


Vertical Heterophoria (VH) is a vertical misalignment of the eyes which can lead to both ocular and systemic symptoms. A specialty-trained optometrist can use patient screening techniques to diagnose and microprisms to manage these patients. VH is estimated to affect at least 20% of the population.1
Pathophysiology of vertical heterophoria
Vertical heterophoria is a binocular vision dysfunction resulting from a vertical misalignment of the eyes. Vertical misalignments as small as 0.25 diopters may result in many vestibular and ocular problems.2 The body tries to correct for the error by overusing and straining the eye muscles to realign the eyes.
A vertical heterophoria can be genetic/developmental or can be acquired from a TBI/concussion, stroke, or other form of brain injury. Genetic/developmental vertical heterophoria may be due to vertical orbit asymmetry or asymmetric extraocular muscle (EOM) innervation or strength.3
Two forms of vertical heterophoria
There are two forms of vertical heterophoria: monocular or binocular. The monocular form is a malfunction of the visual system and is commonly recognized as a superior oblique palsy, and the solution is prism over the impacted eye. A superior oblique palsy can be genetic or acquired in head injuries or due to poor blood supply in systemic conditions like diabetes.4,5
In contrast, the binocular form has not been previously recognized and appears to be a vestibular system problem, most likely due to faulty eye alignment signals sent from the vestibular system through the vestibular ocular reflex (VOR).2
The visual system responds to the impending diplopia (possibly through the fusional vergence reflex) by trying to align the images. The faulty vestibular signal again asserts itself, which sets up a misalignment/realignment cycle, which occurs at a rapid frequency and is the cause of the patient's symptoms.
The overuse of the opposing elevator and depressor muscles trying to re-align the lines of sight results in muscle strain, a headache, asthenopia, and eye pain on eye movement. The rapid misalignment/realignment cycle is hypothesized to cause visual shimmering or sensation of image vibration, as well as dizziness and other vestibular-type symptoms.2
How to identify patients with a vertical heterophoria
The range of VH symptoms is vast and diverse. Typical symptoms include headaches, dizziness, anxiety, neck pain, reading/learning difficulties and balance/gait issues. A head tilt may be a sign of a VH.
Asking patients specific screening questions can identify vertical heterophoria suspects in your patient population. A survey instrument (Binocular Vision Dysfunction Questionnaire or BVDQ) has been developed and designed by the NeuroVisual Medicine Institute to assess the frequency of symptoms in patients with suspected VH.
Patients are screened for VH in five ocular and systemic categories.6
- Headache/Neck Ache
- Vestibular system symptoms
- Standard and binocular vision symptoms
- Psychological symptoms (anxiety)
- Reading/Learning symptoms
Once a possible VH patient has been identified, a specialized neurovisual evaluation is performed to determine if visual misalignment is present. The NeuroVisual Medicine Institute uses proprietary techniques to determine and treat patients with VH.
Treatment approaches to vertical heterophoria
Historically, diagnosing and treating vertical heterophoria has proven to be difficult.3 VH was first described by Stevens in 1887 and he had attempted to treat misalignment with 1.75D, 3.5D, 5.25D, and 7D of prism without much success.3 In the 1950s and 1960s Roy had success with much smaller units of prism, which has been reported by other clinicians.7,8
Determining the magnitude and orientation of the prism may be challenging. Typical tests like Von Graefe phoria testing, vertical vergence testing, red lens tests, and fixation disparity testing are not sensitive enough to identify and treat small vertical heterophorias.9
It may be helpful to perform multiple tests to confirm small amounts of deviation. Once you have identified a patient that has a vertical misalignment the best way to manage them is with a vertical compensatory prism.
Recommendations to identify a VH include the following tests:
1) Cover test
Helpful hint: It may be easier to look for small lid movement up or down vs. look at the actual eye.
2) Fixation disparity
Fixation disparity is a technique that measures the direction and magnitude of the vertical deviation under conditions where fusion is present. The amount of prism required to reduce the vertical alignment will resolve the patient’s symptoms.10
AO vectograph slide, Turville testing or Mallet card can be used to determine the associated phoria.9 Using testing results to determine distance and near associated phoria is another alternate way of prescribing.
In addition to these tests, observation of posture, balance, and gait is very useful in determining misalignment status. The Prism Challenge Technique is a useful approach for both diagnosis and treatment.2
What is a microprism, and how is it used?
A microprism is a small unit of prism. While the exact amount has not been defined, the term is commonly used for fractional units of prism, usually 0.5 diopters or less. Feinberg created the Prism Challenge Technique with the use of microprism to help alleviate VH. This technique uses 0.25 diopter lenses, and while working in free space incrementally adds them to a trial frame until visual clarity is maximized and symptoms are minimized.
