Digital screen-related ocular and visual symptoms have quickly crept to the top of the most common chief complaints during a routine eye exam. The COVID-19 pandemic and the subsequent introduction of stay-at-home mandates, virtual learning, and remote working environments led to global lifestyle disruptions and a dramatic increase in screen time across all age groups.
Dealing with the new digital norm
The new digital norm poses a unique challenge for eyecare practitioners (ECPs): accurately addressing the
steep ocular and visual demands of a digital lifestyle for our patients. It can be challenging to discern the root cause of the screen-related symptoms and whether to attribute them to digital eye strain, digital dry eye, or both.
“Understanding the physiology underlying digital eye strain is imperative to create a paradigm shift in how ECPs treat and manage symptoms.”
Asthenopia is the diagnostic term for eye strain, and the cause of digital device-related asthenopia is multifactorial.1 Symptoms may be induced by uncorrected refractive errors, accommodative and/or oculomotor anomalies, and dry eye resulting from abnormal blinking and increased corneal exposure during computer viewing.2 This article will examine the relationship between digital eye strain and dry eye with special regard to how each leads to the other.
What is digital eye strain?
The American Optometric Association defines digital eye strain as the combination of eye and vision problems that result from the prolonged use of computers and other digital devices.3 It is estimated that approximately 60 million people worldwide suffer from digital eye strain, with a million new cases occurring each year.4
Studies show that up to 90% of computer users experience visual symptoms after prolonged computer use, with a higher prevalence shown in those who view screens for 2 or more continuous hours per day.3,5,6
The most commonly reported visual symptoms include eye strain, eye fatigue, ocular discomfort, burning, sore eyes, headaches,
diplopia, difficulty focusing, and blurred vision.
1 In a review of asthenopia, Sheedy et al. found that symptoms can be categorized into two groups that link them to their inducing conditions, termed internal and external symptom factors.
1,7The pathophysiology underlying eye strain
Describing symptoms based on location and sensation can attribute them to one of two distinct pathophysiologic processes.
1 Thus, a detailed
chief complaint and history are imperative to accurately diagnosing and treating screen-related asthenopia.
| Descriptors | Internal symptoms | External symptoms |
|---|
| Symptoms | Strain, ache, headache, blur, double vision | Burning, irritation, tearing, dryness |
| Location | Behind the eyes | Front and bottom of eyes |
| Causes | Refractive errors, accommodative anomalies, vergence disorders, presbyopia | Reduced blink rate, change in inter-blink duration, incomplete blinking, increased corneal exposure, corneal drying from environmental factors |
Internal symptom factors (ISFs) of asthenopia
The internal symptoms of strain, ache, headache, blurred vision, and diplopia are linked to uncorrected refractive, accommodative, or
binocular vision anomalies.
1 Patients may describe ISF sensations of pressure, pain, or soreness as being located behind the eyes or as a frontal headache.
1External symptom factors (ESFs) of dry eye
The external symptoms of burning, irritation, tearing, and dryness experienced on the front and/or bottom of the eyes are related to
dry eye.
1 Digital dry eye is induced by abnormal blinking, including a reduction in blink rate, reduction in blink amplitude, changes in blink patterns, and increased palpebral fissure due to a superior viewing angle.
8Primary causes of digital eye strain
Asthenopic symptoms result from many factors associated with prolonged digital screen use, including close viewing distance, mixed astigmatism, squinting to compensate for uncorrected refractive error and glare, decreased accommodative ability, development of
heterophoria at a near task, and near point of convergence removal.
1,4The most common oculomotor anomaly that contributes to eye strain is accommodative infacility, diagnosed by the inability to complete 20 cycles in 90 seconds using a +/-1.50D flipper.9
The results of research conducted by Sheppard et al. suggest that the weakness of these important visual functions could actually be the main culprit behind eye strain.1
The visual demand of the digital era
Prolonged viewing of text on a visual display terminal (VDT) is more demanding than reading printed physical text.4 Viewing pixelated letters clearly for a prolonged duration involves continuous relaxation and contraction of the eye muscles, resulting in eye fatigue.4
VDT letters are made up of pixels that are brightest at their center with decreasing brightness towards the periphery.4,10 Compared to printed material, reading on a VDT requires continuous focusing and refocusing of the ciliary body to maintain focus on pixelated characters.4,6,10
Shorter digital screen distance, a constant convergence requirement, high accommodative demand, and frequent saccadic eye movements further exacerbate asthenopic symptoms.
