




According to the most recent worldwide consensus definition, “dry eye” is a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.”1
While estimates are difficult to confirm given the extent of currently undiagnosed and self-managed cases, a recent systematic review found that the pooled prevalence of dry eye disease was 17.4% (95% confidence interval [CI], 8.9% to 31.4%; 13,546,368 participants) across 10 studies judged to be representative of the population in the United States.2
Extrapolation of that value to the overall US population suggests that roughly 58 million Americans suffer from dry eye in some capacity. If we ascribe this population to the current number of eyecare providers in the US (approximately 45,000), it amounts to nearly 25 dry eye patients per practitioner per week, making dry eye disease one of the most common maladies seen in practice today.
Recognizing and classifying dry eye disease
The symptoms of dry eye disease are by now well-known to eyecare providers. Patients with dry eye may report:3
- Burning
- Dryness
- Itching
- Stinging
- Grittiness
- Scratchiness
- A sandy-feeling or foreign body sensation in the eyes
- Photophobia
- Intermittent blurriness
- Heavy or tired eyes
- Discomfort when performing activities that require prolonged focus (e.g., reading, driving, computer use, watching television)
Unfortunately, these symptoms are all relatively nonspecific and can overlap with a host of other ocular surface disorders. Likewise, the clinical signs of dry eye disease are also non-specific; for example, conjunctival hyperemia is characteristic of inflammation, which may be a sign of dry eye disease or a number of other conditions, including allergy, infection, or inflammation from systemic causes. Additional signs may include excessive or incomplete blinking, tearing, or blepharospasm.
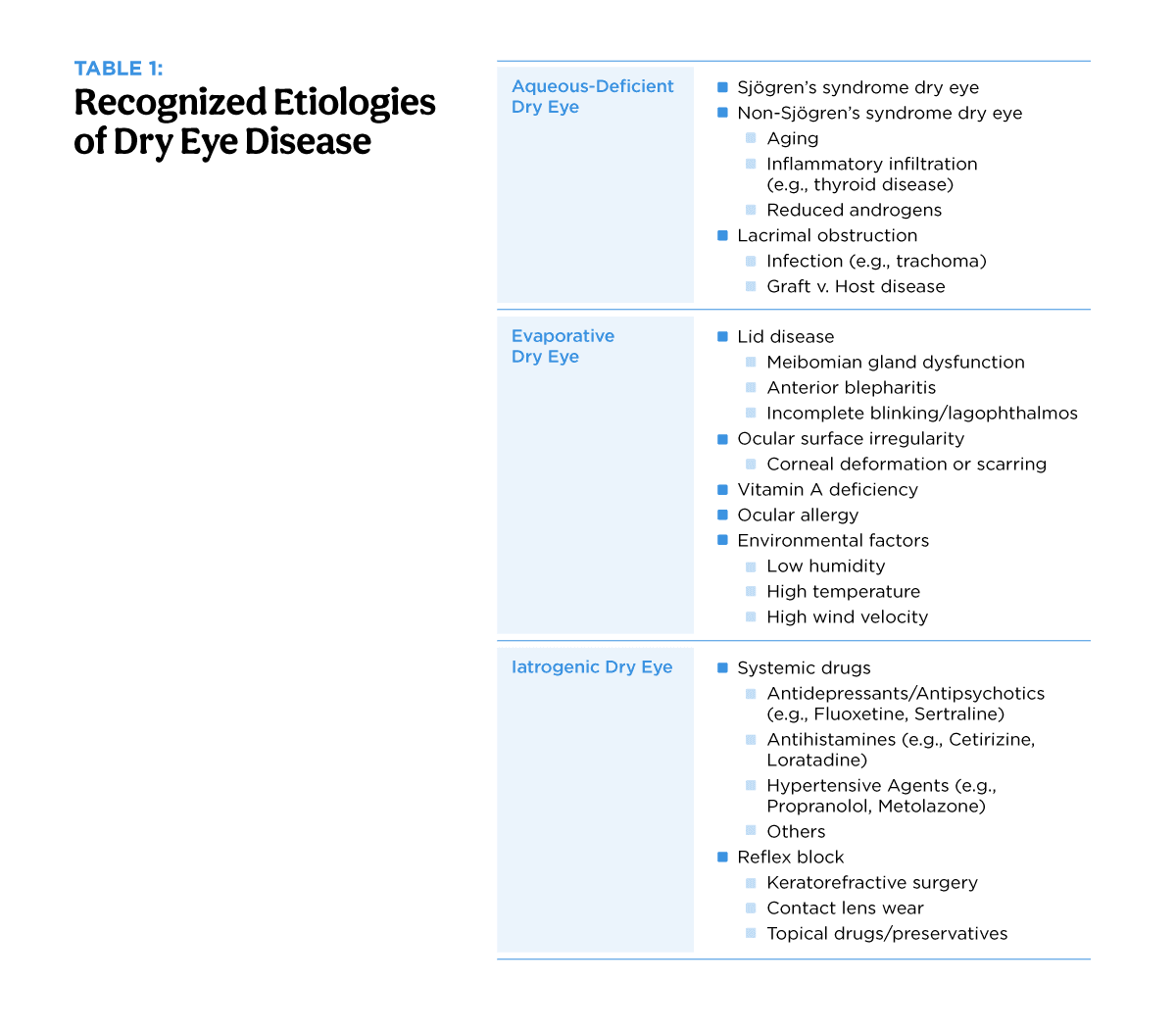
Our current understanding of dry eye disease recognizes two broad etiological subtypes: (1) aqueous-deficient dry eye and (2) evaporative dry eye.1,4,5 While we assume that both of these subtypes are driven by tear film instability and associated with excessive tear hyperosmolarity, the pathophysiology by which this clinical state is reached differs according to etiology.
