


For this month’s issue, I’m going to switch gears from retinal disease to optic nerve disease. Though glaucoma is the most common optic neuropathy, there are many glaucoma masqueraders that we must be aware of. These are conditions that mimic glaucoma but are separate disease processes that require their own management approach.
When examining a glaucoma suspect (or a glaucoma patient transferring care) it is always important to remember the question isn’t whether or not this patient has glaucoma but whether or not this patient has an optic neuropathy. Once you have determined that an optic neuropathy is present, you must decide if the optic neuropathy is glaucoma or one of the many non-glaucomatous optic neuropathies.
The work-up for non-glaucomatous optic neuropathies is massive and beyond the scope of this article, but the methods to differentiate glaucoma from non-glaucomatous disease is thankfully much shorter.
Taking a comprehensive approach to optic nerve disease
First, it is important to understand that the management of any optic nerve disease requires a comprehensive approach including clinical findings, OCT imaging, and visual field testing. Glaucoma is a (usually) slowly progressive optic neuropathy with characteristic findings of cupping and corresponding OCT and visual field defects.
As seen in Figure 1, cupping will correlate with both the location and magnitude of RNFL OCT thinning. Visual field defects tend to lag behind RNFL OCT findings in early and moderate glaucoma patients but then overtake RNFL OCT findings in advanced cases. In glaucoma, RNFL OCT defects tend to affect the superior-temporal and inferior-temporal areas which correlate with inferior-nasal and superior-nasal visual field defects. Visual field defects begin as nasal steps, gradually progressing to arcuates and then altitudinal defects.
Glaucomatous visual field loss will always respect the horizontal meridian as this is the location of the horizontal raphe. Ganglion cell thickness measurements will correspond with the RNFL OCT and visual field changes, beginning on the temporal side of the fovea and progressing to the nasal side with worsening disease.

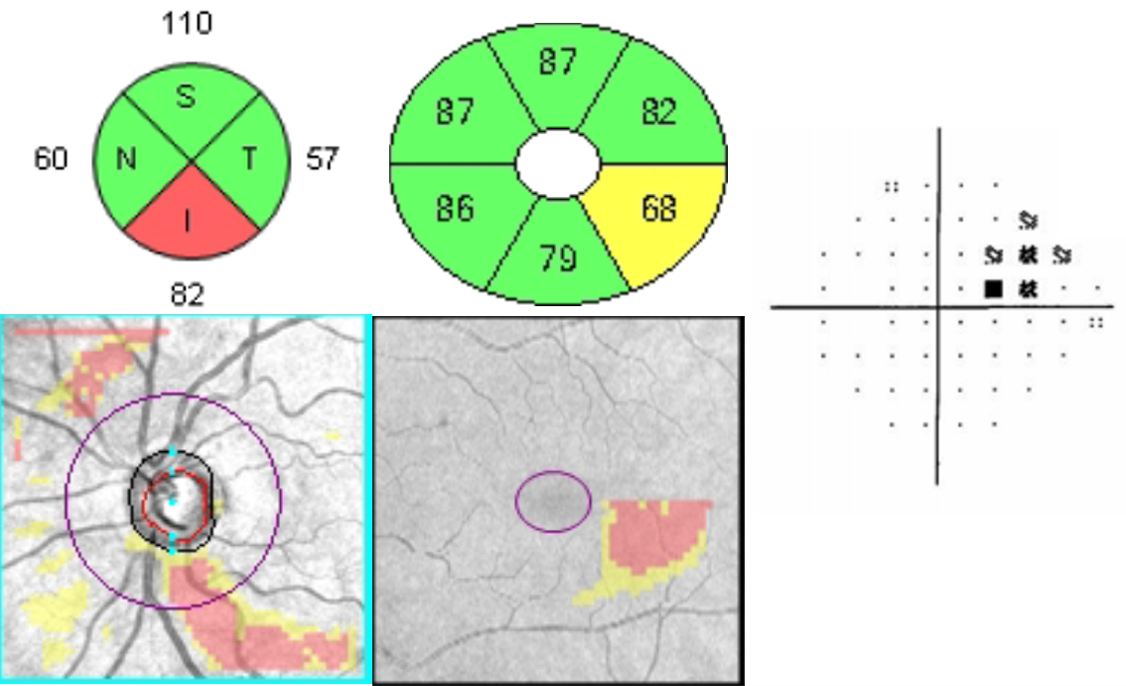
Figure 1
Ruling out retinal disease with OCT
Before diagnosing a primary optic nerve disease such as glaucoma or chiasmal compressive optic neuropathy, it is important to rule out retinal disease as a causative factor.
