Intravitreal and subretinal injections: current approaches to suprachoroidal therapy
Intravitreal and subretinal injections are two potential methods to administer treatments to the retinal pigment epithelial (RPE) cells and photoreceptors. However, both treatment modalities have their potential advantages and disadvantages, which may make injections to the suprachoroidal space (SCS) a novel and enticing approach to consider.
Intravitreal injections
Intravitreal injections are frequently and routinely done in-clinic and are commonly used to administer medications like
anti-VEGF treatments, antibiotics, or steroid medications. This quick and routine procedure has evolved over the past 20 years regarding technique and anesthesia.
This treatment method's risk of complications, such as
endophthalmitis and inflammation, remains very low. Their effect may be limited due to the internal limiting membrane (ILM), which restricts the transduction of treatment particles to the outer retinal layers. It also results in a more potent humoral immune response than subretinal delivery.
Subretinal injections
Subretinal injections require taking a patient to the operating room. It is an invasive surgery involving vitrectomy and injection of a bleb with a small gauge cannula into the subretinal space, creating a serous macular detachment. This allows for a focal region of therapeutic effect near the injection site. Because subretinal injections require surgery, this approach has not become commonplace.
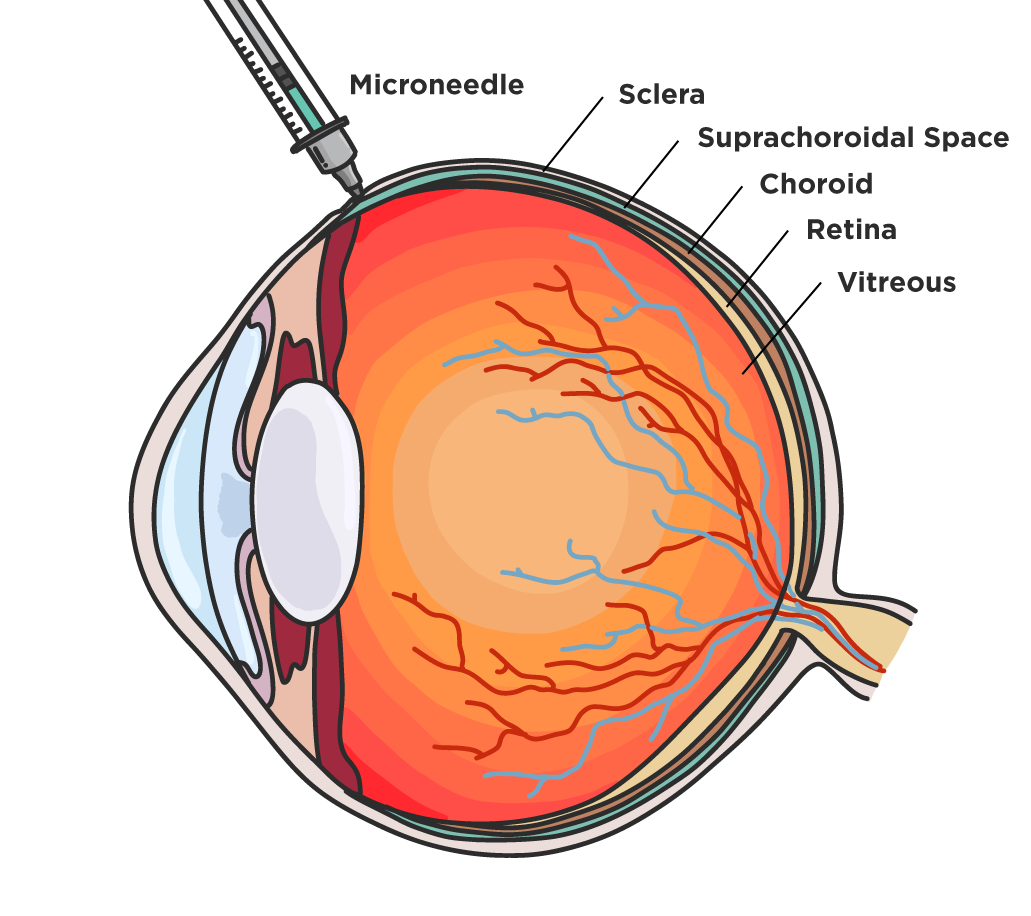
Suprachoroidal injections can be performed in-clinic using a 900- to 1100-micron needle to deliver treatments to a potential space between the sclera and choroid.
Suprachoroidal injections are advantageous because they produce diffused, peripheral effects in RPE cells. It achieves chorioretinal concentrations significantly greater than that seen with traditional intravitreal injections.
