


Let’s start this article with a dramatic statement: differentiating glaucoma from non-glaucomatous optic neuropathy (NGON) can be a vision- or potentially life-saving diagnosis.
Conditions that can lead to NGON include serious systemic diseases like giant cell arteritis, compressive lesions, or severe nutritional deficiencies.
This article will familiarize you with the signs and symptoms of NGON and how to discern it from glaucoma.
Comparing glaucoma and NGON
So, what is the difference between glaucoma and NGON? We know that glaucoma is an acceleration of retinal ganglion cell death, leading to thinning of the neuroretinal rim and subsequent enlargement of the cup.
It is often, but not always, accompanied by elevated intraocular pressure (IOP). Due to redundancy in the visual pathway, symptomatic vision loss is typically a late finding in glaucoma.
NGON, on the other hand, occurs when damage occurs to the optic nerve, leading to degeneration of the neural tissue. The damage can be acute, as in trauma, or insidious, as in compressive lesions. Frequently, the cup will enlarge, and the remaining neuroretinal rim will become pale.
Table 1 highlights the differences in signs and symptoms between glaucoma and non-glaucomatous optic neuropathy. *Afferent pupillary defect (APD) will only be present in unilateral and/or asymmetric optic neuropathies.
| Signs and Symptoms | Glaucoma | Non-Glaucomatous Optic Neuropathy |
|---|---|---|
| Visual Acuity Loss | Late | Earlier |
| Color Vision Deficits | Late, subtle | Earlier |
| Afferent Pupillary Defect* | Can be early | Earlier |
| Visual Field Loss | Moderate to severe stage | Defects can be variable |
| Optic Nerve Pallor | None except in advanced cupping | Variable timing, can be diffuse or sectoral |
| Retinal Nerve Fiber Layer (RNFL) Loss | Superior-temporal and/or inferior-temporal | Any, including the papillomacular bundle (PMB) and nasal bundles |
| Ganglion Cell Complex (GCC) Loss | Superior and/or inferior | Any, including diffuse or hemianopic |
Table 1: Courtesy of David Holland, OD.
Optic atrophy caused by NGON
Optic atrophy is the term used when optic nerve pallor occurs and is considered an end-stage marker of non-glaucomatous optic nerve disease. It takes approximately 4 to 6 weeks to develop optic atrophy after the initial injury.1
Further, it can be categorized into primary or secondary optic atrophy. The difference is that secondary optic atrophy is preceded by optic disc swelling, while primary optic atrophy is not. A third category, consecutive optic atrophy, arises from widespread retinal disease.1
The epidemiology of NGON
According to the Centers for Disease Control and Prevention (CDC), approximately 3 million Americans have glaucoma. A study by Wiggs et al., found that the prevalence of glaucoma is 2.2% worldwide.2 Of note, studies have also shown that glaucoma is more common in people of African descent compared to Caucasians (5.57% vs. 2.2%).3
Non-glaucomatous optic neuropathy is less common than glaucoma. Optic atrophy, being a marker of disease rather than a disease itself, has not undergone many investigations into its prevalence. A study of nursing home residents found that the prevalence of optic atrophy was 0.8% of residents with significant visual impairment.4
So, while NGON is not very common, it is always good to remember that “it ain’t rare if it’s in your chair!”
Presentation of non-glaucomatous optic neuropathy
The hallmark clinical sign of optic atrophy is optic disc pallor.
Figure 1 highlights fundus photography of optic disc pallor caused by optic atrophy.

