to possibly reduce the IOP by 2 mmHg would be very reasonable.
Part of the glaucoma management process should involve considering postural IOP changes, ruling out ocular compression, and discussing different sleep positions, such as sleeping on a 30o incline. With the understanding of postural IOP differences, sleep positions can be a powerful adjunctive tool that clinicians can use in their glaucoma management arsenal. Good night!
References
- Krieglstein GK, Waller WK, Leydhecker W. The vascular basis of the positional influence of the intraocular pressure. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1978 May 2;206(2):99-106. doi: 10.1007/BF00414618. PMID: 306777.
- Lee TE, Yoo C, Kim YY. Effects of different sleeping postures on intraocular pressure and ocular perfusion pressure in healthy young subjects. Ophthalmology. 2013 Aug;120(8):1565-70. doi: 10.1016/j.ophtha.2013.01.011. Epub 2013 Apr 3. PMID: 23561328.
- Seo H, Yoo C, Lee TE, Lin S, Kim YY. Head position and intraocular pressure in the lateral decubitus position. Optom Vis Sci. 2015 Jan;92(1):95-101. doi: 10.1097/OPX.0000000000000432. PMID: 25437907.
- Mayalı H, Tekin B, Kayıkçıoğlu ÖR, Kurt E, İlker SS. Evaluation of the Effect of Body Position on Intraocular Pressure Measured with Rebound Tonometer. Turk J Ophthalmol. 2019 Feb 28;49(1):6-9. doi: 10.4274/tjo.galenos.2018.90359. PMID: 30829018; PMCID: PMC6416475.
- Najmanová E, Pluháček F, Haklová M. Intraocular pressure response affected by changing of sitting and supine positions. Acta Ophthalmol. 2020 May;98(3):e368-e372. doi: 10.1111/aos.14267. Epub 2019 Oct 10. PMID: 31602816; PMCID: PMC7216979.
- Sobczak M, Asejczyk M, Geniusz M. Does body position, age, and heart rate induce IOP's changes? Eur J Ophthalmol. 2021 Jun 6:11206721211023313. doi: 10.1177/11206721211023313. Epub ahead of print. PMID: 34096356.
- Prata TS, De Moraes CG, Kanadani FN, Ritch R, Paranhos A Jr. Posture-induced intraocular pressure changes: considerations regarding body position in glaucoma patients. Surv Ophthalmol. 2010 Sep-Oct;55(5):445-53. doi: 10.1016/j.survophthal.2009.12.002. Epub 2010 Jul 16. PMID: 20637484.
- Correction to: The Effect of Posture on Intraocular Pressure and Systemic Hemodynamic Parameters in Treated and Untreated Patients with Primary Open-Angle Glaucoma, by Katsanos, A., Dastiridou, A.I., Quaranta, L., Rulli, E., Riva, I., Dimasi, V., Tsironi, E.E., and Weinreb, R.N. J Ocul Pharmacol Ther 2017;33(8):598-603. DOI: 10.1089/jop.2017.0030. J Ocul Pharmacol Ther. 2018 Apr;34(3):309. doi: 10.1089/jop.2017.0030.correx. Epub 2018 Feb 2. Erratum for: J Ocul Pharmacol Ther. 2017 Oct;33(8):598-603. PMID: 29393727; PMCID: PMC5963873.
- Ireka OJ, Ogbonnaya CE, Arinze OC, Ogbu N, Chuka-Okosa CM. Comparing posture induced intraocular pressure variations in normal subjects and glaucoma patients. Int J Ophthalmol. 2021 Mar 18;14(3):399-404. doi: 10.18240/ijo.2021.03.11. PMID: 33747816; PMCID: PMC7930549.
- Sawada A, Yamamoto T. Posture-induced intraocular pressure changes in eyes with open-angle glaucoma, primary angle closure with or without glaucoma medications, and control eyes. Invest Ophthalmol Vis Sci. 2012 Nov 13;53(12):7631-5. doi: 10.1167/iovs.12-10454. PMID: 23099489.Tabl
- Park JH, Yoo C, Yang KS, Kim YY. Effects of Different Body Postures on the Intraocular Pressure in Patients with Primary Angle-Closure Disease. Optom Vis Sci. 2019 Jul;96(7):477-483. doi: 10.1097/OPX.0000000000001399. PMID: 31274735.
