


WHAT YOU'LL LEARN
How to recognize the pathophysiology of TON
How to diagnose TON
What to look out for in patients with TON
How to care for TON patients
TON is a finding, not a diagnosis
Few clinical findings make eye care practitioners more unsettled than the presence of unexplained atrophy to the optic nerve. The differential diagnosis of optic nerve pallor can be broad, with etiologies ranging from benign to sight/life-threatening. Since optic atrophy is simply a finding, not a diagnosis, it is the clinician’s responsibility to provide a definitive explanation and if necessary, conduct a further investigation to determine the etiology.
Among the many causes of optic nerve pallor, traumatic optic neuropathy (TON) is relatively benign and non-progressive. Upon further questioning, patients with suspected TON will have a positive history of direct/indirect trauma to the head/orbit/eye. These patients, however, may not be aware of any changes to their vision. In this article, we’ll explore the clinical manifestations and management for patients presenting with TON.
Pathophysiology
Traumatic optic neuropathy occurs when the optic nerve transitions from being normal and functional to having a pale/atrophic appearance. This can occur weeks to months after a direct/indirect traumatic event. This process is thought to be multifactorial and can result in highly variable visual outcomes for the patient.
TON is a relatively uncommon cause of vision loss in cases of blunt trauma and affects up to 2.5% of individuals with a history of trauma. The prevalence of TON in the general population is approximately one per 1,000,000. The majority of patients affected with TON are young adult males in their thirties. Common causes can include motor vehicle accidents, falls, and/or assaults.
Traumatic stress to the head/skull tends to concentrate at the optic canal, causing anatomical disruption to the optic nerve and shearing forces to the retinal ganglion cell (RGC) axons. This results in recession and loss of the micro-capillary networks that supply the optic nerve and remaining RGC axons. An atrophic appearance to the neuroretinal rim is the eventual result of this process.
Trauma can also cause swelling and ischemia within the tight space of the optic canal. This process further contributes to the irreversible loss of RGC axons, and leads to apoptotic cell death of the neuroretinal rim.

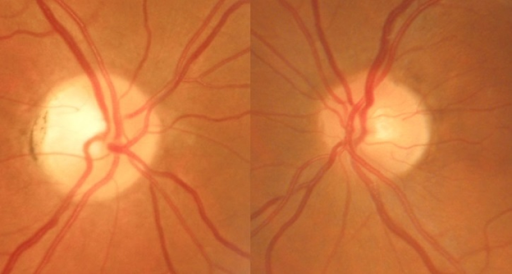
Figure 1: Traumatic optic neuropathy in the right eye of a 56 y/o female patient with positive history for head trauma
Diagnosing TON
Making a Diagnosis
The diagnosis of TON is usually straightforward based on clinical presentation and a thorough case history. Some patients will confirm longstanding decreased vision in one eye from a past ocular injury or trauma. In other cases, patients may be completely asymptomatic for any vision loss, despite the presence of optic atrophy.
Visual outcomes can be highly variable in TON cases, with visual acuities ranging from 20/20 to light perception. As many as 60% of patients with TON will present with light perception (or worse) visual acuity at baseline. It is crucial to conduct formal visual field testing, preferably a 30-2 field, to determine the extent of vision loss. Visual field results can be highly variable, often with no regard for fixation nor for respecting the vertical vs. horizontal meridians (as compared to other pathologies of the optic nerve). Patients with TON will also likely have compromised color vision/red desaturation testing as well.
With the exception of bilateral TON cases, a relative afferent pupillary defect (RAPD) will always be present. In mild TON cases where frank optic neuropathy is not clinically detectable, a RAPD may be subtle. The presence of a RAPD can also precede optic neuropathy in the initial period following trauma.
Unless a traumatic pupil-involving third nerve palsy is suspected (warranting neurosurgical monitoring of the pupil), patients with ocular trauma should always have a dilated ocular health assessment. This ensures the clinician can rule out the presence of vitreous/retinal hemorrhages, retinal tears/detachments, and in cases of penetrating injury, an intraocular foreign body.