More specifically, hyperosmolarity in aqueous-deficient disease is thought to be due to diminished lacrimal production, causing a higher concentration of salts, ions, and other components in the tears.1 Alternatively, evaporative dry eye begins with a normal volume of lacrimal gland secretions, but excessive evaporation from ocular surface disease results in tear film hyperosmolarity.4,6
Addressing evaporative dry eye
Despite the two categories described, the clinical distribution of aqueous-deficient and evaporative dry eye are far from equal. Current literature acknowledges that “an evaporative component to dry eye disease is more common than an aqueous deficient component. Indeed, meibomian gland dysfunction (MGD), a primary contributor to evaporative dry eye, is considered the leading cause of dry eye in clinic- and population-based studies.”7,8,9,10
Today, we understand that most clinical cases demonstrate some degree of evaporative element, with a diagnosis of MGD (or a combination of MGD and aqueous deficiency) present in at least 50% and perhaps as many as 86% of those with dry eye disease.7,11,12,13
In addition to MGD, evaporative dry eye may be potentially related to incomplete lid closure, diminished blink frequency or quality, or simply an abnormally large palpebral aperture; additionally, it may be attributable to other ocular surface-related issues, including mucin deficiency and/or contact lens-related problems.1,14,15 For this reason, appreciating the role of evaporation in dry eye disease is crucial when considering the wide range of therapeutic management approaches.
Table 1: List of some of the more common etiologies of dry eye disease.

Managing dry eye disease
Determining which therapy or therapies are most appropriate for a given patient must be predicated via a comprehensive diagnostic assessment. As stated, the vast majority of patients have more than one contributor to their dry eye disease. While MGD is extremely common, lid laxity and corneal nerve abnormalities are also frequently encountered.
Dry eye must also be considered within the context of co-morbid ocular conditions such as glaucoma, thyroid eye disease, or prior laser vision correction. Finally, lifestyle contributors to ocular surface disease must also be addressed and managed. Thus, it is unusual that a single treatment in isolation can be entirely effective at controlling dry eye.
As a general rule of thumb, experts suggest aligning the initial treatment to the specific type or etiology of dry eye disease. For example, if inflammation is evident, anti-inflammatory therapies (e.g., corticosteroids, cyclosporine, lifitegrast) are typically indicated as a first- or second-line therapy.
Similarly, if the patient clearly manifests evaporative dry eye due to MGD, then therapy aimed at restoring the integrity of the meibomian glands and replenishing the tear lipid component becomes paramount. Several years ago, this could only be accomplished by using mechanical procedures to help evacuate the glands, but today, we have additional options available, including pharmaceutical agents.

We are fortunate that medications with novel mechanisms of action that go beyond anti-inflammatory effects have made it into the marketplace, and each is well-positioned to improve our ability to provide multimodal therapy.
Varenicline solution nasal spray
Varenicline is an older medication that, in systemic form, has historically been used for smoking cessation. It is a partial agonist of the α4β2 nicotinic acetylcholine receptor (nAChR), which is the primary receptor subtype involved in nicotine addiction.16
By binding and partially activating this receptor, dopamine is released, which in turn helps reduce nicotine cravings by mimicking some of the effects of nicotine intake. Moreover, when a person smokes, varenicline is already bound to the nicotinic receptor, preventing the dopamine surge that makes smoking pleasurable.