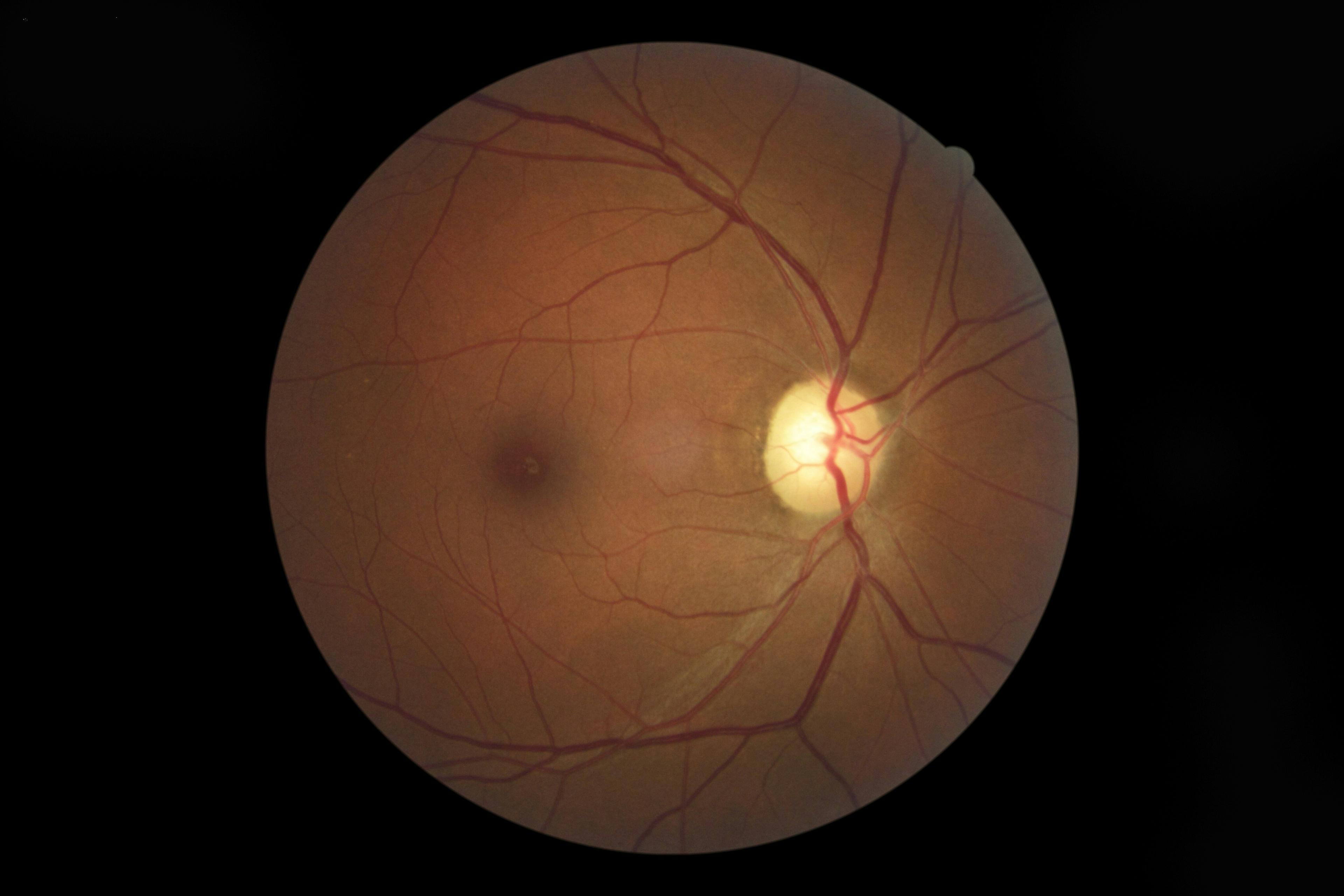
Figure 1: Courtesy of David Holland, OD.
The degeneration of ganglion cell axons and the loss of capillaries causes the optic disc to lose its pinkish hue and become white or pale. Pallor can be diffuse (involving the entire optic disc) or sectoral (involving a section of the optic disc).
Signs of non-glaucomatous optic neuropathy:
- Optic disc pallor
- Diffuse RNFL loss on optical coherence tomography (OCT) testing, including the papillomacular bundle
- Diffuse ganglion cell-inner plexiform layer (GC-IPL) thinning on OCT testing
- Generalized depression on visual field (VF) testing
- Any type of localized visual field defect
Symptoms of non-glaucomatous optic neuropathy:
- Visual acuity loss (sometimes out of proportion to observed cupping)
- Color vision changes
- Asymptomatic (early)
It is very important to note that glaucoma does not cause optic disc pallor except in end-stage glaucoma with severe cupping, but this is not considered true optic atrophy. If you see an optic disc with a pale rim, optic atrophy needs to be on the list of differential diagnoses.
Vision loss in NGON
The hallmark clinical symptom of optic atrophy is vision loss. This is a useful differentiator between glaucoma and optic atrophy. Glaucoma typically does not cause visual acuity loss until late in the disease process.
If a patient presents with moderate cupping but a significantly reduced visual acuity, start paying close attention to the rim color to check for pallor—this may be optic atrophy.