The presence of optic nerve pallor in TON typically manifests clinically around six weeks post-injury. In addition to sectoral/diffuse optic atrophy, large wedge defects in the retinal nerve fiber layer (RNFL) can also be appreciated. Using a red-free filter during biomicroscopy/fundus photography can also help clinicians better appreciate RNFL dropout when assessing optic nerve pathologies like TON.
It is important for clinicians to differentiate optic nerve cupping from atrophy. Vertical cupping of the neuroretinal rim is classic with glaucomatous optic neuropathy, and tends to occur only in rare cases of non-glaucomatous optic neuropathy. The presence of optic atrophy is rare in glaucoma and typically only occurs with end-stage disease.
Optic nerve pallor secondary to trauma isn’t always easy to distinguish, especially when assessing the fundus through media opacities like a dense cataract. It is also important to distinguish true optic nerve pallor from physiologic variations of normal. Myopic/tilted discs, optic nerve drusen, and myelinated nerve fiber layers can also create the illusion of rim pallor or cupping. In some cases, requesting/reviewing old optometry/ophthalmology records from the patient’s last exam can be helpful to clarify exam findings.
Pseudophakic patients may also appear to have optic nerves that are slightly more pale and atrophic than usual. This phenomenon, referred to as “pseudophakic pseudo pallor,” is caused by the alteration in light filtration between the natural lens and the lens implant after surgery. In these cases, the temporal rim tends to be lighter than the rest of the disc.
Communicating with TON patients
When diagnosing traumatic optic neuropathy it is important to confirm the traumatic event by taking a thorough case history. Unfortunately, many TON cases involve a history of abuse and domestic violence. Do not be surprised if patients initially deny a history of trauma or even become emotional in your chair as they recount their past. Many patients with TON may not correlate their past trauma with their vision, especially if their central acuity remains satisfactory.

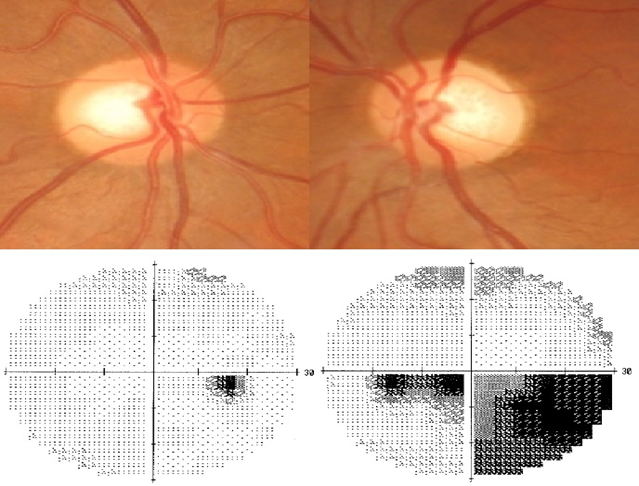
Figure 2: Traumatic optic neuropathy of left eye in 47 y/o female with history of head trauma from motor vehicle accident and domestic violence. Visual field patterns in TON can be highly variable without regard for horizontal vs. vertical meridian.
Management and treatment of TON
Treating TON patients
The majority of eye care practitioners today opt to manage TON cases conservatively, usually with observation alone. Given the lack of randomized control trials pertaining to treatment modalities for traumatic optic neuropathy, definitive treatment for TON remains controversial. Other treatments like surgical decompression and high dose corticosteroids have also been studied in the literature. Final visual outcomes with these other interventions are similar to observation alone. Given the high risk for potential adverse side effects with other treatment modalities, they are typically avoided.