Delivery directly to the posterior segment reduces the drug’s exposure to the vitreous and anterior segments, potentially reducing the rate of intraocular pressure (IOP) increase, a common side effect of steroid injections. Additionally, the suprachoroidal approach avoids the need for vitrectomy, allowing for greater access to care with an in-office procedure, like intravitreal injections.
The suprachoroidal space in the past
Tanzanite study: suprachoroidal triamcinolone acetonide for branch retinal vein occlusions with macular edema
The Tanzanite study was a phase two, multicenter, randomized, masked, and active-controlled clinical trial sponsored by
Clearside Biomedical Inc.
1 This study assessed the safety and efficacy of a 4 mg suprachoroidal injection of triamcinolone acetonide (CLS-TA), in conjunction with intravitreal aflibercept, and it compared these results to treatment with aflibercept monotherapy.
Subjects targeted for treatment were those with macular edema secondary to retinal vein occlusion. This study comprised 46 patients between 14 sites from December 2014 through November 2015.
The subjects were randomly assigned to different groups in a 1:1 ratio to either the suprachoroidal injection of CLS-TA and aflibercept group or the sham suprachoroidal injection and aflibercept group. Each group was followed up to receive aflibercept injections as needed at months 1, 2, and 3.
The primary efficacy endpoint was based on the number of aflibercept retreatments required by each patient belonging to each respective group through the end of the third month. Secondary outcomes were measured as the mean improvement from baseline best-corrected visual acuity, central subfield thickness (CST), and the percentage of the subjects with a CST of <310 um at each measured time point.
The results reported 23 retreatments in the combination group and nine in the monotherapy group (P=0.013). The percentage of participants that did not need any retreatments also increased, with 78% being in the combination therapy group and 30% being in the monotherapy group (P=0.003).
When comparing the best-corrected visual acuity between the combination and monotherapy groups, respectively, it was: 16.1 and 11.4 at the end of the first month (P=0.20), 20.4 and 11.9 at the end of the second month (P=0.04), and 18.9 and 11.3 at the end of the third month (P=0.09).1
The mean baseline CST went from 731.1 um to 284.7 um by the end of the first month in the combination group. In the subsequent 2 months, it held stable at 272.4 um and 285.4 um.
For the monotherapy group, the baseline was 727.5 um, decreasing to 322.8 um by the end of the first month, and increasing to 383.4 um and 384.6 um at the end of months one, two, and three, respectively. Edema resolution in the combination therapy group improved 87.0%, 87.0%, and 78.3% by the end of months 2, 3, and 3. In the monotherapy group, edema was improved by 56.5%, 47.8%, and 47.8% by the end of months 1, 2, and 3.
The combination therapy group improved overall, resulting in a decreased need for additional intravitreal aflibercept treatments over the three months studied compared to the monotherapy group.
The procedures were well tolerated, with only one participant in the combination group having progression of a preexisting cataract, and four with increased IOP that was well-managed with topical medication.1
HULK trial: suprachoroidal triamcinolone acetonide for diabetic macular edema
The HULK trial was a phase one and phase two study of suprachoroidal space delivery of triamcinolone acetonide.
2 This study was designed to observe any improvement in patients' eyes with
diabetic macular edema (DME).The study consisted of two groups: the first group was the treatment-naïve group (n=10), and the second group was the previously treated group (n=10). The treatment-naïve group received a single injection of IVT aflibercept and suprachoroidal CLS-TA, with a total of 2.6 mean injections of CLS-TA. Conversely, the previously treated group received only suprachoroidal CLS-TA monotherapy, with a total mean of 3.3 CLS-TA injections.
Between the two groups, at 6 months there was a mean best-corrected visual acuity (BCVA) of +8.5 ETDRS letters, mean CST reduction of 91 um in the treatment-naïve group, and mean BCVA change of +1.1 and 128 um reduction of CST in the previously treated group.2 Adverse effects resulted in two patients with an increased IOP, three patients with cataract progression, one case of local pain during the procedure, and one case of accidental IVT injection.
While the numbers seemed to have improved with this therapy, there was a return to baseline within 1 month of treatment. There was no lasting improvement with the studied treatment, halting the trials from progressing past phase one/two.
TYBEE study: suprachoroidal triamcinolone acetonide and intravitreal aflibercept for diabetic macular edema
TYBEE was a study to compare the treatment of DME using intravitreal aflibercept in conjunction with suprachoroidal CLS-TA versus intravitreal aflibercept monotherapy.3 The study design was a randomized, double-masked, parallel-design, and controlled study with an active group of 36 eyes and a control group of 35 eyes.