Acquired color deficiency due to NGON
An acquired color deficiency is often an indicator of optic neuropathy. Glaucoma can cause color vision changes but is often a late finding and is not typically significant. If you are suspicious about optic atrophy, pull out your Ishihara or HRR test or even a red cap desaturation test.
Any acquired changes or loss of color vision should always prompt the clinician to suspect non-glaucomatous optic neuropathy.
Afferent pupillary defect secondary to NGON
An APD is frequently seen in non-glaucomatous optic neuropathy if the optic neuropathy is unilateral or asymmetric. It is associated with decreased visual acuity, but the acuity may only be mildly reduced in the early stages.
Glaucoma can cause an afferent pupillary defect but only in the late stages with significant cupping and RNFL loss. The presence of an APD in an eye without advanced glaucoma requires further evaluation for non-glaucomatous optic neuropathy. Remember, however, that an APD will only present if the disease is unilateral or very asymmetric.
Ancillary testing for NGON
Optical coherence tomography testing can be very helpful in differentiating glaucoma from optic atrophy. Pay close attention to the ganglion cell-inner plexiform layer scan. The GC-IPL includes the axons of the ganglion cells, which form the neurosensory portion of the optic nerve.
Thus, damage to the optic nerve will show as thinning of the GC-IPL layer. The pattern of GC-IPL loss will match the pattern of disc pallor. If the entire optic disc is pale, the entire GC-IPL will be thin. With sectoral pallor of the disc, the GC-IPL will be thin in those areas serving the atrophic area of the nerve.
You can also see a pseudo-homonymous defect (Figure 2) in patients with neurologic disease. Glaucoma can also cause diffuse GC-IPL thinning, but only in the presence of advanced disease. Of note, GC-IPL thinning out of proportion to the cupping should raise a red flag.
Figure 2 demonstrates OCT imaging of a pseudo-homonymous defect in a patient with neurologic disease.

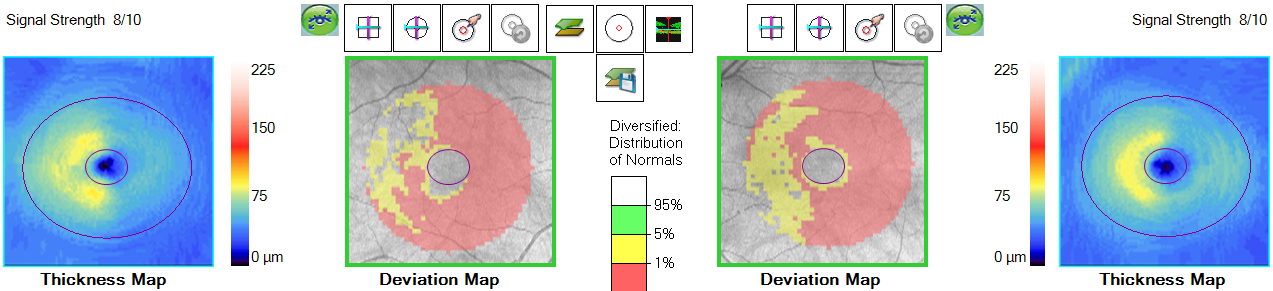
Figure 2: Courtesy of David Holland, OD.
Visual field testing can also be used to differentiate glaucoma from optic atrophy. With glaucoma, the defects are usually nasal or central and respect the horizontal midline. NGON can cause any type of visual field defect. Diffuse optic atrophy tends to cause diffuse depressions across the entire visual field.
Etiologies of non-glaucomatous optic neuropathy
There are many causes of NGON, and listing all of them would be beyond the scope of this article. We can simplify things by looking at several categories of disease and an example of each.
Ischemic and inflammatory disease
A common cause of optic nerve pallor is ischemic optic neuropathy. Non-arteritic ischemic optic neuropathy (NAION) is the most common optic neuropathy in adults over 50 years of age.5
In the acute stage, NAION presents with an acute loss of vision, often in an altitudinal pattern. The optic nerve will appear swollen with peripapillary hemorrhages. Over time, the swelling will subside, leaving a pale nerve.
One of the most feared inflammatory optic neuropathies is giant cell arteritis. While not a very common cause of optic atrophy, it needs to be on the differential for any patient over age 55 years with unexplained optic disc pallor.
We should all be familiar with the typical systemic signs of giant cell arteritis—jaw claudication, skin tenderness over the temporal artery, fever of unknown origin, and headaches. It can also present early with optic disc pallor.