In managing TON, it is important to document everything. Initially, it may be necessary to follow patients on a weekly/monthly basis. When confirming a diagnosis of TON, recording a detailed case history is essential. Serial clinical testing confirms the diagnosis and helps determine visual prognosis and final visual outcome. Important tests include visual acuity and pupil testing, optical coherence tomography (OCT), fundus photography, and Humphrey 30-2 visual fields.
Obtaining a thorough case history and documenting all clinical findings is very important, as TON cases may involve future medicolegal proceedings (e.g., domestic violence cases)

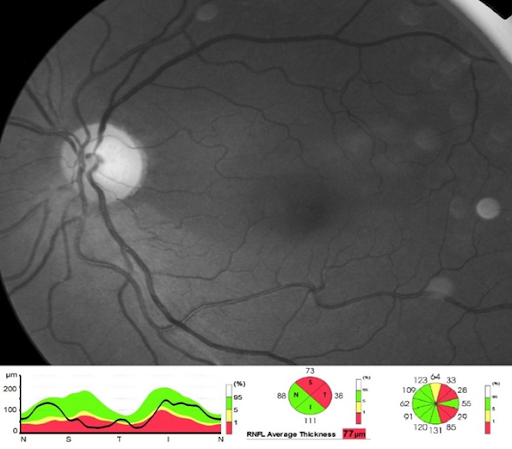
Figure 3: Diffuse RNFL dropout superiorly in left eye TON. Red-free fundus photos can also help reveal RNFL dropout and tends to correlate well with optical coherence tomography in TON.
The decision to order neuroimaging is highly debatable in cases of TON. The consensus is highly variable among eye care practitioners worldwide. In the past, clinicians have been known to order imaging to rule out optic canal fractures and help determine potential candidates for surgical decompression.
While surgical decompression has been shown to improve visual outcomes in some TON patients (no-light-perception vision at baseline) it is generally not a first-line treatment. In general, decompression surgery has not been shown to improve visual outcomes in most TON cases as compared to more conservative treatment approaches (e.g., observation alone).
Based on the National Acute Spinal Cord Injury Study (NASCIS) in the 1990s, intravenous steroids were found to improve motor function in patients with acute spinal injuries. Shortly after, these results were extrapolated and applied to TON treatment.
The International Optic Nerve Trauma Study (IONTS) is the largest prospective multicenter TON study to date, closely following the NASCIS. It concluded that treatment with both surgical decompression and/or corticosteroids did not provide any additional benefit to final visual recovery over observation alone. In fact, of the three treatment groups, those untreated (observation alone) had the best visual recovery. Given the relatively high rate of spontaneous visual recovery with indirect TON cases, it has been concluded that neither surgery nor corticosteroids should be considered standard of care treatment.
The Corticosteroid Randomization for Acute Head Trauma (CRASH) trial also showed an increased risk of adverse systemic events (including death) in trauma patients treated with corticosteroids. In animal models, treatment for TON with corticosteroids has been shown to further exacerbate axonal loss in the optic nerve. Therefore, corticosteroid treatment remains highly controversial and is typically avoided.
Roughly half of indirect TON cases managed with observation alone will have some recovery in vision. Visual acuity at baseline is the best predictor of final visual outcome. Other factors that correlate with poor visual recovery include a loss of consciousness, no improvement in vision 48 hours post-trauma, optic canal fractures, and absence of visual evoked responses.
Conclusion
Given the potentially high stakes of unexplained optic nerve pallor, it is crucial for the clinician to determine a definitive diagnosis. It is important to always obtain a thorough case history in the presence of optic atrophy and rule out a history of trauma. Clinicians must also be mindful of other causes of primary/secondary optic atrophy in their workup. Drug-related/toxic, NAION/ischemia, optic neuritis, are all among other common etiologies for optic atrophy. Of the myriad of causes for optic atrophy, TON is a relatively benign, non-progressive diagnosis.
Given the lack of convincing evidence showing improved visual outcomes with active intervention, most eye care practitioners today typically opt for conservative management in cases of non-progressive traumatic optic neuropathy.