At 24 weeks, the mean BCVA of the combination therapy group resulted in 11.8 ETDRS and a mean CST decrease of 212.1 um.3 The monotherapy group had a BCVA of 13.8 ETDRS and a mean CST decrease of 178.6 um.
There was an average of 2.6 treatments for the joint therapy group, with complications being increased IOP in three patients and cataract development in two patients. There was an average of 4.6 treatments with the monotherapy group, with complications including one patient with an increase of 10 mmHg from baseline IOP, and one with cataract development.
The results showed similar effects on vision and the safety of the treatments in both groups. This study did not go beyond phase two due to the similarity of the two groups.
The suprachoroidal space today
Xipere (Bausch + Lomb) is a new FDA-approved suprachoroidal triamcinolone acetonide 40 mg/mL injection used to treat macular edema secondary to posterior
uveitis.
9 It is the first and only treatment approved for delivery to the suprachoroidal space.
PEACHTREE trial: suprachoroidal triamcinolone acetonide for macular edema secondary to posterior uveitis
Xipere was studied in PEACHTREE, a phase three trial involving 160 patients.9 In this trial, macular edema was defined as intraretinal or subretinal fluid with a retinal thickness of 300 um or more in the central subfield. Patients had a best-corrected visual acuity of 5 or more and 70 or fewer ETDRS letters. The distribution of anterior, intermediate, posterior, and panuveitis was comparable between the treatment and control groups.
Patients were randomized 3:2 for suprachoroidal triamcinolone versus sham injections administered at day 0 and week 12. Patients in the suprachoroidal triamcinolone group were administered 4 mg suprachoroidal injections in a single eye.9 The sham group underwent a sham procedure without the drug. Patients were followed every 4 weeks up to week 24.9
The primary endpoint was an improvement in BCVA of 15 or more ETDRS letters in week 24. The trial met the primary endpoint, with 47% of patients in the CTS-TA group gaining 15 or more letters, compared to 16% in the control/sham group. In the CLS-TA group 60% of participants gained 10 or more letters, which was true for 30% of those in the sham group. In addition, 76% and 39% in the CLS-TA and control groups gained five or more letters, respectively.
The trial also met its secondary endpoint, which saw the central macular thickness reduced by 153 um in the CLS-TA group, compared to only 18 um in the sham group. Two-thirds of patients with active inflammation at the beginning of the study in the CLS-TA group experienced resolution at 24 weeks.
Of the patients, 13.5% versus 72% needed rescue treatment in the CLS-TA and the control group, respectively, with the median time for the first rescue being 89 days for the CLS-TA group, versus 36 days in the sham group.9 There was a 30% incidence of adverse effects in the treatment group versus 12.5% in the control group.
Adverse events included only cystoid macular edema in the control group and eye pain and elevated eye pressure in both groups.9 The incidence of cataracts was comparable between both groups, at 7.3% and 6.3% in the treatment and control groups, respectively.9
MAGNOLIA trial: an extension study to PEACHTREE
In an extension of the phase three trials (MAGNOLIA), the time to rescue was evaluated over an additional 24 weeks.10 Twenty-eight patients from the CLS-TA, and five from the sham group, were enrolled. The extension study found the median time to rescue therapy to be 257 days in the CLS-TA group, versus 55.5 days in the sham group.10
This study showed that 50% of the patients in the CLS-TA group did not require rescue for 9 months after the second injection.10 In patients who did not require rescue, there was a CST reduction of 174.5 um, and a gain of 12.1 letters at 48 weeks. The median time to rescue patients treated with Xipere (n=28) was 344 days, showing good durability for Xipere. Of the patients treated with Xipere, 50% completed the study by reaching the Week 48 visit without rescue medication.
AZALEA study: suprachoroidal triamcinolone acetonide for active and inactive non-infectious uveitis
The AZALEA study also examined SCS administration of triamcinolone acetonide (CTS-TA) in non-infectious uveitis (NIU).8 Unlike PEACHTREE, AZALEA included active and inactive NIU. Patients were treated with two doses of 4 mg 12 weeks apart.8 After 24 weeks, the treatment was well tolerated.8
There was a modest improvement of the mean BCVA from a baseline of 68.9 to 75.9 at week 24.8 The mean CST at baseline was 335.9, and decreased by 15% to 284.0 at week 24.8 Additionally, 70 to 80% of subjects with macular edema had a reduction in retinal thickness by more than 20%.8
Overall, the study showed the efficacy and safety of CLS-TA, with a low likelihood of IOP elevation and cataracts, which is similar to the results seen in the PEACHTREE study.8,9
The future of the suprachoroidal space
Gene therapy
The standard method for
gene therapy is to directly deliver the vector to RPE and photoreceptors.