4,6 Due to the high visual demand of computer and digital device use, spherical
myopia and
hyperopia should be corrected to reduce the stimulus to accommodation.
1 Additionally, astigmatic errors should be fully corrected to reduce unwanted symptoms.
9Research on the effects of astigmatism on digital eye strain shows that 0.50 to 1.00 diopters of residual uncorrected astigmatism in spherical contact lens wearers are clinically significant enough to produce an increase in symptoms.9 Symptoms can be reduced by fitting spherical contact lens wearers in toric contact lenses or by using spectacles over top contact lenses during computer use.9
The ISF symptoms of strain, ache, and headache are distinct from those associated with dry eyes. A full assessment of the accommodative and binocular vision system is warranted to determine the underlying cause.1
Dry eye and digital eye strain
Contrary to ISF, ESF is highly related to dry eye symptoms caused by a reduction in blink rate and amplitude, change in blink patterns, tear film abnormalities, and increased corneal exposure in up gaze.
9 Dry eye may be exacerbated by VDT factors such as glare, small font, and flickering.
9Disrupted blink patterns
Perhaps the biggest player in the pathophysiology of digital dry eye is the disruption in blinking, which leads to alterations in the tear film that ultimately damages the ocular surface. Digital device use has been shown to cause alterations in blink patterns and an inhibited blink reflex that gives way to dry eye conditions.9 Healthy blinks are vital to maintaining the integrity of the precorneal tear film.11
The precorneal tear film, though heterogeneous in actuality, is traditionally broken down into three main layers: the anterior lipid layer formed by meibum from the meibomian glands, the aqueous layer secreted by the lacrimal gland, and the innermost mucin layer that covers corneal epithelial cells with mucin secreted by conjunctival goblet cells.11
Blinking is necessary for constant lubrication, as it stimulates the secretion of both tears and the aqueous mucin glycoprotein, redistributes the tear film over the ocular surface, assists the drainage of tears, and facilitates the expression of lipids from the meibomian glands.8,11 With each blink, a “jet” of oil from the lipid layer is secreted onto the tear film surface, giving it an anti-evaporative property.11
Blink reflex and gaze angle
Digital device use disrupts the blink pattern and reduces the frequency and amplitude of blinks.11 Studies have shown that as little as 45 minutes of computer use can reduce blink rates by 57%.4 Computer users adopt a superior gaze angle that hinders the blink reflex and results in a greater exposed ocular surface area and subsequent tear evaporation.1 The blink reflex is blocked by the fusion of the fibrous sheaths of the superior rectus and levator palpebrae superioris muscles in high visualization angles.1
Increased corneal exposure in the gaze angle results in corneal epithelium injury, stimulating nerve endings responsible for symptoms of dryness and discomfort.4
Additionally, to fixate and focus for a prolonged period, blinks are inhibited from high cognitive demand or low-legibility conditions.4 Low legibility can result from visually disruptive glare, small font size, low contrast, flicker, and poor resolution.4,12 The use of high contrast and larger font size may help the visual system process information easier and faster, reducing the amount of time spent looking at a screen without blinking.7
Tear film abnormalities found in digital device users
Ocular surface and tear film abnormalities, including reduced tear stability and tear volume, altered tear composition, and
meibomian gland dysfunction, have been found in computer users and are exacerbated with longer durations of device use.
13 The alterations in tear composition include increased oxidative stress markers and inflammatory mediators.
13To evaluate ESF-inducing conditions, the use of ophthalmic dyes such as lissamine green, sodium fluorescein, and rose bengal are indicated to assess tear film stability and corneal desiccation.
“Meibography is also a vital tool to assess structure and function of the meibomian glands contributing to evaporative dry eye.”
Since the symptoms of digital eye strain and digital dry eye are often conflated, it is imperative to explore the relationship between these two separate conditions that can exacerbate one another to create unwanted symptoms for the patient.
How does digital eye strain cause dry eye?
Digital eye strain may lead to dry eye symptoms due to eyelid squint. Digital viewers adopt a squint response to compensate for uncorrected
refractive error and minimize screen glare.