Figure 2 depicts a patient with moderate cupping and a superior-temporal chorioretinal scar. The scar has led to a consecutive optic neuropathy where local ganglion cell loss produces axonal atrophy. Co-localizing ganglion cell and RNFL OCT defects are noted superiorly but the thinnest ganglion cell sector is superior to the fovea instead of temporally. This discordance alerts us that the corresponding RNFL, ganglion cell, and visual field defects may be of non-glaucomatous nature which is easily confirmed with our funduscopic evaluation.

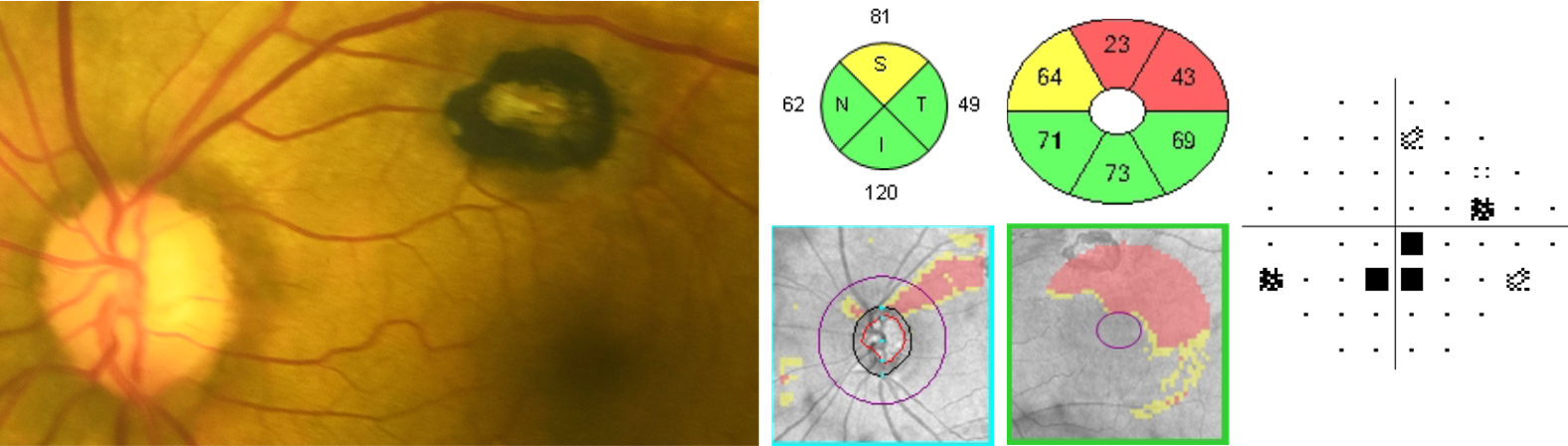
Figure 2
In its acute phase, non-arteritic ischemic optic neuropathy (NAION) is impossible to confuse for glaucoma. The acute vision loss, presence of an APD, and optic nerve head swelling will easily rule out glaucoma. But in its chronic phase, with hemispheric RNFL, ganglion cell, and visual field defects, NAION may mimic glaucoma.