- Ozkok A, Tamcelik N, Capar O, Atalay E. Posture-induced changes in intraocular pressure: comparison of pseudoexfoliation glaucoma and primary open-angle glaucoma. Jpn J Ophthalmol. 2014 May;58(3):261-6. doi: 10.1007/s10384-014-0314-8. Epub 2014 Mar 15. PMID: 24627149.
- Dar N, Belkin A, Pillar S, Sheiman V, Tempelhof OF, Barkana Y, Geffen N. Effects of Postural Variation on Intra-ocular Pressure: Comparison between Pseudo-exfoliation Glaucoma and Primary Open Angle Glaucoma. Curr Eye Res. 2020 Oct;45(10):1309-1314. doi: 10.1080/02713683.2020.1739313. Epub 2020 Mar 13. PMID: 32141781.
- Sedgewick JH, Sedgewick JA, Sedgewick BA, Ekmekci B. Effects of different sleeping positions on intraocular pressure in secondary open-angle glaucoma and glaucoma suspect patients. Clin Ophthalmol. 2018 Aug 1;12:1347-1357. doi: 10.2147/OPTH.S163319. PMID: 30122886; PMCID: PMC6078092.
- Kim KN, Jeoung JW, Park KH, Lee DS, Kim DM. Effect of lateral decubitus position on intraocular pressure in glaucoma patients with asymmetric visual field loss. Ophthalmology. 2013 Apr;120(4):731-5. doi: 10.1016/j.ophtha.2012.09.021. Epub 2012 Dec 20. PMID: 23260257.
- Manabe Y, Sawada A, Yamamoto T. Localization in Glaucomatous Visual Field Loss Vulnerable to Posture-Induced Intraocular Pressure Changes in Open-Angle Glaucoma. Am J Ophthalmol. 2020 May;213:9-16. doi: 10.1016/j.ajo.2020.01.010. Epub 2020 Jan 15. PMID: 31953057.
- Kim HS, Park KH, Jeoung JW. Can we measure the intraocular pressure when the eyeball is against the pillow in the lateral decubitus position? Acta Ophthalmol. 2013 Nov;91(7):e502-5. doi: 10.1111/aos.12151. Epub 2013 Apr 23. PMID: 23607647.
- Korenfeld MS, Dueker DK. Review of external ocular compression: clinical applications of the ocular pressure estimator. Clin Ophthalmol. 2016 Feb 23;10:343-57. doi: 10.2147/OPTH.S92957. PMID: 26966349; PMCID: PMC4770069.
- Lazzaro EC, Mallick A, Singh M, Reich I, Elmann S, Stefanov DG, Lazzaro DR. The effect of positional changes on intraocular pressure during sleep in patients with and without glaucoma. J Glaucoma. 2014 Jun-Jul;23(5):282-7. doi: 10.1097/01.ijg.0000435848.90957.fe. PMID: 24248001.
- Buys YM, Alasbali T, Jin YP, Smith M, Gouws P, Geffen N, Flanagan JG, Shapiro CM, Trope GE. Effect of sleeping in a head-up position on intraocular pressure in patients with glaucoma. Ophthalmology. 2010 Jul;117(7):1348-51. doi: 10.1016/j.ophtha.2009.11.015. Epub 2010 Feb 25. PMID: 20188421.
- Yeon DY, Yoo C, Lee TE, Park JH, Kim YY. Effects of head elevation on intraocular pressure in healthy subjects: raising bed head vs using multiple pillows. Eye (Lond). 2014 Nov;28(11):1328-33. doi: 10.1038/eye.2014.211. Epub 2014 Sep 5. PMID: 25190537; PMCID: PMC4274296.
- Park JH, Nam KT, Yoo C, Kim YY. Head Elevation and Intraocular Pressure in Glaucoma. Optom Vis Sci. 2016 Sep;93(9):1163-70. doi: 10.1097/OPX.0000000000000895. PMID: 27232904.