7Poor viewing conditions, including glare, poor resolution, and flicker, cause a contraction of the orbital portion of the orbicularis oculi muscle, which causes eyelid squint in an attempt to improve vision.7 Sheedy et al. found that squinting increases the visual acuity in the presence of uncorrected refractive error and decreases the retinal illumination in the superior visual field.1
Squinting not only contributes to symptoms of asthenopia but also negatively impacts the blink rate.9 As measured using electromyography (EMG) of the orbicularis oculi, greater squint levels cause a greater blink rate reduction.1,7
Pre-existing dry eye is exacerbated by reduced blinking,
contact lens wear, and increasing age, particularly in females. Environmental conditions such as excessive air conditioning and computer-generated heat may also contribute to dry eye symptoms.
4,12Conversely, how does dry eye lead to digital eye strain?
Pre-existing dry eyes with an unstable tear film can bring on symptoms of digital eye strain more rapidly and with increased severity. A study by Saldanha et al. explored the impact of the
COVID-19 pandemic on eye strain and dry eye symptoms. Patients with moderate dry eye, especially those with Sjögren's, experience the impact of increased eye strain to a greater extent than individuals with mild dry eye.
14 The most reported symptoms were increased eye pain, headache, and difficulty concentrating.
14“Exposure to short-wavelength blue light may also play a factor in producing visual symptoms specifically in individuals with reduced tear break-up time (TBUT) dry eye.”
Although there is no conclusive data on blue light’s role in digital eye strain, studies show that