The patient in Figure 3 presented for a diabetic ocular examination and was noted to have moderate cupping and pallor OS. The patient had 20/25 vision and an APD in the left eye but denied any visual symptoms or history of acute vision loss. RNFL OCT thinning was noted superior-temporally but ganglion cell thinning was noted superiorly and inferiorly. Visual field testing revealed an inferior altitudinal defect with superior central defects which correlated with the ganglion cell defects.
Both the visual field and ganglion cell defects were out of proportion to the RNFL OCT thinning. The presence of pallor should immediately raise suspicion of a non-glaucomatous process and the discordant imaging results further compound this suspicion. After requestioning the patient and requesting old records, it was clear that the patient had an episode of NAION years ago and the current findings were all sequelae of that event. Due to the presence of old records, further evaluation was not necessary and the patient was monitored for stability.

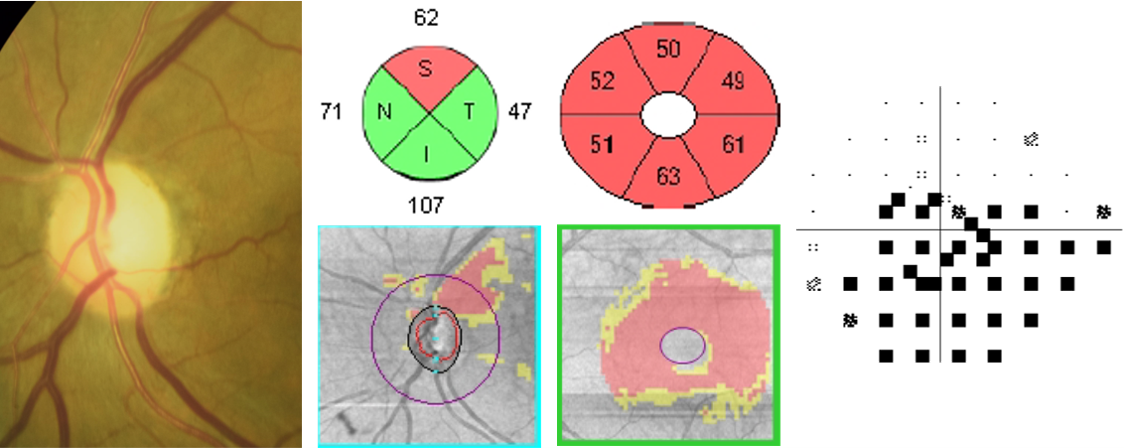
Figure 3
Optic nerve head cupping is sometimes thought to be a pathognomonic sign of glaucoma, but any anterior visual pathway disease can cause cupping. Especially in younger patients, it is important to rule out chiasmal compressive optic neuropathy as this is an uncommon cause of bilateral cupping that must be treated immediately.
The images in Figure 4 are of a 52-year-old patient who was transferring glaucoma to my clinic. She reported being treated with latanoprost QHS OU for several years and denied any ocular issues. Her BCVA was 20/25- in each eye and there was no APD. She did have large cups with significant RNFL and ganglion cell OCT thinning but both tests had more prominent loss on the nasal side. Visual fields revealed distinct bitemporal defects which respected the vertical meridian. An MRI of the pituitary gland was ordered and radiological signs of a macroadenoma were noted.
The patient had prompt neurosurgery but her visual field defects and mildly reduced visual acuity did not recover. Due to the likely chronicity of her chiasmal disease, the ganglion cells had atrophied as denoted by the OCT ganglion cell analysis. In cases of any compressive optic neuropathy, visual field defects tend to appear before OCT findings. Ganglion cell OCT measurements are particularly useful for prognostic purposes because atrophy of ganglion cells tends to be permanent and appears after visual field defects but before RNFL OCT thinning.