This can be a blessing in disguise because intervention can be initiated before the onset of arteritic anterior ischemic optic neuropathy (A-AION) with its attendant profound and irreversible vision loss.5
Compressive lesions
Compression of the optic nerve by a tumor, such as an optic nerve sheath meningioma, can cause slow progressive visual loss. Other signs of optic nerve dysfunction, such as color vision changes, visual field defects, and an APD, can also occur. Further, optic disc pallor (and/or edema) can also occur.
Nutritional deficits
Vitamin B deficiency can lead to pallor of the temporal portion of the optic nerve and thinning of the RNFL in the papillomacular bundle. This deficiency is not very common, but it can be seen in patients with previous bariatric surgery (e.g., gastric bypass), digestive malabsorption diseases (e.g., celiac disease), and strict vegan/vegetarian diets.6
Genetic disease
Autosomal dominant optic atrophy is the most common inherited optic neuropathy with an onset in the first and second decades of life.7 Vision loss is slow and progressive, typically staying 20/200 or better. Central scotomas are common due to optic atrophy of the temporal portion of the optic disc.7
Trauma
Traumatic optic neuropathy occurs after blunt or penetrating head trauma. Vision loss occurs very soon after the injury, although the optic nerve may initially appear normal. After 4 to 6 weeks, optic atrophy with pallor typically appears.
Other causes of NGON
Previous optic neuropathy, such as optic neuritis or papilledema, can lead to chronic optic disc pallor.9 Heavy pan-retinal photocoagulation leads to optic nerve pallor due to the destruction of a significant portion of the retina.
Previous vascular occlusions, both artery and vein, can also cause late optic nerve pallor.
NGON case report: Giant cell arteritis
