




Telemedicine, a term derived from "telecommunication" and "medicine," is a healthcare delivery method that uses electronic communication and information technologies to provide clinical services to patients remotely.
The concept of telemedicine dates back to the early 20th century when radio and telephone were used to offer medical consultations. Over the years, telemedicine has significantly evolved, particularly with the introduction of the Internet and video communication, making it accessible and efficient.1
Recently, telemedicine has increased in popularity, primarily due to the COVID-19 pandemic, allowing patients to receive healthcare services from the comfort of their homes.
Telemedicine in eyecare
Telemedicine has made remarkable advancements in the field of eyecare. It is precious for routine screenings and consultations. Ophthalmologists and optometrists can remotely diagnose and monitor ocular conditions using high-resolution images and videos of the eye.
This is particularly beneficial for patients in remote or underserved areas and those with limited mobility. Tele-ophthalmology has also found applications in triage, allowing specialists to prioritize urgent case presentations.
Moreover, it plays a vital role in managing chronic eye diseases, such as glaucoma and diabetic retinopathy, by facilitating routine check-ups and early intervention. With the integration of artificial intelligence (AI), the accuracy and efficiency of tele-ophthalmology will continue to improve, making it a valuable tool in eyecare services.
Overview of diabetic retinopathy
Diabetic retinopathy is an ocular complication seen in patients with diabetes secondary to damaged retinal blood vessels and ischemia. Of note, diabetic retinopathy is the leading cause of blindness in adults. People with diabetes have a more than 20 times increased risk of blindness than those without diabetes.
The prevalence of diabetic retinopathy is significant, with approximately one in three diabetics developing some degree of the condition.2 The increasing prevalence of diabetic retinopathy will likely result in an increased demand for screening.
This may affect the ability of eyecare professionals to provide traditional in-person dilated fundus examinations promptly.
The prevalence of diabetic retinopathy
The prevalence of diabetic retinopathy increases with the duration of the disease. According to the American Academy of Ophthalmology (AAO), it is recommended that people with type 1 diabetes have routine dilated fundus exams starting 5 years after diagnosis and at the time of diagnosis for people with type 2 diabetes.3 After that, retinal exams every 1 to 2 years are recommended.3
According to the Centers for Disease Control (CDC), only 40% of diabetes patients receive the recommended dilated eye exams.4 Barriers to care may include patient education, cost, transportation, lack of symptoms, and refusal of pupillary dilation.
Ocular complications of diabetes
Sight-threatening complications of diabetes in the retina include bleeding, macular edema, exudation, ischemia, and neovascularization, which may lead to vitreous hemorrhage or retinal detachment.
Some treatment options for these conditions include intravitreal injections, laser photocoagulation, and sometimes more invasive surgical techniques (i.e., vitrectomy), which rely on early detection for optimal visual outcomes.
In its early stages, diabetic retinopathy often presents asymptomatic, which is why routine eye exams are crucial for individuals with diabetes. As the disease progresses, symptoms may include blurred vision, the appearance of floaters, and even complete vision loss in severe cases.
Diagnosing diabetic retinopathy
Diabetic retinopathy is traditionally diagnosed through a comprehensive eye examination by an ophthalmologist or an optometrist.
This typically includes a dilated eye exam and supportive imaging techniques such as fundus photography, optical coherence tomography (OCT), and fluorescein angiography when needed to assess further and identify leakage or neovascularization.5
Early detection and management of diabetic retinopathy are vital in preventing its progression and preserving vision.
Conducting tele-ophthalmic diabetic screenings
Tele-ophthalmic diabetic screenings are conducted through remote imaging technology and telemedicine to assess the eye health of individuals with diabetes. The process typically begins with a patient visit to a local healthcare facility, where trained personnel use specialized non-mydriatic equipment to capture high-resolution images and videos of the patient's fundus.
These images are obtained using fundus cameras or other ophthalmic imaging devices that focus on the vitreous, optic nerve, macula, blood vessels, retina, and choroid to the extent captured.6 Once the images are acquired, they are securely transmitted to an eyecare specialist at a remote location.
These experts then evaluate the images to identify signs of diabetic retinopathy and stage appropriately. Following this analysis, the eyecare provider can provide a tentative diagnosis and recommend appropriate follow-up, including an in-person dilated examination or referral to a retina specialist for proper management.
Tele-ophthalmic diabetic screenings are especially valuable for reaching individuals in remote or underserved areas, increasing access to essential eyecare, and helping to prevent vision loss through early detection and intervention.7
The impact of telemedicine on public health and accessibility