blue light-blocking glasses may improve visual impairment associated with tear instability.
15 In a study conducted by Kaido et al., 22 patients with reduced TBUT dry eye and 18 healthy controls underwent functional visual acuity examinations with and without wearing 50% blue light-blocking lenses.
15 The study revealed that blocking 50% of blue light emission resulted in significant improvement in both mean functional visual acuity and visual maintenance in the dry eye group, while no significant changes were observed in the control group.15 Thus, suppression of blue light may be useful in improving visual function in dry eye patients.
Case report
The following case is of a 28-year-old female with symptomatic
dry eye and digital eye strain. The patient reports ISF of frontal headaches and pain behind the eyes, ESF of burning and stinging on the front of the eyes, and transient blurred vision during and after prolonged screen use. The patient has a dry eye Standard Patient Evaluation of Eye Dryness (SPEED) score of six.
Medical history
The patient’s medical history is significant for a 6-month course of Accutane in 2017. Also, the patient’s pre-existing ocular history is significant for nocturnal lagophthalmos, incomplete blink, and hyperopic
astigmatism. The patient self-reports digital screen time of around 8 hours per day on three different digital devices, listed in order of most to least usage: iPhone, iPad, and desktop computer. The causative factors of the symptoms may be found using Sheedy’s method of categorizing the symptoms by ISF and ESF.
Results from testing