4 This is done in the OR by doing a vitrectomy, retinotomy, and injection to the subretinal space. This creates a temporary and limited retinal detachment.
SCS administration of vectors does not require detachment of photoreceptors and RPE, thus limiting the iatrogenic effects on the compromised retina.4 Preclinical studies show acceptable results when comparing SCS and subretinal injections.5
REGENXBIO is developing a drug called
RGX-314 for gene therapy that targets the vascular endothelial growth factor (VEGF) by delivering a gene encoding a therapeutic anti-VEGF Fab protein.
AAVIATE trial: suprachoroidal therapy to treat wet age-related macular degeneration (REGENXBIO, Inc)
AAVIATE (NCT04514653) is a phase two trial examining RGX-314 in treating
wet age-related macular degeneration (AMD).12 Recently, the company announced it had completed enrollment in cohort five in the trial.
12 The study examines suprachoroidal injections' efficacy, safety, and tolerability using a Clearside SCS Microinjector.12 RGX-314 is an adeno-associated virus that encodes antibody fragments that inhibit VEGF.
12Cohort one was randomized 3:1, with the treatment group receiving 2.5x1011 genomic copies of RGX-314, versus monthly 0.5 mg Ranibizumab intravitreal injections.12 Cohort two and three treatment groups received 5x1011 genomic copies.12 Cohorts four and five received 1x1012 genomic copies.12 The 20 patients enrolled in cohort five are Nab-positive. The company announced that it expects results by the end of 2022.
In addition to AAVIATE, the drug is also being studied in patients with
diabetic retinopathy in phase two dose-escalation trials, to determine its efficacy, safety, and tolerability (ALTITUDE, NCT04567550).
13There are three cohorts in the study, with cohort one and two being randomized, and cohort three receiving the drug.13 Cohort one will receive dose one, and cohorts two and three will receive dose two of RGX-314.13 The study is expected to be completed in June 2023.
Melanoma
AU-011 is a light-activated virus-like particle made of phthalocyanine dye, and is being studied to treat
choroidal melanoma.
6,7 It binds selectively to cancer cells through a modified heparan sulfate proteoglycan on the tumor cell surface.
6,7 This therapy results in cell membrane disruption and cancer necrosis.
6,7 The drug is being studied in the phase two clinical trial examining SC administration.
14 Retinal implants
Argus II is a prosthetic retinal implant that stimulates inner retinal neurons, restoring vision in patients with severe vision loss.
6,7 However, implantation is associated with complications related to location and surgical techniques.
6,7 Potential implantation into the SCS would reduce the chances of disrupting fragile retinas in patients with severe degeneration.6,7 The first human trials showed improved light localization, but were complicated with subretinal and suprachoroidal hemorrhage.6,7
Retinal detachment repairs
SCS can also relieve traction from peripheral
retinal breaks in rhegmatogenous detachments and the repair of myopic foveoschisis.
6,7 These often involve complications related to silicone bands for scleral buckling.
6,7 However, there is a risk for choroidal hemorrhage.
6,7Conclusion
Suprachoroidal treatment delivery is in an exciting research phase and has many advantages related to drug bioavailability and durability. Clinical trials show promising results in the safety and efficacy of drug delivery to the SCS.
It also avoids complications related to intravitreal injections and subretinal injections. SCS can potentially be an innovative way of treating many diseases, including uveitis, melanoma, and gene therapy.
References
- Campochiaro, P. A., Wykoff, C. C., Brown, D. M., Boyer, D. S., Barakat, M., Taraborelli, D., & Noronha, G. (2017, July 17). Suprachoroidal triamcinolone acetonide for retinal vein occlusion ... Retrieved August 1, 2022, from https://clearsidebio.com/wp-content/uploads/2021/10/Campochiaro_et_al_Ophthalmol_Retina_2017Oct10_Suprachoroidal_triamcinolone_acetonide_for_retinal_vein_occlusion_-_results_of_the_Tanzanite_study.pdf
- Lampen SIR, Khurana RN, Noronha G, Brown DM, Wykoff CC. Suprachoroidal Space Alterations Following Delivery of Triamcinolone Acetonide: Post-Hoc Analysis of the Phase 1/2 HULK Study of Patients With Diabetic Macular Edema. Ophthalmic Surg Lasers Imaging Retina. 2018 Sep 1;49(9):692-697. doi: 10.3928/23258160-20180831-07. PMID: 30222804.