In dry eye disease, varenicline acts by binding to nAChRs on the trigeminal sensory nerves, which stimulates the parasympathetic innervation of the lacrimal functional unit. Varenicline enhances basal and reflex tear secretion, helping to alleviate dry eye symptoms.17,18,19 Unlike systemic cholinergic agents like pilocarpine, however, varenicline targets nAChRs selectively without significant muscarinic side effects (e.g., sweating, salivation).16
Varenicline’s unique ability to directly stimulate the lacrimal functional unit offers significant advantages. While it can be effective as step therapy, it works very well for patients who have moderate dry eye as well. It also begins to work quickly, between 2 to 4 weeks in published studies.17,18,19

Because the dose of locally administered varenicline is much lower than the oral medication (which has some potential neuropsychiatric side effects), it is a safe medication for most patients. Common side effects include sneezing (~82%), nasal irritation (~16%), cough (~5%), and throat irritation (~3%).20 Less common side effects include dysgeusia, headaches, and excessive tearing, while rare side effects may include a runny nose, fatigue, or nausea.20
As with all medications, discussing the potential side effects with patients before initiation of therapy and then following up several weeks to months after initiation to assess the side effect profile is often effective in managing any negative reactions.
Case report: TYRVAYA (varenicline solution nasal spray)

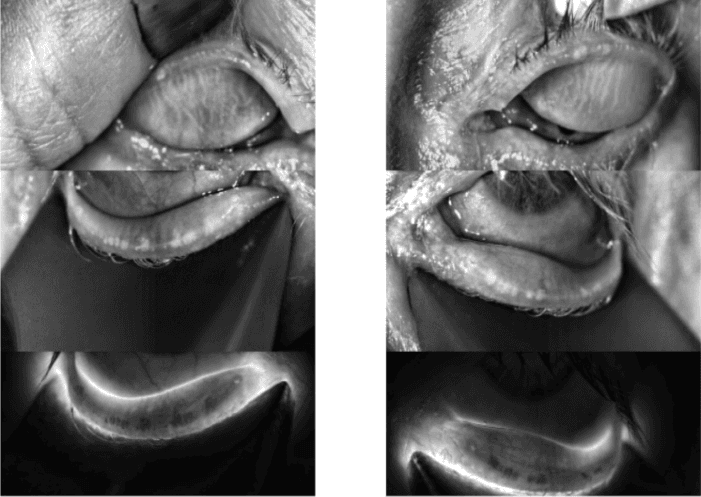
Figure 1: Courtesy of Amy Nau, OD, FAAO.
A 63-year-old white female presented with a history of longstanding MGD, with evidence of significant atrophy OU, nocturnal lagophthalmos OU, and corneal hyperalgesia OU with corneal nerve changes confirmed by in-vivo confocal microscopy. Her ocular history was also positive for lens pseudoexfoliation without glaucoma OU, as well as mild cataracts OU.
A dry eye-focused evaluation revealed the following:
- SPEED symptom questionnaire: 15/28
- MGYLS with meibomian gland expression: <5 per eyelid
- Corneal staining: (-) sodium fluorescein, (-) lissamine green
- Conjunctival staining: (-) lissamine green, (-) lid wiper epitheliopathy, (-) superior limbic keratoconjunctivitis
- Fluorescein tear breakup time (FTBUT): OD 7s, OS 8s
Therapy at the time of presentation consisted of the following:
- Punctal plugs OU (lower lids only)
- 30% serum tears 6 times daily OU
- 0.5% loteprednol etabonate twice weekly OU
- Sleep mask QHS
- Irrigation with non-preserved saline every morning OU
- Moisture chamber glasses PRN
- Manual meibomian gland expressions - 15 times since 2016
- Intense pulsed light (IPL) - every ~4 months since 2020
Failed past therapies included:
- Mechanical neurostimulation (TrueTear; caused irritation and bleeding)
- Topical cyclosporine (3 brands; caused burning)
- Topical lifitegrast (ineffective and caused dysgeusia)
- Thermal pulsation (not perceived as effective)
- Testosterone eye drops (unaffordable)
This patient displayed increasing symptoms on SPEED as well as reduced FTBUT and clear evidence of advanced MGD, with multiple failed therapies. We prescribed varenicline solution nasal spray twice daily, based on the prior poor efficacy and tolerability of topical eye drops combined with the reported benefit of mechanical nasal stimulation despite adverse reactions.
Upon follow-up 2 months later, her SPEED score had decreased to 6/28, while her ocular surface remained stable.