Let’s look at a case of giant cell arteritis. An 80-year-old white male presented as a glaucoma suspect after having undergone uncomplicated, bilateral cataract surgery. His corrected visual acuity was 20/40 OD and 20/25 OS. Also, his IOP was 17mmHg with a central corneal thickness of over 600 microns OU. A positive APD was seen OD.
A dilated fundus exam revealed pale optic discs with a 0.7 cup-to-disc ratio OU. The optic nerve OCT showed diffuse RNFL loss OD (including the papillomacular bundle) and significant superior temporal and inferior temporal RNFL loss OS (Figure 3). The GCC scan showed diffuse and severe loss of the GCC OU (Figure 4).
Visual field testing showed a generalized depression OU with an underlying inferior arcuate defect OD and an inferior nasal step OS with accompanying superior defects.
Figure 3 shows optic nerve head (ONH) and RNFL scans of diffuse RNFL loss OD and superior temporal and inferior temporal RNFL loss OS.

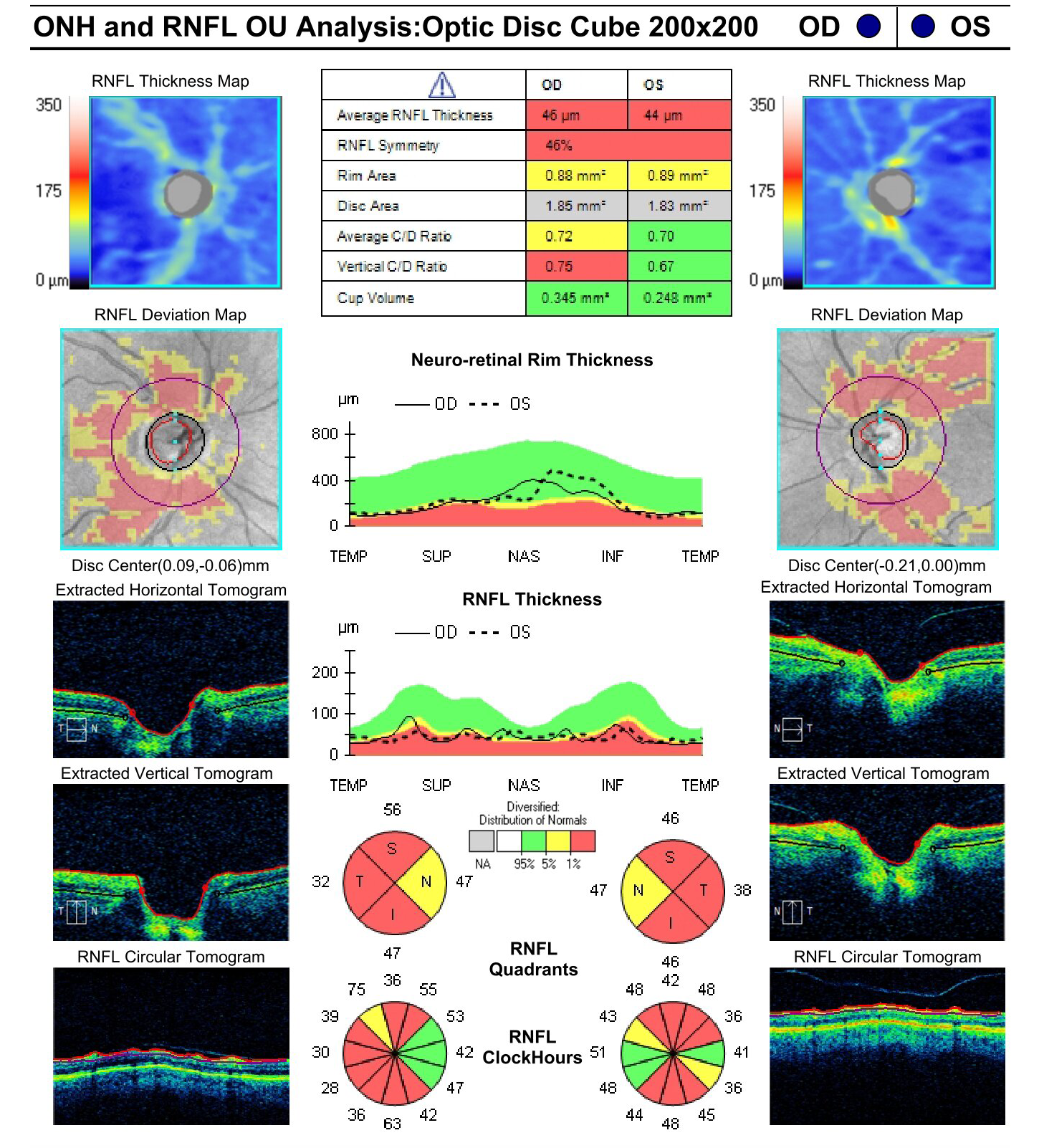
Figure 3: Courtesy of David Holland, OD.
Figure 4 features a GCC scan with diffuse and severe loss of the GCC bilaterally.

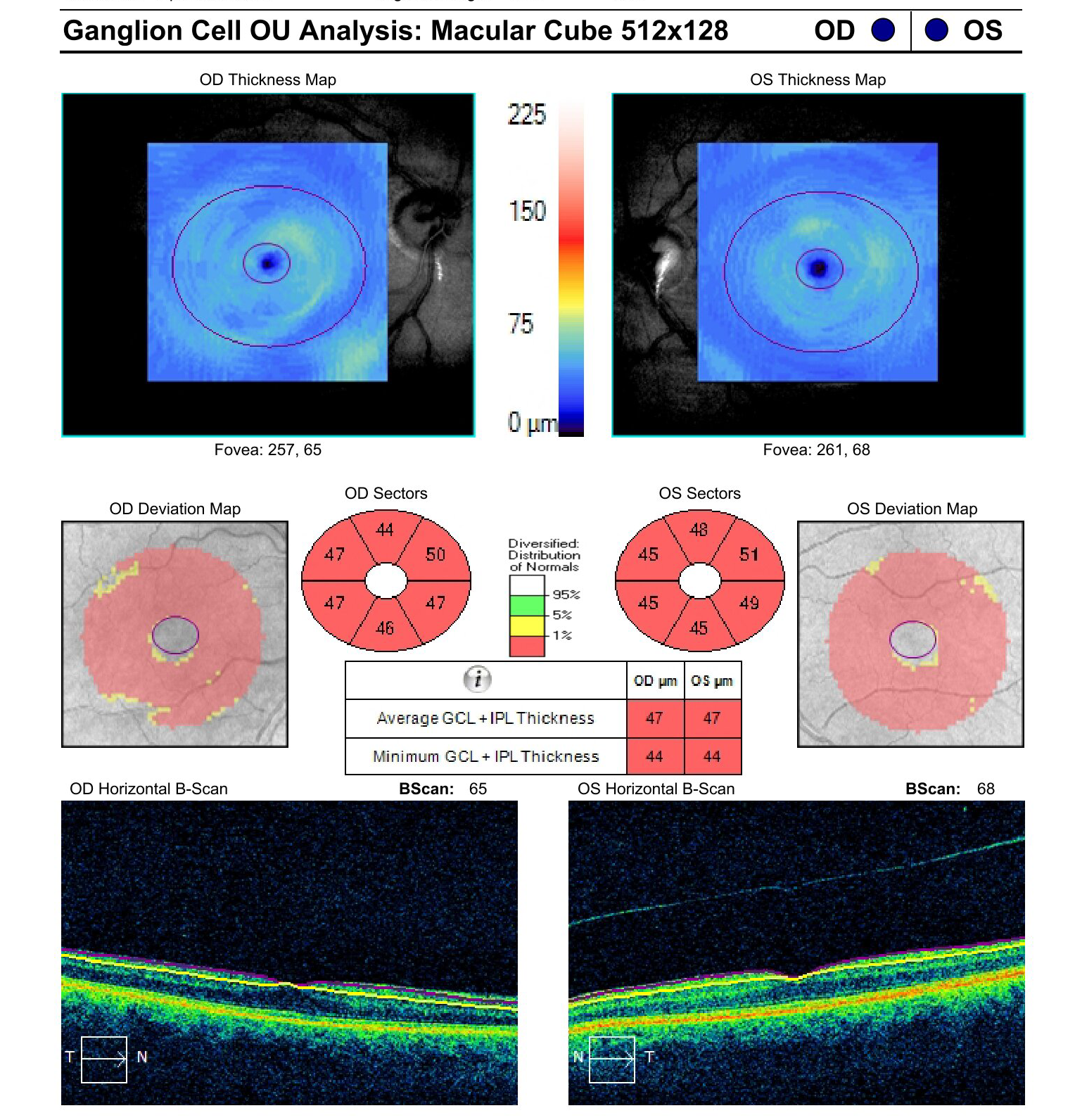
Figure 4: Courtesy of David Holland, OD.
This patient had some features of possible glaucoma (i.e., cupping, arcuate field defects) but the decreased visual acuity, optic disc pallor, and severe RNFL and GCC loss were all suggestive of optic atrophy.
This patient was referred to our local neuro-ophthalmologist. After a thorough workup, including a temporal artery biopsy, the patient was diagnosed with giant cell arteritis. Without timely intervention, this patient may have had profound vision loss from arteritic ischemic optic neuropathy.
Co-managing non-glaucomatous optic nerve disease
So, if you suspect NGON, what should you do? These cases are best managed or co-managed with a neuro-ophthalmologist. The underlying cause of optic atrophy may need a team of specialists, including neuro-ophthalmologists, neurologists, rheumatologists, and oncologists.