- Barakat MR, Wykoff CC, Gonzalez V, Hu A, Marcus D, Zavaleta E, Ciulla TA. Suprachoroidal CLS-TA plus Intravitreal Aflibercept for Diabetic Macular Edema: A Randomized, Double-Masked, Parallel-Design, Controlled Study. Ophthalmol Retina. 2021 Jan;5(1):60-70. doi: 10.1016/j.oret.2020.08.007. Epub 2020 Aug 20. PMID: 32829027.
- Campochiaro, MD, P. A. (2020, February 1). Suprachoroidal Gene Transfer. Retinalphysician.com. Retrieved July 20, 2022, from https://www.retinalphysician.com/issues/2020/special-edition-2020/suprachoroidal-gene-transfer
- Bo Tian, Jun Xie, Wenqi Su, Shuo Sun, Qin Su, Guangping Gao, Haijiang Lin; Suprachoroidal Injections of AAV for Retinal Gene Delivery in mouse. Invest. Ophthalmol. Vis. Sci. 2021;62(8):1177.
- Mehta, MD, N., & Yiu, MD, G. (2021, August 10). Therapeutics in the suprachoroidal space. Review of Ophthalmology. Retrieved July 18, 2022, from https://www.reviewofophthalmology.com/article/therapeutics-in-the-suprachoroidal-space
- Ciulla, MD, MBA, T. A., Andino, MSBE, MBA, R. V., & Hancock, MBA, S. (2022, August 1). Suprachoroidal Drug Delivery Technology. Retinalphysician.com. Retrieved August 3, 2022, from https://www.retinalphysician.com/issues/2022/special-edition-2022/suprachoroidal-drug-delivery-technology
- Henry CR, Shah M, Barakat MR, Dayani P, Wang RC, Khurana RN, Rifkin L, Yeh S, Hall C, Ciulla T. Suprachoroidal CLS-TA for non-infectious uveitis: an open-label, safety trial (AZALEA). Br J Ophthalmol. 2022 Jun;106(6):802-806. doi: 10.1136/bjophthalmol-2020-318019. Epub 2021 Feb 5. PMID: 33547034; PMCID: PMC9132856.
- Yeh S, Khurana RN, Shah M, Henry CR, Wang RC, Kissner JM, Ciulla TA, Noronha G; PEACHTREE Study Investigators. Efficacy and Safety of Suprachoroidal CLS-TA for Macular Edema Secondary to Noninfectious Uveitis: Phase 3 Randomized Trial. Ophthalmology. 2020 Jul;127(7):948-955. doi: 10.1016/j.ophtha.2020.01.006. Epub 2020 Jan 10. PMID: 32173113.
- Khurana RN, Merrill P, Yeh S, Suhler E, Barakat MR, Uchiyama E, Henry CR, Shah M, Wang RC, Kapik B, Ciulla T. Extension study of the safety and efficacy of CLS-TA for treatment of macular oedema associated with non-infectious uveitis (MAGNOLIA). Br J Ophthalmol. 2022 Aug;106(8):1139-1144. doi: 10.1136/bjophthalmol-2020-317560. Epub 2021 Mar 12. PMID: 33712478.
- Arshad M. Khanani; Suprachoroidal Delivery of RGX-314 Gene Therapy for Neovascular AMD: The Phase II AAVIATE™ Study. Invest. Ophthalmol. Vis. Sci. 2022;63(7):1497.
- REGENXBIO presents positive initial data from phase II AAVIATE® trial of RGX-314 for the treatment of wet AMD using suprachoroidal delivery and provides trial update at Retina Society 54th annual scientific meeting. REGENXBIO Inc. (n.d.). Retrieved July 25, 2022, from https://regenxbio.gcs-web.com/news-releases/news-release-details/regenxbio-presents-positive-initial-data-phase-ii-aaviater-trial
- RGX-314 gene therapy administered in the suprachoroidal space for participants with diabetic retinopathy (DR) without center involved-diabetic macular edema (CI-DME) - full text view. RGX-314 Gene Therapy Administered in the Suprachoroidal Space for Participants With Diabetic Retinopathy (DR) Without Center Involved-Diabetic Macular Edema (CI-DME) - Full Text View - ClinicalTrials.gov. (n.d.). Retrieved July 28, 2022, from https://clinicaltrials.gov/ct2/show/NCT04567550
- Phase 2 trial to evaluate safety and efficacy of AU-011 via suprachoroidal administration in subjects with primary indeterminate lesions and small choroidal melanoma - full text view. Full Text View - ClinicalTrials.gov. (n.d.). Retrieved July 28, 2022, from https://clinicaltrials.gov/ct2/show/NCT04417530