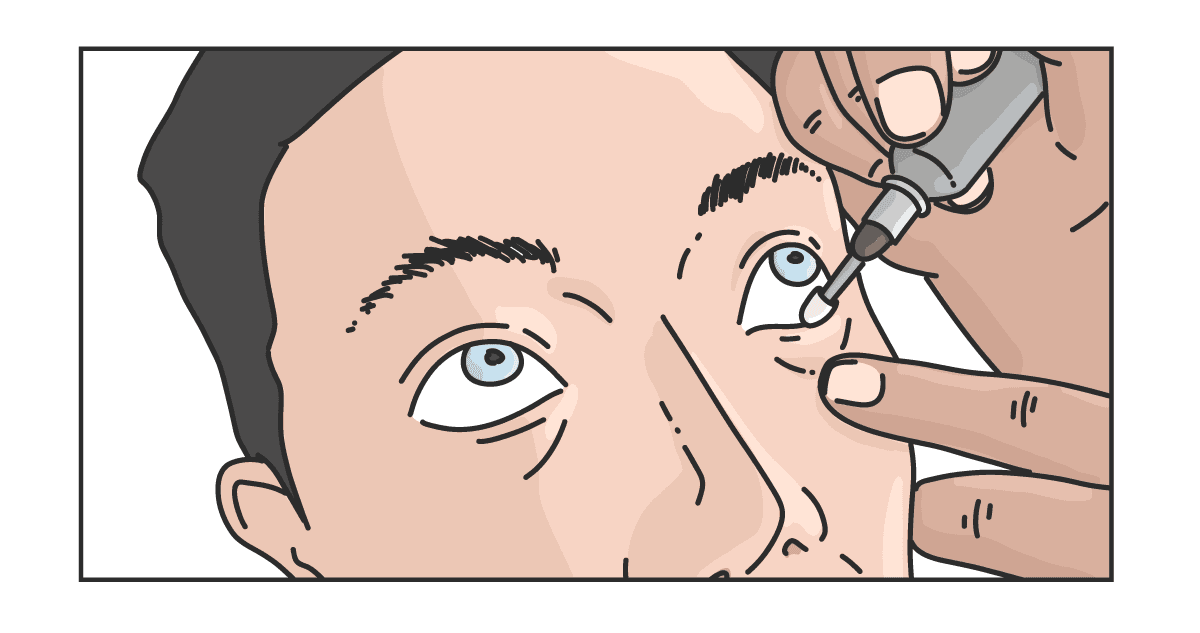
Perfluorohexyloctane ophthalmic solution
Perfluorohexyloctane was introduced in Europe in 2017 and the US in 2023, where it is marketed as a drug specifically targeting the evaporative component of dry eye, which is commonly associated with meibomian gland dysfunction. It is sold as a single-ingredient medication without the addition of water or preservatives and has been shown to last up to 4 to 8 hours on the eye.21
Perfluorohexyloctane has amphiphilic properties, containing both aerophilic and lipophilic segments that interact with the oxygen-rich external environment and lipid layer of the tear film, creating an additional layer that prevents evaporation.22,23,24,25,26
It also has low surface tension, allowing it to spread more efficiently over the ocular surface.27,28 Finally, it may offer some indirect anti-inflammatory effects by providing an enhanced protective barrier over the ocular surface.
Because of its anti-evaporative properties, perfluorohexyloctane is an excellent option for patients in virtually all stages of dry eye disease. Even if the lipid layer is very low or non-existent, this medication may still confer some advantages as it acts as a surrogate.29
In the US market, it is recommended not to use perfluorohexyloctane while wearing contact lenses, with instructions to remove contact lenses before instillation and to wait 30 minutes before reinsertion after use.
Perfluorohexyloctane is, by definition, a semi-fluorinated alkane (SFA), putting it in the category of PFAs or “forever chemicals.” However, because it is physically, chemically, and physiologically inert, it is highly stable in the environment, so it will not biodegrade.30,31
Additionally, because it is a small molecule, it has low systemic absorption and, therefore, is less likely to bioaccumulate in ocular tissues and shows undetectable blood levels after use.32 Understandably, some patients may express concern about this feature of perfluorohexyloctane, and we must be ready to address any concern, especially as fluorinated compounds are widely used throughout medicine today (contact lenses, inhalers, etc.).33,34
Case report: MIEBO (Perfluorohexyloctane ophthalmic solution)
A 30-year-old Hispanic male presented with a work history that included 12 to 14 hours of daily screen time, along with high hyperopia and esophoria managed by way of neuroadaptive spectacle lenses (Neurolens; Coppell, TX). He reported significant ocular discomfort, especially toward the end of the day.
A dry eye-focused evaluation revealed the following:
- SPEED symptom questionnaire: 14/28
- MGYLS with meibomian gland expression: <1 per eyelid
- MGD severity: Obstructive MGD with <25% atrophy
- Corneal staining: (+) grade 2 inferiorly, OU
- Conjunctival staining: (+) grade 1 lid wiper epitheliopathy OU
- MMP-9 levels: Strongly positive (+) MMP-9 marker (InflammaDry; San Diego, CA) OU
Therapy at the time of presentation consisted of the following:
- Electric heat mask QHS
- Hypochlorous acid foam twice weekly OU
- Lipid-based artificial tear drops TID or more PRN
- In-office therapies (e.g., microblepharoexfoliation and thermal pulsation) had been recommended, though the patient was reluctant to engage
Based upon the significance of this patient’s MGD and physical symptoms, we prescribed perfluorohexyloctane QID, while simultaneously reducing his artificial tear use to BID OU. Upon follow-up 2 months later, his SPEED score had improved to 8/28. Additionally, his lid wiper epitheliopathy had completely resolved, as had the corneal staining in his right eye. Corneal staining in the left eye also improved by >50%.