Our role as eyecare providers is to spot the disease and make the appropriate and timely referral. Co-managing these patients would include serial visual field testing and OCT scans. Depending upon your state laws and your level of comfort, you can order neuroimaging and blood tests.
This can be useful if there is a long wait time to get the patient to a neuro-ophthalmologist. The results of these tests can be forwarded to the neuro-ophthalmologist in order to reduce any delays in diagnosis.
Case report: Non-glaucomatous optic neuropathy
A white female in her mid-60s presented to the office as a new patient. She had been previously diagnosed with primary open-angle glaucoma (POAG) and was using Travatan eye drops. However, she ran out of the drops several months ago. She also had undergone selective laser trabeculoplasty (SLT) in both eyes at her previous eyecare provider’s office.
Her medical history was significant for a history of hypertension, for which she took no medication at this time. Her surgical history was significant for a cholecystectomy, hernia repair, and two C-sections. She had a remote family history of glaucoma.
Her uncorrected visual acuity was 20/70 OD, and light perception (LP) OS with no improvement with pinhole in either eye. Her extraocular muscle (EOM) movements were full and smooth. She had an APD OS. Her IOP was measured as 18mmHg OD and 20mmHg OS measured via Tonopen.
Her slit lamp exam showed bilateral dermatochalasis and meibomian gland dysfunction (MGD), as well as epithelial basement membrane dystrophy (EBMD) and moderate nuclear sclerotic cataracts. A dilated fundus exam showed almost no cupping in either optic nerve and significant optic nerve pallor.
Looking at the fundus photo (Figures 5 and 6), we can see significant pallor of the optic nerve. Additionally, OCT of the optic nerve is shown in Figure 7 with diffuse RNFL loss OU. Her VF in Figure 8 shows dense, diffuse depressions OU.
Figures 5 and 6 highlight fundus photography of significant optic nerve pallor.