The average patient experiences a 50% reduction of symptoms immediately during the initial evaluation and confirms the diagnosis. The first set of lenses allows the visual system to move away from the extreme tension and overuse it has been experiencing, and the EOMs begin to relax. This results in a prescription change, requiring that the amount of microprism and the other elements of the prescription be reassessed over several additional visits to maximize the patient’s symptom reduction.5
AO vectograph slide, Turville testing, or Mallet card can be used to determine the associated phoria.10 Using testing results to determine distance and near associated phoria is another alternate way of prescribing.
Distinguishing vertical heterophoria from other conditions
An evaluation for VH should be considered early with presenting symptoms of headache, dizziness, nausea, anxiety, learning challenges, and panic disorders, but only after serious conditions, such as a stroke or an intracranial mass are excluded as differentials.2
A VH evaluation by a specialist will determine if VH is a partial or the sole cause of the patient’s symptoms. The initial evaluation is 80 minutes, noninvasive, and the disorder is simple and affordable to treat.
If symptoms remain after the evaluation, other pathologies should be considered. VH shares common symptoms with other binocular vision disorders, ADHD, MS, strokes, inner ear disorders, migraines, Méniere’s Disease, and other systemic conditions.11 A comprehensive medical history is important to diagnosis including time of onset, additional symptoms, systemic medical history, and trauma.

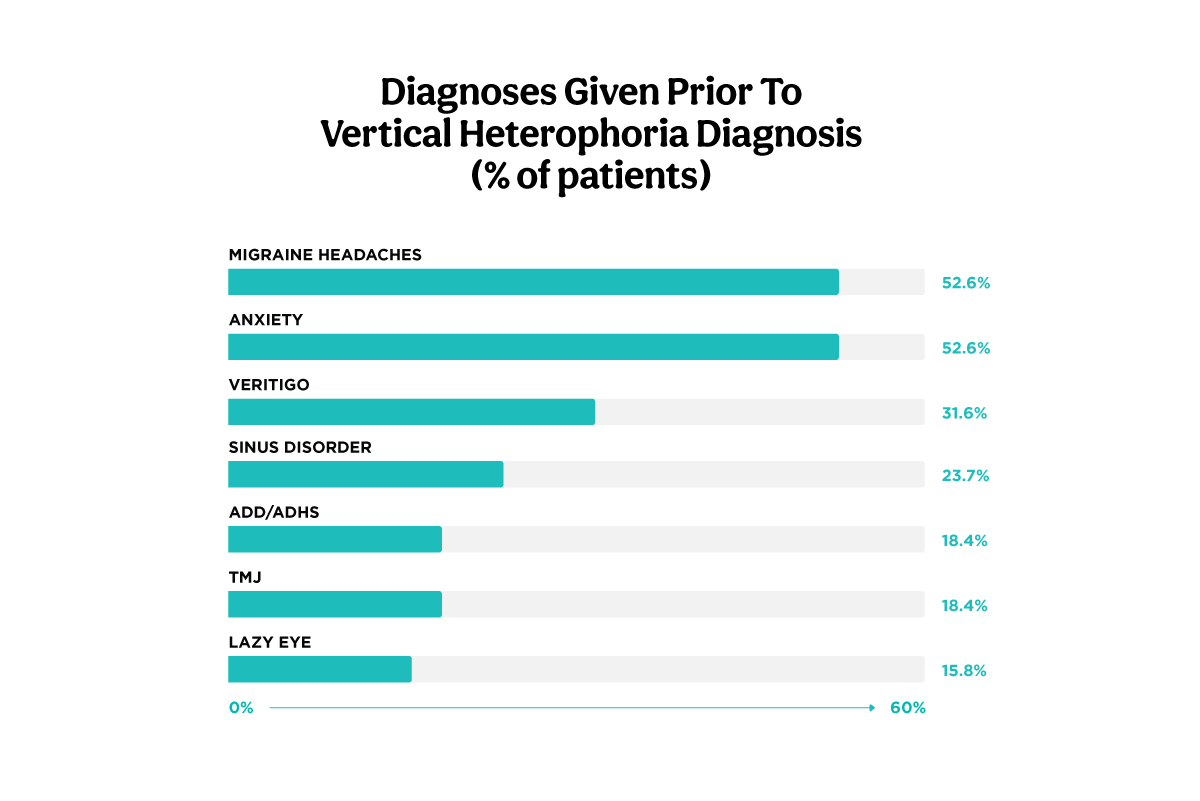
Figure 1: adapted from:vision-specialists.com
Vertical heterophoria vs. anxiety/ panic disorders
Patients with VH often have anxiety or panic when driving at high speeds on the freeway, in crowded environments, in wide open spaces with tall ceilings like malls, and in visually complex environments with patterned wallpaper or carpet. VH creates feelings of dizziness and anxiety causing the patient to feel they are no longer in control in some cases leading to agoraphobia.12 A VH evaluation using microprisms can confirm the diagnosis.