Preventative eyelid cleaning techniques
Both MGD and blepharitis are extremely common disorders of the eyelids. Microbial overgrowth and accumulation of biofilm can naturally occur on the lid margins and, over time, cause inflammation.35,36
Despite these facts, recommending preventative eyelid cleaning starting from a young age is not yet the standard of care, as it is with tooth and gum care in dentistry. As a result, patients often present with moderate to severe eyelid disease, which can have deleterious consequences on the ocular surfaces.
Thermal pulsation was the first commercially available device to treat MGD, receiving FDA approval in 2011, though other technologies to care for the meibomian glands and eyelids quickly followed.
While each of these treatments occupies a niche in the realm of eyecare, the end goal for all is similar: improvement of eyelid health and rehabilitation of meibomian gland function. A summary of the commercially available technologies for the treatment of eyelid disease and MGD is presented below.
Microblepharoexfoliation

Simply put, microblepharoexfoliation may be defined as removing debris (biofilms, desquamated epithelium, collarettes/Demodex mites, and cosmetics) from the lashes and lid margin. The mechanism of action involves the removal of debris, harmful biofilms, and excessive amounts of bacteria, which, over time, can cause an inflammatory cascade.37
If done frequently, this technique can be extremely effective at keeping inflammation at bay and maintaining patent, flowing meibomian glands that may otherwise be obstructed by the buildup of debris on the lid margin.
To some extent, patients can perform microblepharoexfoliation at home with their finger, a cotton-tipped applicator, or a lid wipe made specifically for eyelid cleansing (commonly called “lid scrubs” in the common vernacular). However, there are also several electrical devices that can provide more thorough cleanings, particularly when performed by a trained provider as an in-office procedure.