Figure 4
Posterior visual pathway disease can often be tricky to diagnose because the clinical exam can be completely normal. Unlike anterior visual pathway disease, posterior disease will not cause cupping and will rarely cause optic nerve head pallor. There will be no APD because the disease is bilateral and vision may be unaffected. Figure 5 illustrates a 47-year-old who was referred for a glaucoma evaluation. His vision was 20/20 OU, pupils unremarkable, and confrontation visual fields full. He did have moderate cupping, more so in the right eye, which correlated with the more pronounced RNFL OCT thinning of the right eye.
There were corresponding ganglion cell defects worse in the right eye than the left. Visual field testing revealed an inferior partial arcuate in the right eye which correlated with the rest of the findings. But it was the visual field results of the left eye which raised suspicion that this was not a glaucomatous process. The left visual field defects were most prominent inferior-temporally, a very atypical finding in glaucoma but a common finding in parietal lobe disease.
An MRI of the brain was ordered and a right parietal lobe lesion consistent with lymphoma was discovered. The patient received prompt chemotherapeutic therapy and maintained his asymptomatic 20/20 vision.

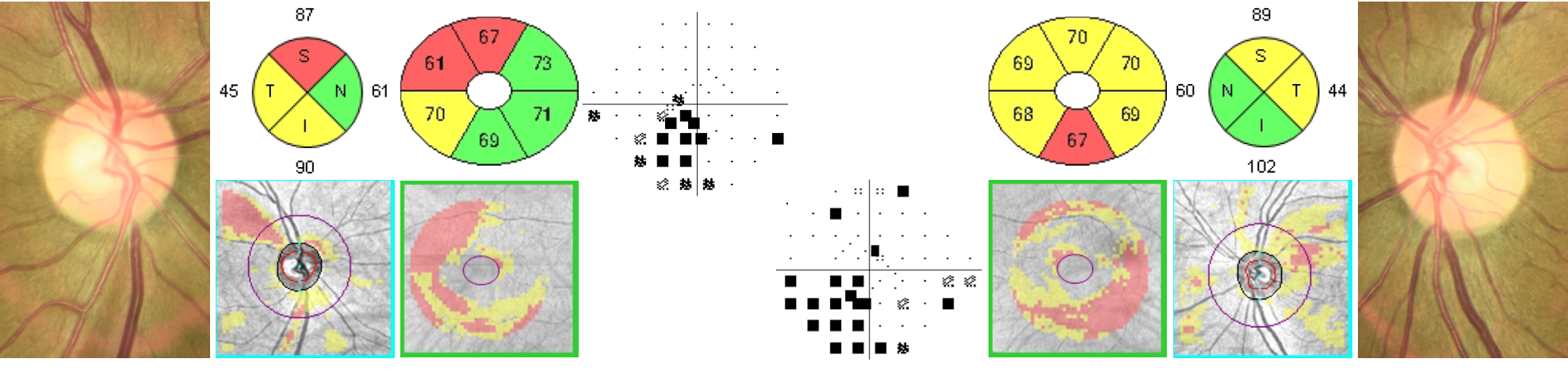
Figure 5
83% of optometrists who treat glaucoma rank their knowledge of minimally invisible glaucoma surgery a 6.16 out of 10.* Are you one of them? Boost my understanding >>
Source: 2022 Glaucoma Report
Final notes
Glaucoma is a relatively common optic neuropathy that all eyecare providers will come across in their clinics. It is important to perform a thorough history and acquire a full diagnostic ocular imaging panel before diagnosing glaucoma. In glaucoma, RNFL OCT thinning tends to initially affect the superior-temporal and inferior-temporal regions of the optic nerve head. This will correlate with ganglion cell thinning of the temporal macula which eventually encompasses the whole hemisphere. Visual field defects will be most prominent on the nasal side and always respect the horizontal meridian.
Every clinician should always have a healthy suspicion for non-glaucomatous optic neuropathy, but patients who break the above diagnostic tendencies should be especially scrutinized to ensure proper diagnosis.