Tele-ophthalmic diabetic screenings have a significant current and potential future impact on public health and accessibility. Currently, they play a role in improving access to eyecare services for individuals with diabetes, especially in underserved or remote areas where access to eyecare is limited.
With more than an 80% sensitivity, these screenings enable early detection of diabetic retinopathy.8 This allows for timely intervention and treatment, essential in preventing vision loss.
They also reduce the need for frequent in-person visits, making eyecare more convenient and cost-effective for patients. During the COVID-19 pandemic, tele-ophthalmic screenings gained even more relevance, providing a safer way for patients to receive essential eyecare while minimizing the risk of exposure.
AI and diabetic retinopathy screening
In the future, the impact of tele-ophthalmic diabetic screenings is likely to grow. As technology advances, the quality and efficiency of remote eye imaging will improve, enhancing the accuracy of diagnoses.
Moreover, the integration of deep learning as a method of AI via artificial neural networks is being created to analyze retinal images. These algorithms can detect subtle abnormalities associated with diabetic retinopathy. As deep learning improves its ability to interpret complex visual data, it is expected to play an increasing role in eyecare.9
Considerations for implementing tele-screenings
Integrating tele-screenings into a medical practice requires careful consideration of several vital factors. First, it's essential to ensure compliance with relevant legal and regulatory requirements, including patient data privacy and telemedicine licensure. Practitioners must also invest in secure and Health Insurance Portability and Accountability Act (HIPAA)-compliant telehealth technology to protect patient information.
Additionally, selecting appropriate equipment and training staff to conduct tele-screenings effectively is crucial. Ensuring the quality and reliability of the telehealth equipment, such as fundus cameras, is necessary to produce accurate results.
Staff should be trained to use this equipment proficiently and assist patients during screening. Creating clear protocols and workflows for conducting tele-screenings, transmitting and storing patient data, and consulting with remote specialists is vital to maintaining an efficient process.
Attention should also be given to reimbursement policies and insurance coverage for tele-screenings. Finally, enhancing patient education and engagement is vital to increase awareness and promote participation in these remote screenings.10
Potential limitations of tele-ophthalmology
While tele-ophthalmology holds promise as a valuable tool for remote eyecare, it is essential to acknowledge the potential limitations that it may have. One of the primary concerns is the proficiency and training of technicians who capture images and information during virtual consultations.
Inadequate technician training can lead to inaccuracies and missed details crucial for diagnosis. Additionally, the image quality in tele-ophthalmology can be compromised, raising concerns about the accuracy of findings and the ability to detect subtle abnormalities.
Some conditions, such as cataracts or vitreous hemorrhages, may affect the clarity of the images. Using non-mydriatic cameras may only sometimes suffice, as some instances require mydriasis to achieve optimal photo quality. Retinal cameras with ultra-widefield imaging capability should be considered.
Also, the postural limitations of patients in a remote setting can pose challenges, potentially affecting the angle and view necessary for a thorough evaluation.11 Recognizing and addressing these limitations is necessary to ensure the reliability of tele-ophthalmology.
Diabetic retinopathy telehealth case report
A 46-year-old African American male with a history of uncontrolled non-insulin dependent diabetes mellitus, diagnosed 8 years prior, underwent diabetic retinopathy screening by telemedicine.
Retinal photos were captured via a digital non-mydriatic retinal camera by a trained technician in the primary care clinic and electronically sent to the eye clinic for analysis. Per chart review, he was dilated yearly for the past 4 years with no evidence of diabetic retinopathy in either eye.
Tele-retinal imaging findings
Upon review of tele-retinal imaging, anterior segment photos were unremarkable in both eyes (OU). Retinal photos were of good quality, with minimal artifacts and shadowing to the extent captured. The vitreous appeared clear OU. His optic discs were well-perfused and distinct without hemorrhage, pallor, edema, or neovascularization.
His retinal vasculature appeared tortuous, with mild crossing changes in his right eye (OD) more significant than in his left eye (OS). It broadened the arteriolar reflex, as seen in poorly controlled diabetics and hypertensives.
There was a microaneurysm in his macula (challenging to appreciate) and a single dot hemorrhage nasally OD (Figure 1). Multiple dot/blot hemes, as well as microaneurysms (also difficult to value), were noted OS (Figure 2).
As there was no documented patient history or visual acuities and we could not reach the patient via telephone, a letter was sent recommending a follow-up dilation in our clinic within 3 months, or sooner if loss or change in vision.
Figures 1 (OD) and 2 (OS) illustrate moderate non-proliferative diabetic retinopathy as seen in a Canon non-mydriatic fundus photo.