Microblepharoexfoliation should be advocated for early in life, starting in middle school. It is well-established that children now experience dry eye disease due to prolonged screen time (the average is 7 hours per day for teenagers, and 40% of toddlers have their own tablet device by the time they are 2 years old).38,39
At-home therapy, coupled with occasional in-office deeper cleanings, should be considered preventative care and not necessarily a dry eye “treatment.” Microblepharoexfoliation, performed by capable hands, carries no recognized adverse events other than the potential for mild conjunctival or corneal abrasion.
Intense pulsed light therapy (IPL)

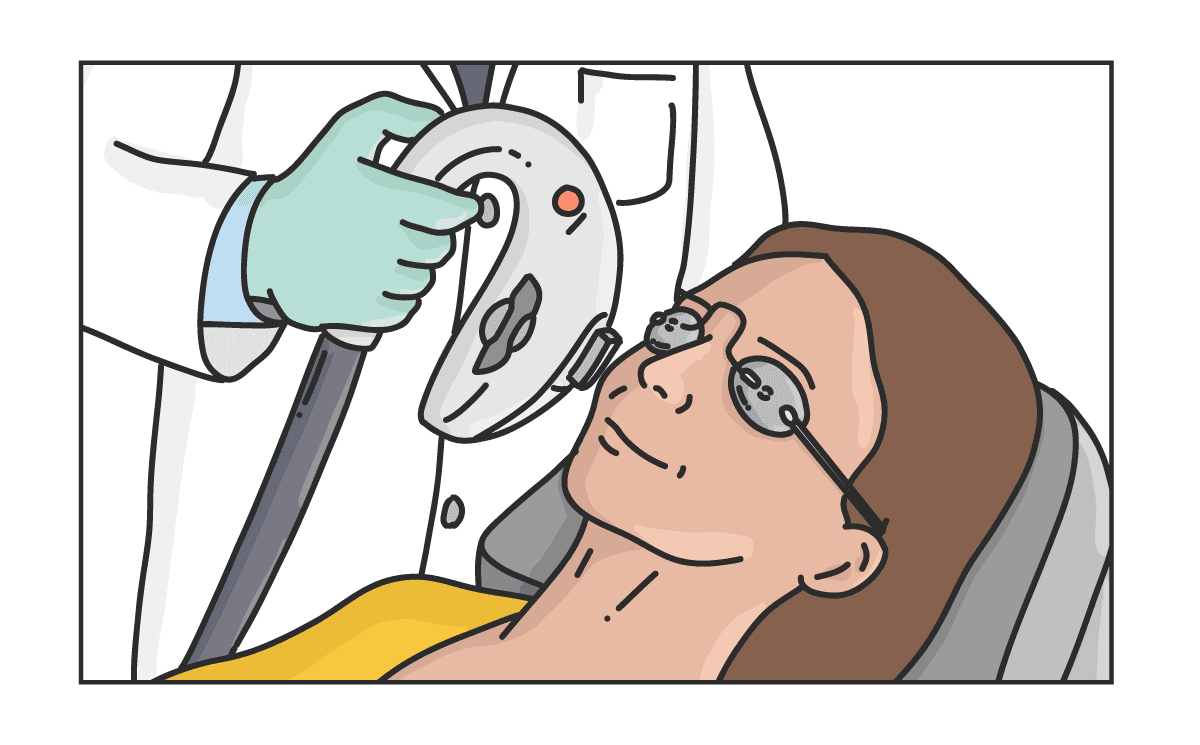
Intense pulsed light uses broad-spectrum light and several filters that allow eyecare providers to target specific chromophores to treat eyelid disease.40 One mechanism of action of IPL is photobiomodulation, which enhances cellular function and reduces inflammation.41
Additionally, IPL is capable of reducing the population of potentially pathogenic bacteria and Demodex mites present through coagulation necrosis.42,43 Because the filters used allow for the selective targeting of blood vessels, lid margin telangiectasias can regress over time as well, reducing the volume of inflammatory mediators reaching the eye and adnexa.40,44
By enhancing cellular function and addressing harmful microbes and inflammation, rehabilitation of the meibomian glands is enabled.45 It is also beneficial to express the meibomian glands; however, the use of multimodal therapy with other dedicated heating devices is recommended, as this will enhance the evacuation of stagnant meibomian gland contents.