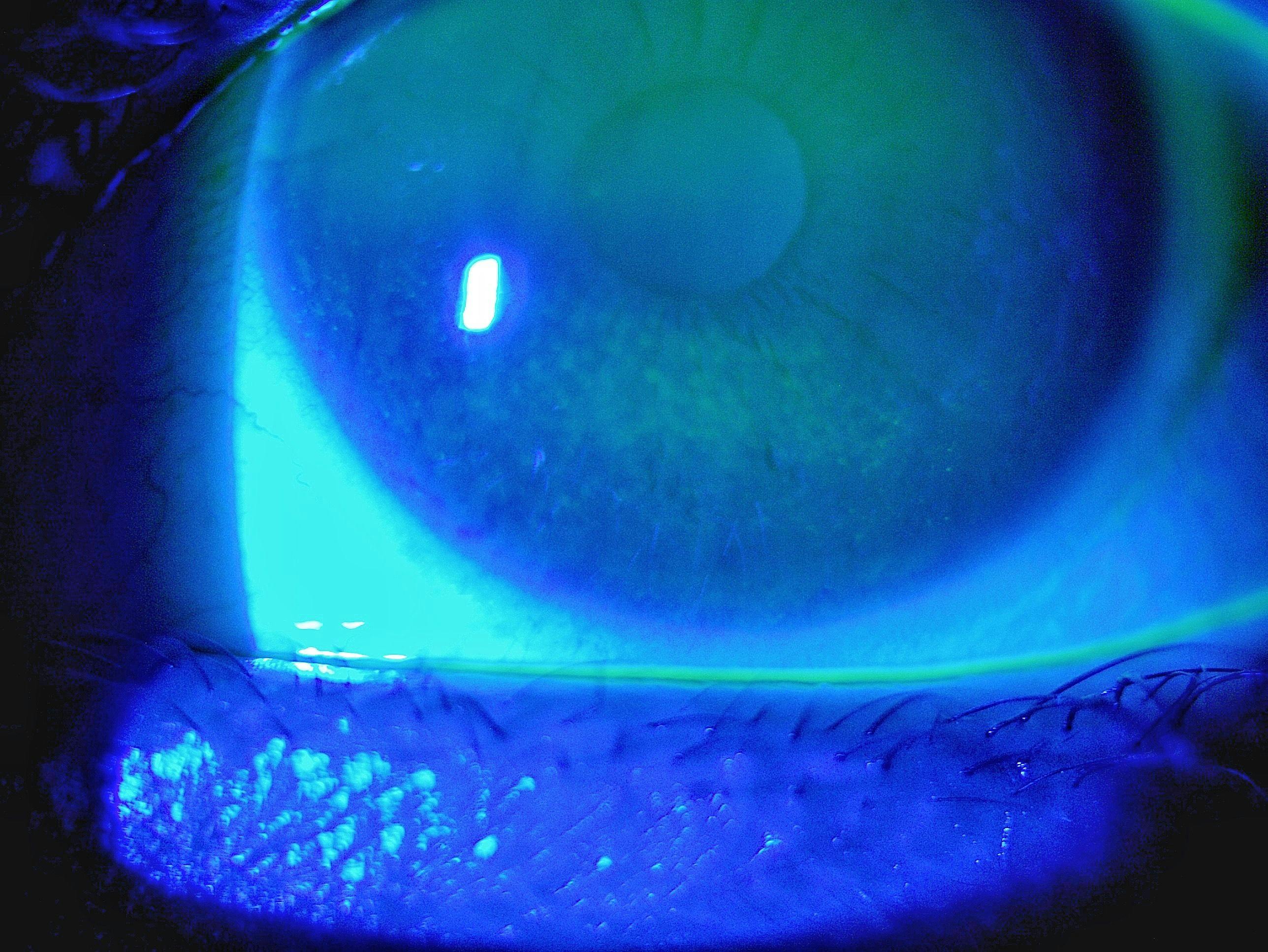
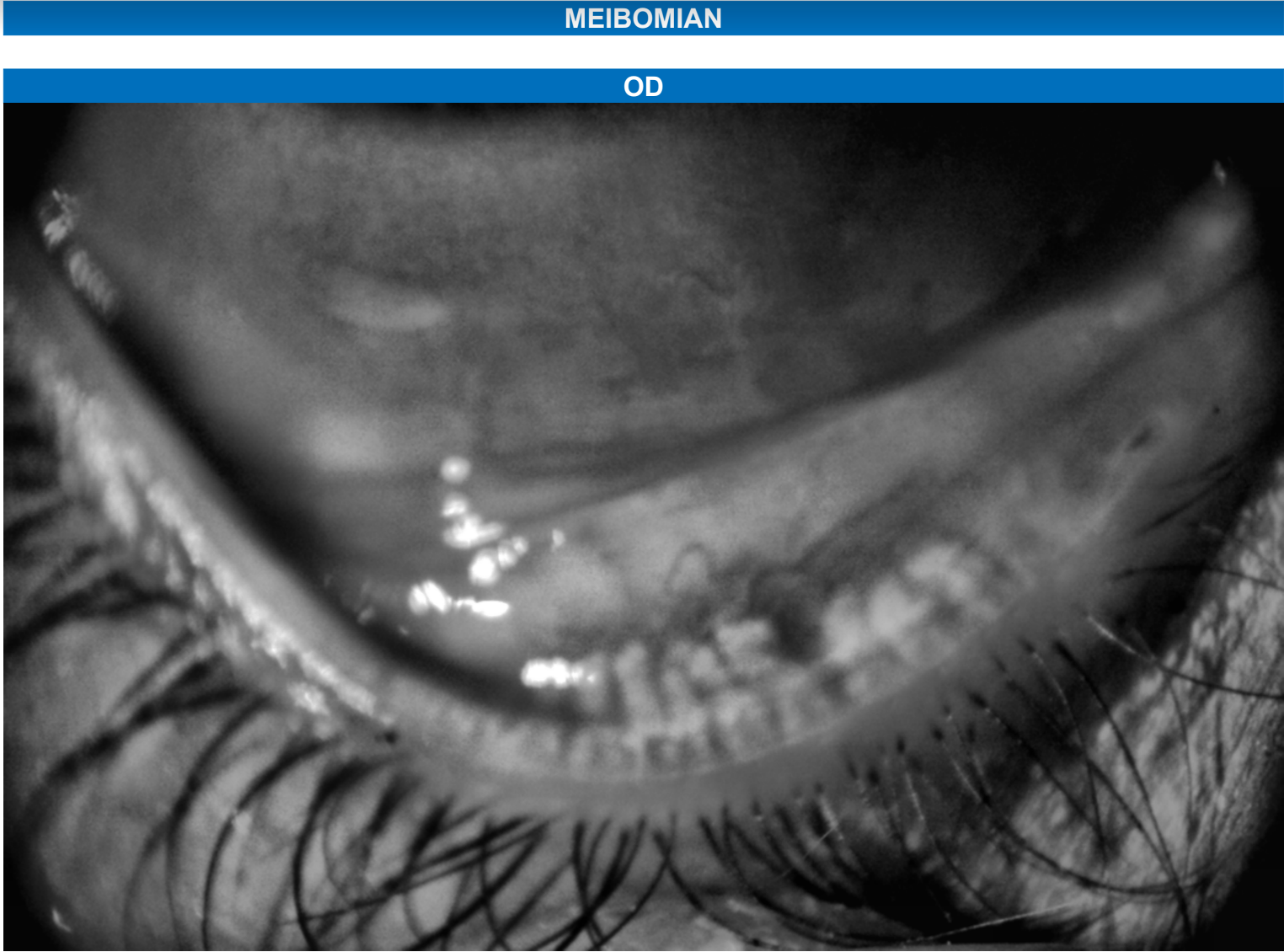
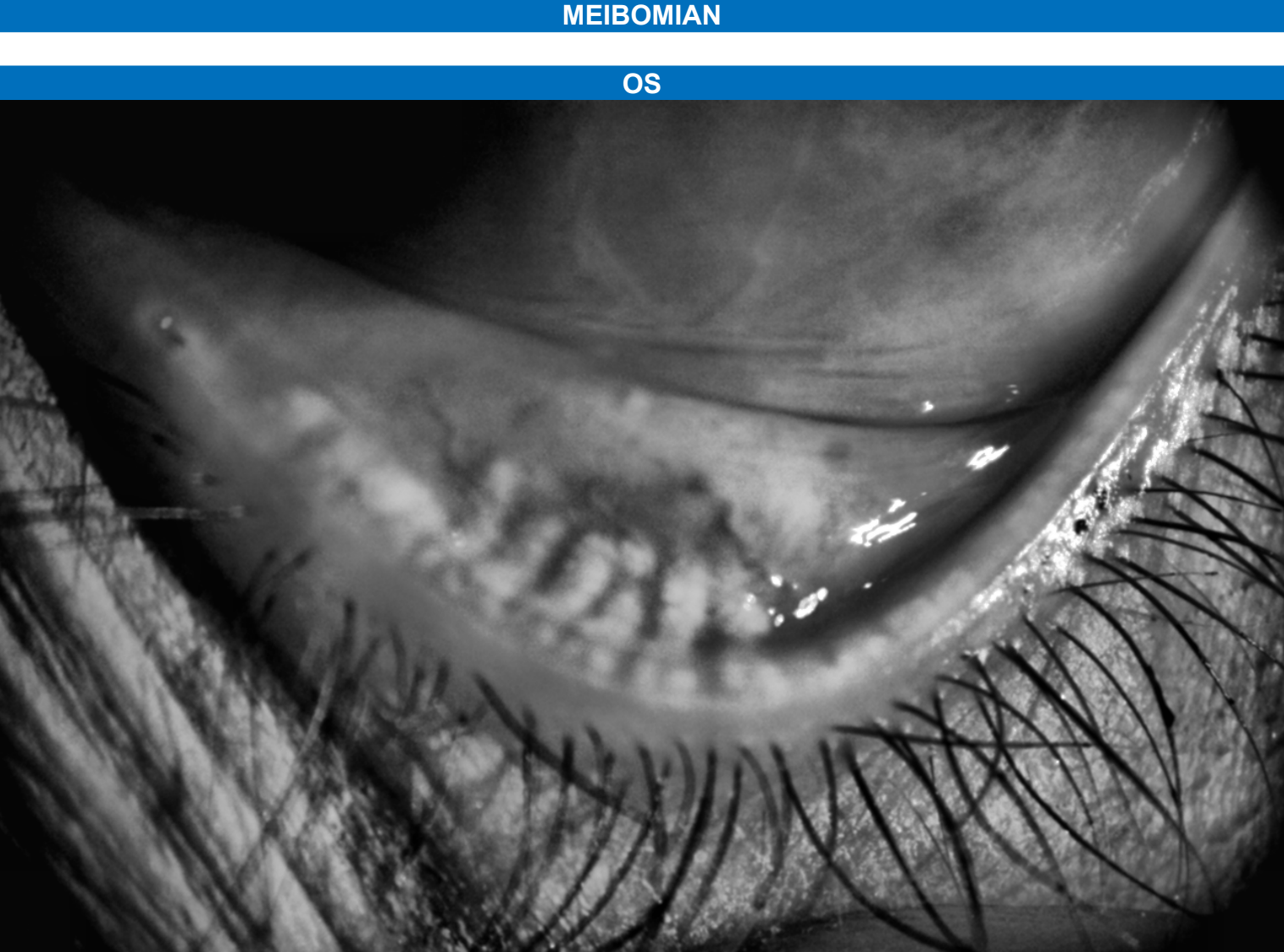
Refractive testing revealed hyperopic astigmatism, and binocular testing is significant for reduced positive relative accommodation (PRA), reduced flipper cycles per minute (cpm), and mild esophoria at near. Slit lamp examination revealed corneal staining with sodium fluorescein +1 SPK of the inferior ⅓ cornea (Figure 1) and a tear break-up time of 3 seconds OU. Meibography reveals meibomian gland dropout of the nasal meibomian glands of the lower lids and overall meibomian gland truncation (Figures 2 and 3), presumed to be caused by Accutane.
Figure 1 shows inferior corneal staining with sodium fluorescein.
Figure 1: Image courtesy of Jaskiran Kaur, OD
Figures 2 and 3 feature meibography imaging that reveal meibomian gland dropout OD and OS, respectively.
Figure 2: Image courtesy of Jaskiran Kaur, OD
Figure 3: Image courtesy of Jaskiran Kaur, OD
Diagnosis and treatment
The patient was diagnosed with evaporative dry eye and accommodative spasm. The treatment approach for external symptom factors of dry eye includes in-office IPL and an at-home maintenance regimen consisting of
omega-3 fatty acid supplements, lipid-based preservative-free artificial tears, a preservative-free nighttime ointment, and eyelid tape while sleeping.
The patient’s internal symptom factors of frontal headaches associated with accommodative spasm and refractive error are treated with prescription lenses with a base-out prism and blue light blocking to decrease unwanted glare from digital devices.
| Symptoms | Underlying conditions | Findings | Treatment |