Figure 1: Courtesy of Michelle D’Amura, OD, FAAO.


Figure 2: Courtesy of Michelle D’Amura, OD, FAAO.
Follow-up visits and treatment
The patient was seen in our general clinic 2 months later, and a dilated fundus exam and imaging confirmed moderate non-proliferative diabetic retinopathy without clinically significant macular edema OU.
His visual acuity was 20/20 OD and 20/25 OS at that visit. He was educated extensively on associated risks, stressed medication compliance, and lifestyle changes, and a 6-month follow-up was recommended.
Unfortunately, our patient had poor medication compliance and was often lost to recommended follow-up. Of note, 5 years after his initial tele-retinal image, he returned to the clinic with subjective floaters OS.
Severe non-proliferative diabetic retinopathy OD (Figure 3) and proliferative diabetic retinopathy OS with neovascularization of the disc and vitreous hemorrhage (Figure 4) were seen on dilated fundus examination. Visual acuity was 20/20 OD and reduced to 20/40 OS.
He has since been treated with intravitreal injections and panretinal photocoagulation appropriately by our retina specialist, and his vision recovered to 20/20 OU.
Figures 3 (OD) and 4 (OS) demonstrate Optos fundus photos showing severe non-proliferative diabetic retinopathy.


Figure 3: Courtesy of Rachel Goretsky, OD.

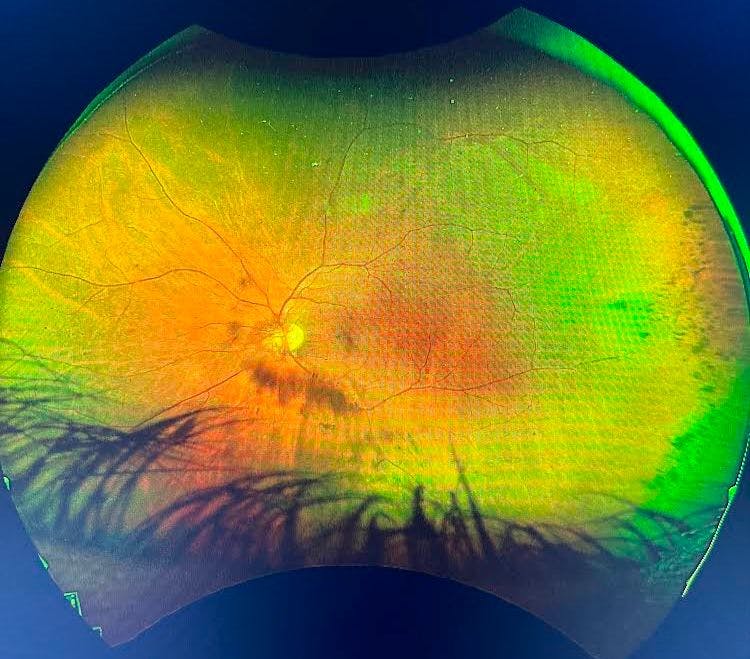
Figure 4: Courtesy of Rachel Goretsky, OD.
Conclusions
The evolution of tele-ophthalmic diabetic screenings represents a transformation in healthcare delivery.
This innovative approach not only enhances access to essential eyecare services, particularly for individuals with diabetes, but also has the potential to reduce health disparities and improve public health outcomes.
As technology progresses, the future of tele-ophthalmology appears promising, with even greater accuracy and efficiency on the horizon.