IPL is best suited for patients with MGD, Demodex, rosacea, and/or lid margin telangiectasis. In my experience, four to six sessions scheduled 2 to 5 weeks apart is usually the minimum needed for patients to start experiencing relief, so it is best to inform the patient that IPL therapy may take up to 6 months to have an effect.
Waiting until these conditions become entrenched makes it harder to achieve optimal results. Therefore, while it can be effective even in severe cases, IPL should be considered even at the mildest stages to prevent disease progression.
While some IPL devices can be used in patients with darker skin tones, this must be done with extreme caution due to the potential for burning/blistering or skin pigmentation changes.
There are also restrictions on the use of retinoids, neurotoxins, fillers, and other laser-based facial rejuvenation procedures, as well as sun exposure proximal to getting IPL. Heavy exercise and the use of facial exfoliants are contraindicated for 24 hours after the procedure.
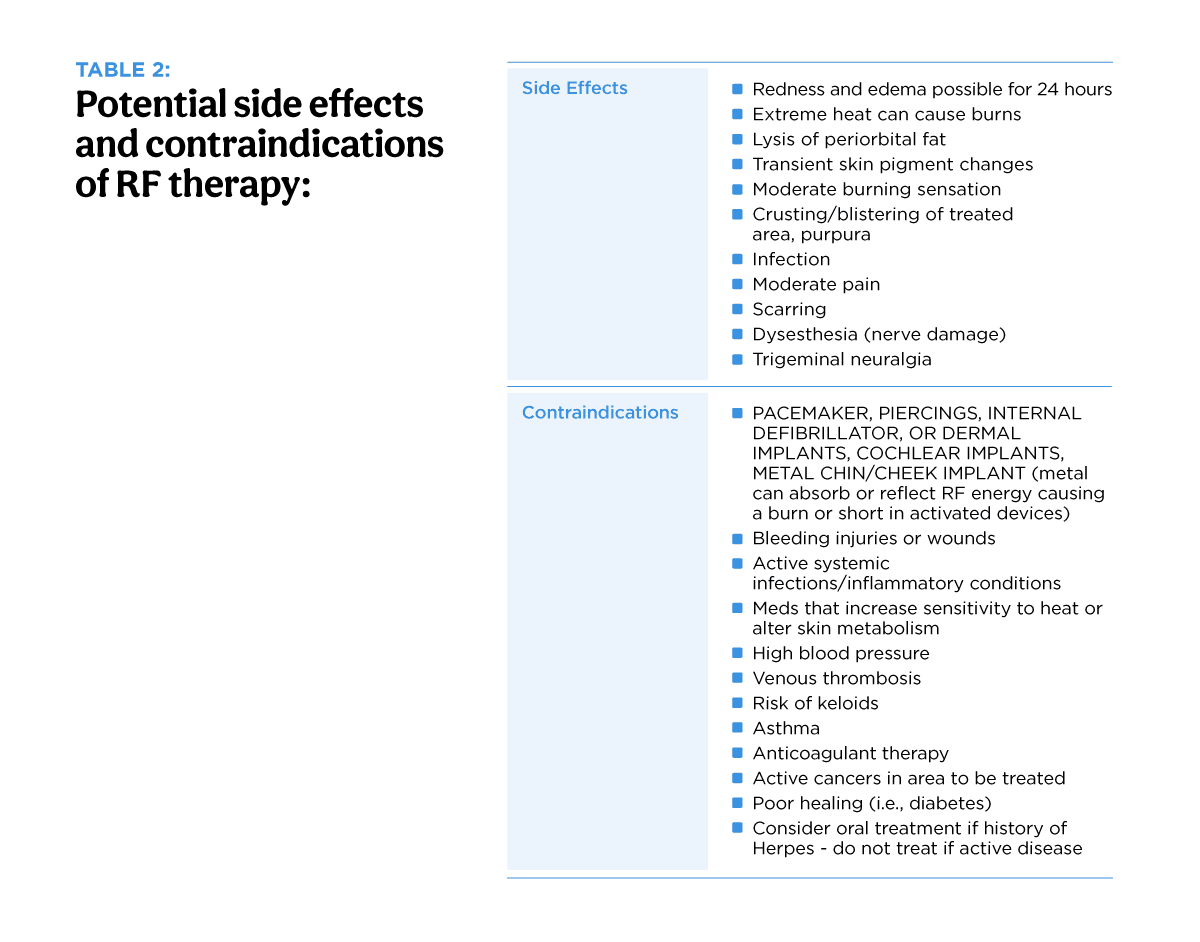
Radiofrequency (RF) therapy
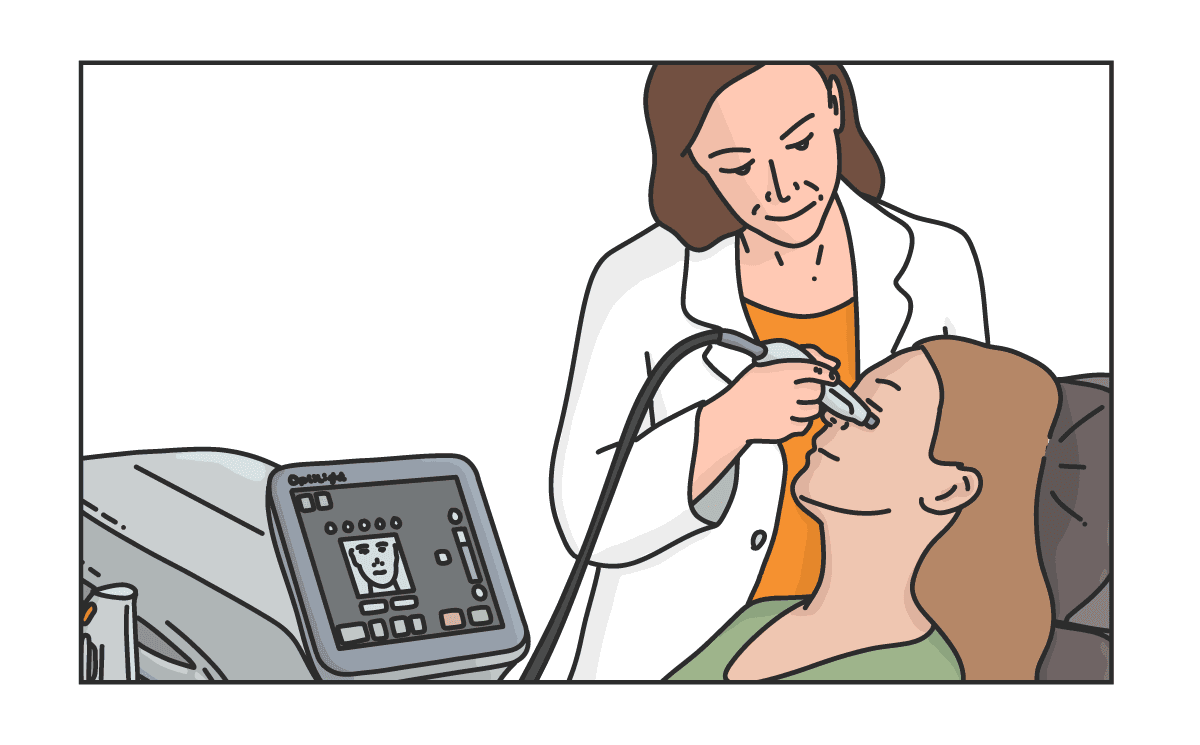
RF therapy, like IPL, is well-established in the field of dermatology. Unlike IPL, RF uses radio waves to heat the skin. Radio waves are generated when electrons move back and forth within an antenna. The RF dielectric heating principle involves exposing tissue water to an alternating electric field between two electrodes.
When RF energy is passed into tissue, the (+) charged sides of water molecules are attracted to the (–) current, while the (–) charged sides of water molecules are attracted to the (+) current. Since the current alternates rapidly, the water molecules change position, causing them to rotate. This resistance transforms electrical energy into heat.46
When applied to periorbital skin, heat and pressure can melt the meibum, reduce inflammation, and decrease laxity of the eyelid skin, potentially improving blink efficiency and lid closure.