|---|
| Internal symptom factors | Frontal headache, pain behind eyes | Hyperopia, astigmatism, accommodative spasm, esophoria | Refractive error: +1.25-1.25x178 OD, +1.00-1.00x002 OS, reduced PRA, reduced flipper cpm, 3 BO esophoria | Prescription glasses with base-out prism and blue-light blocker |
| External symptom factors | Burning, stinging | Evaporative dry eye, lagophthalmos, incomplete blink | SPK inferior ⅓, truncation and atrophy of meibomian glands, reduced TBUT of 3 seconds OU | Lipid-based artificial tears and ointments, omega-3 supplement 2000mg, eyelid tape while sleeping, intense pulsed light |
Digital eye strain patient education
The American Academy of Pediatrics (AAP) guidelines suggest no screen time for toddlers until 18 to 24 months (excluding video chatting), up to 1 hour a day for preschoolers, and no more than 2 hours per day for older children.16
| Age | Recommended screen time per day |
|---|
| Under 18 months old | No screen time outside of video chatting |
| Toddlers: 18 to 24 months old | Little to no screen time |
| Preschoolers: 3 to 5 years old | Up to 1 hour |
| Elementary school: 6 to 10 years old | Up to 1.5 hours per day |
| Middle school: 11 to 13 years old | Up to 2 hours per day |
All pediatric patients and their parents should be asked questions about daily screen time, digital habits, and
time spent outdoors. Based on the responses, patients and their parents should be educated on recommended screen time based on AAP guidelines, appropriate working distance for each digital device used, digital hygiene, and the importance of outdoor time to promote the healthy development of the visual system.