Figure 5: Courtesy of David Holland, OD.


Figure 6: Courtesy of David Holland, OD.
Figure 7 shows OCT imaging of the patient’s optic nerve with diffuse RNFL loss OU.

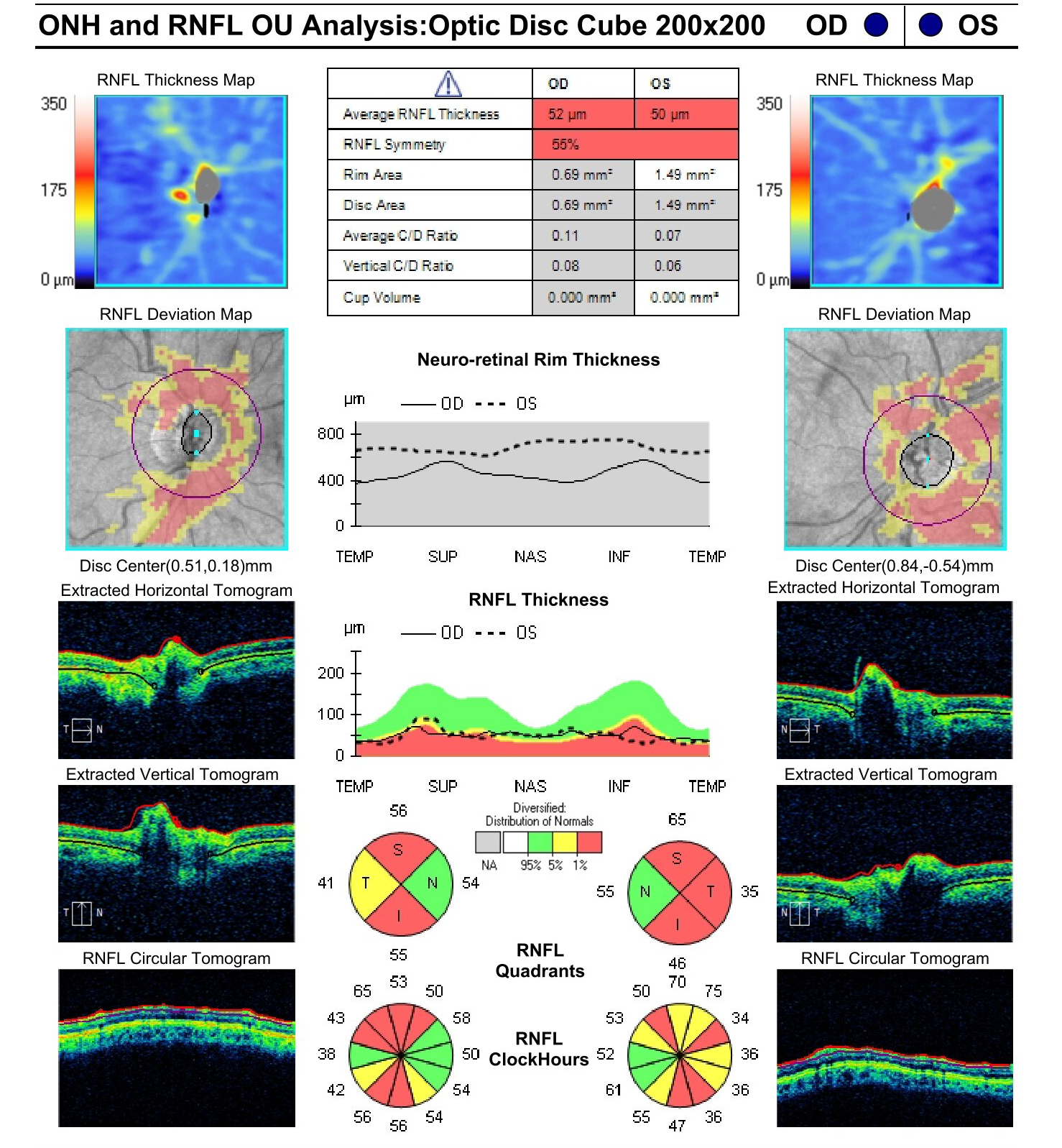
Figure 7: Courtesy of David Holland, OD.
Figure 8 features the patient’s visual field testing, with dense and diffuse depressions bilaterally.