Generally, treatments are every 2 to 6 weeks. Changes can be seen in 2 to 6 months, and the effects can last 1 to 3 years.47 RF improves skin tone, texture, firmness, and sun damage and reduces fine wrinkles. It works on all sexes and skin tones. However, RF is not effective on severely sagging skin (i.e., younger patients often have better results).

Thermal systems
Vectored thermal pulsation specifically refers to one commercial instrument (LipiFlow; Johnson & Johnson, Jacksonville, FL) that simultaneously produces heat on the inner surface of the upper and lower eyelids, combined with automated externally vectored and pulsed pressure to target obstructed meibomian glands.
Two other devices in the category of in-office thermal systems (TearCare, Sight Sciences, Inc, Menlo Park, CA & iLux, Alcon, Forth Worth, TX) heat the outer eyelids but require manual application of pressure.48 All of these devices work by heating the inner or outer eyelid surface to a temperature sufficient to melt meibum. The practitioner then expresses the meibum to fully evacuate the gland contents.
Like microblepharoexfoliation, thermal gland expression should be done early and frequently. Delaying treatment until the meibomian glands have atrophied and the ocular surface inflammatory sequelae have become moderate to severe results in the need for multiple treatment sessions before the meibum normalizes.
These devices are generally considered safe; while it is possible that a patient may experience a corneal or conjunctival abrasion during the treatment or that they may feel the treatments are subjectively “too hot” for them (although there is an upper limit to the amount of heat they can generate), it is quite rare to experience a serious adverse event.
Patient education is likewise important. Unless patients engage in regular home care, the meibomian glands will quickly become obstructed again, particularly if patients use computers, wear contact lenses (which potentially impair blinking), or use cosmetics.38,49
Lotilaner ophthalmic solution 0.25%
In addition to device-based treatments for eyelid disease, such as blepharitis and MGD, there also now exists a prescription option as well in the form of lotilaner ophthalmic solution (Xdemvy), the first and only FDA-approved treatment for Demodex blepharitis. Demodex blepharitis (DB) is a common condition seen in as many as 25 million eyecare patients and accounts for nearly ⅔ of all cases of blepharitis.50,51
Demodex mite overpopulation can result in inflammation of the eyelids and ocular surface, lash changes, and MGD.35,49,52,53 Lotilaner kills Demodex mites through inhibition of mite-specific GABA-gated chloride channels, which results in paralysis and death.54,55,56
The use of lotilaner twice a day for 6 weeks has demonstrated a reduction in collarettes (the proinflammatory waxy, cylindrical buildup of debris at the base of the eyelashes that is pathognomonic for DB) and mites, as well as improvement in meibomian gland function in patients with DB-associated MGD, and symptoms of itching, redness, and fluctuating vision.52,58,57,60
Factors affecting patient selection
It is no longer sufficient to say a patient has “dry eye” without further specification; rather, we may find that they, in fact, have MGD, blepharitis, corneal hyperalgesia, contact lens overwear, and inadequate lid closure. Patients will understand the need for multimodal therapy much better when their disease is put into this context.
In addition, each contributory condition must be staged. Is the MGD simply mild gland obstruction or near-total gland atrophy? Is the corneal hyperalgesia restricted to the afferent nerves, or is there a centralized component? Has the patient been overwearing their contact lenses for 2 years or 50 years? Can they stop lens wear or do they have keratoconus? Is the lagophthalmos 0.5mm or 3mm? Is osmolarity just a bit above normal or very high?
The patient needs to be given proper expectations regarding what to expect in terms of improvement and how long it will take to make them feel better. Many of the patients I see in my office have already been treated by numerous eye doctors, yet very few of them have had an honest conversation about their prognosis for recovery.
Patient demographics also play a role in crafting a management strategy. Older patients are going to have more severe disease but may have dexterity or vision issues or a high existing medication burden that prevents them from engaging in care. On the other hand, younger people who have subclinical disease may be unwilling to invest time or money into a condition that is not yet causing discomfort.
Conclusion
Treating dry eye has become more complicated as our understanding of its multifactorial nature has matured and the array of treatment options has ballooned. Navigating treatment is hampered by the unfortunate fact that newer medications are often not covered by insurance, and in-office treatments are rarely covered by insurance.
It is critical to have up-front discussions about what is available for an ideal management plan versus what is financially feasible for the individual patient. Most often, we have to pick and choose precisely what therapy will give the patient the greatest benefit with the least financial burden.
Patients who are “self-pay” will generally expect to have significant immediate benefit, but this may be unrealistic. It is our job to educate our patients on the expected time course and prognosis for symptomatic relief in the management of dry eye disease.