Developing digital hygiene habits
All patients with digital eye strain complaints should undergo a
complete case history using intake forms and questionnaires, such as SPEED, to properly inquire about digital device use and to screen for dry eye.
Digital device intake forms should include the following information:12
- Number and type of devices used
- Duration of use for each device
- Viewing distance and gaze angle of each device
- Monitor size and number of monitors
- Type of task being performed on each device
- The size of critical detail being observed during the task
Patients of all age groups should be counseled on establishing “digital hygiene” routines that focus on limiting screen time, increasing the number of breaks during prolonged work periods, increasing time spent distance viewing to offset near work, appropriate working distance, and proper workplace ergonomics.
Patients should be educated on the 20-20-20 rule: every 20 minutes, the viewer focuses on an object 20 feet in the distance for 20 seconds. Some patients may have demanding work where frequent breaks may not be realistic. For these patients, a 15-minute break after 2 hours of continuous computer use may be implemented.3
An etiological perspective on treatment
Due to the
multifactorial nature of dry eye and digital dry eye and eye strain, different treatment modalities are designed to meet the demands of patient-specific lifestyles.
Treatment options include full correction of refractive error and accommodative and binocular vision anomalies, evaporative dry eye treatments, and proper workplace ergonomic practices.4,6 The list below includes a list of potential treatment options for the ISF and ESF that contribute to asthenopic complaints related to digital screen use.
- Refractive error, binocular and accommodative anomalies: Most recent and accurate prescription glasses or daily disposable contact lenses, prism and low add for near work if necessary. Anti-fatigue lenses (Neurolens, Sync)
- Filters and tints: blue light blocker to help regulate circadian rhythm and decrease blue-light scatter, yellow tint to increase contrast
- In-office evaporative dry eye treatments: IPL, Tearcare, Lipiflow, iLux
- At-home dry eye maintenance regimen: omega 3 fatty acid supplements, warm compress, lipid-based preservative-free artificial tears, gels, and ointments, moisture-chamber goggles
- Preventative treatments: proper workplace ergonomics, 20/20/20 rule, a window near the desk, daily disposable contact lenses, cool-mist humidifier, eyelid hygiene
Workplace ergonomics
The list below includes a list of ocular ergonomic guidelines for computer users:17
- The distance between the eyes and the screen should be approximately arm’s length, at least 20 to 25 inches.
- The recommended gaze position of the eye to the screen should be slightly below eye level. Ideally, the center of the screen should be about five to six inches below the straight-ahead gaze.
- A downward gaze position is favored over an upward gaze position to reduce corneal exposure and tear evaporation.
- Overall, room lighting should be enhanced and adjusted to keep overhead lighting to a minimum.
- Contrast should be increased, and text size should be enlarged to reduce the visual demand for digital text.
- Monitor display quality should be increased by using high-resolution LCD monitors with a matte finish to minimize flicker. A matte screen filter can be used to reduce glare.
- Regular screen time breaks should be practiced. The AOA suggests the 20-20-20 rule.
- Alternatively, a 15-minute break after 2 hours of continuous computer use may be implemented for those who cannot take more frequent breaks.
- Glasses are preferred to correct refractive, binocular, or accommodative errors instead of contact lenses.
- If contact lenses must be worn, daily disposable lenses are preferred, and astigmatism should be fully corrected.
- An artificial humidifier on the cool-mist setting may improve localized moisture.
Closing thoughts
While the widespread use of screens has placed an enormous workload on the visual system and ocular surface, the digital age shows no sign of slowing down. ECP’s responsibility to accurately
address and manage screen-related symptoms is made simple using Sheedy's method of categorizing the symptoms by ISF and ESF.
By viewing digital eye strain through an etiological lens, customized solutions can be created to meet patient-specific needs. Furthermore, educating patients on digital hygiene empowers them to become more mindful of their digital habits.