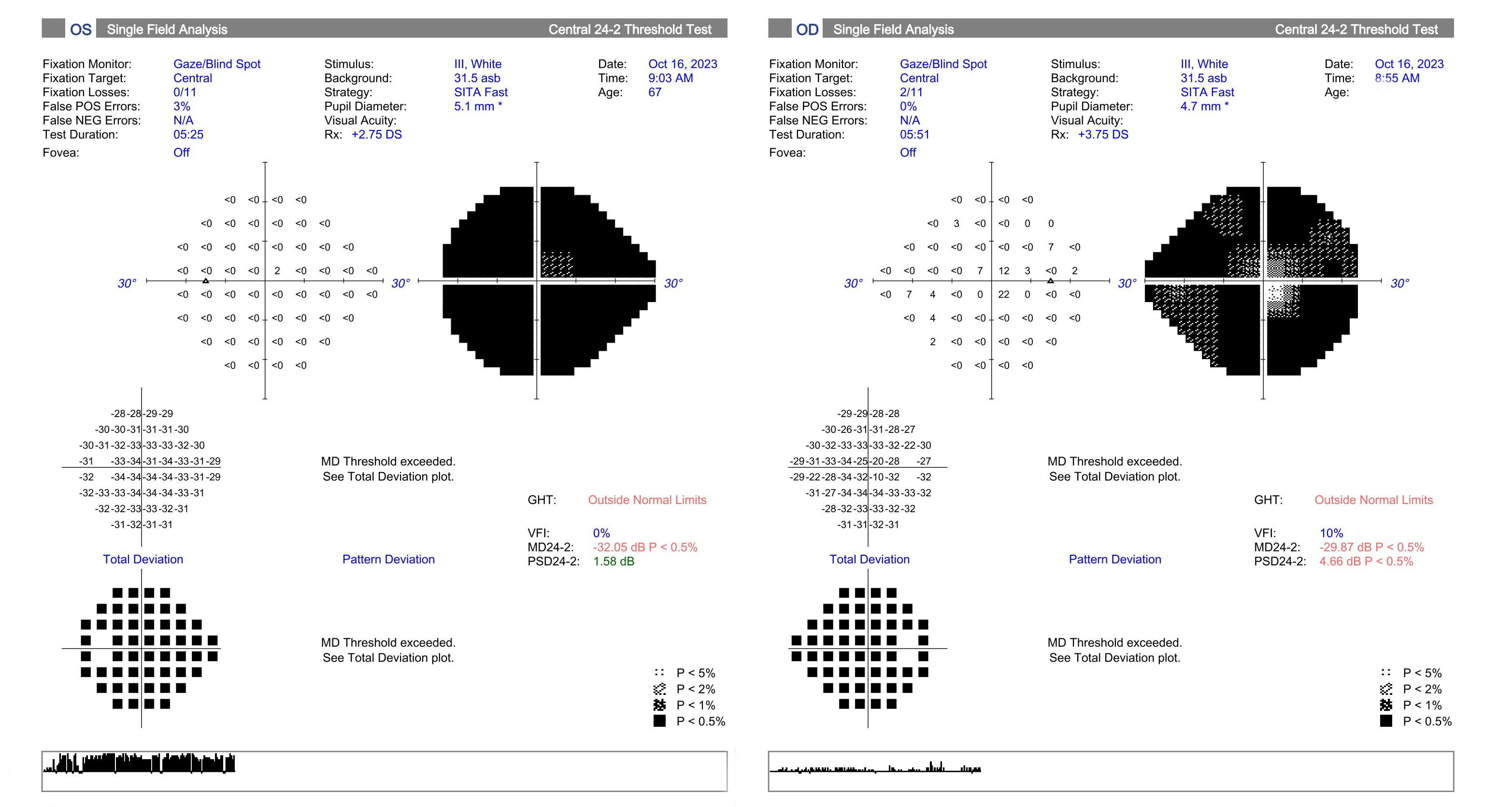
Figure 8: Courtesy of David Holland, OD.
None of this is suggestive of glaucoma, aside from borderline high IOP. This was a clear case of optic atrophy that required further evaluation. This patient was referred to our local neuro-ophthalmologist.
Conclusion
Non-glaucomatous optic neuropathy can be a difficult condition to diagnose, but the ramifications for the patient can be life-changing.
Paying close attention to the optic disc color, the pattern of OCT, and visual field changes can help make this diagnosis. Hopefully, this article will help you make these calls.
Remember—glaucoma does not cause optic nerve pallor except in late stages!