Vertical heterophoria vs. ADHD
ADHD shares similar symptoms to VH and is often misdiagnosed. Up to 50% of children with ADHD/ADD could be suffering from a binocular vision disorder. VH symptoms can lead to issues with learning and reading comprehension. Eye strain and fatigue can make reading and writing both frustrating and difficult for children.
Symptoms may vary according to the age of the child, but may include covering one eye while reading, skipping lines or losing place while reading, difficulty sitting still or focusing on schoolwork or bumping into things.6 Fine motor function can be impaired with BVD, possibly due to rapid misalignment/realignment cycles.11
Figure 2 illustrates a peacock drawn by a patient with vertical heterophoria.

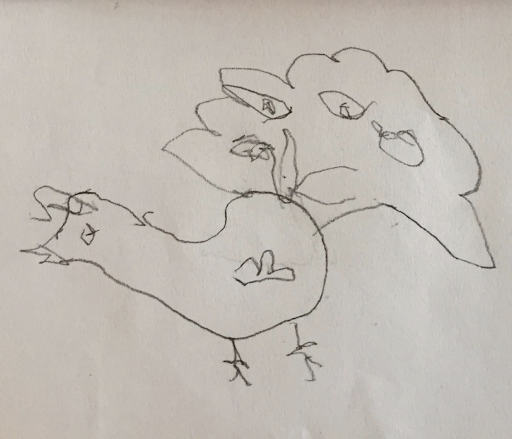
Figure 2
Figure 3 illustrates a peacock drawn by the same patient after the addition of microprisms.

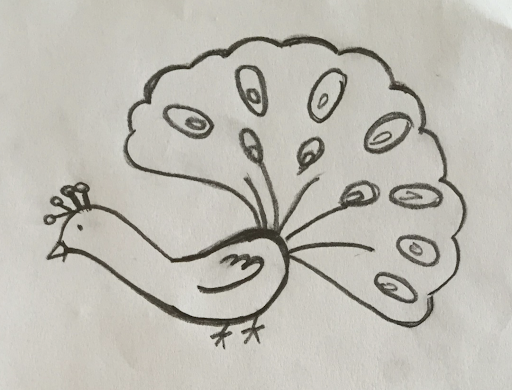
Figure 3
Vertical heterophoria vs. migraines
Besides headaches and nausea, patients with VH typically present with symptoms of dizziness, neck pain, and anxiety. The presence of a head tilt may be helpful in identifying headache sufferers who need a VH evaluation.2 Completing a comprehensive history regarding migraine symptoms including age of symptom onset, frequency of symptoms and headache triggers can help differentiate VH from migraines.
Vertical heterophoria vs. Ménière’s disease
VH and Ménière’s disease share common symptoms of dizziness and difficulty with balance. Ménière’s disease is a disorder of the inner ear which causes vestibular problems and hearing difficulties. Patients diagnosed with Ménières disease tend to be in their 40s to 60s and may experience sporadic attacks of hearing loss and vertigo.13
Patients with VH have routinely been evaluated by specialists like ENT’s, neurologists, and psychiatrists/psychologists due to common symptoms like headache, dizziness, and anxiety, yet did not experience adequate improvement of symptoms using traditional treatment approaches as the major cause of their symptoms is BVD.
Using validated screening instruments like the BVDQ, you can identify these patients in your practice and, if appropriately trained, treat them using the Prism Challenge Technique. You should expect for their symptoms to improve by at least 50% in your chair!2
References
- Surdacki M, Wick B. Diagnostic occlusion and clinical management of latent hyperphoria. Optometry & Vision Science 1991;68:261–269.
- Feinberg DL, Rosner MS, Rosner AJ. Vertical heterophoria treatment ameliorates headache, dizziness, and anxiety). Optometry and Visual Performance. 2020 March; 8:1-33.
- Feinberg, D. Practice Profile: Vision Specialists of Michigan. The Case for Vertical Heterophoria Care. Accessed from https://www.optometricmanagement.com/issues/2019/october-2019/the-case-for-vertical-heterophoria-care
- Doble, JE, Feinberg DL, Rosner MS, Rosner AJ. Identification of binocular vision dysfunction (vertical heterophoria) in traumatic brain injury patients and effects of individualized prismatic spectacle lenses in the treatment of postconcussive symptoms: a retrospective analysis. PM R. 2010 Apr;2(4):244-53. doi: 10.1016/j.pmrj.2010.01.011. PMID: 20430325.
- Ferris, J. Superior Oblique Palsy. American Academy of Ophthalmology. 2015. Retrieved from https://www.aao.org/basic-skills/superior-oblique-palsy
- Feinberg DL, Rosner MS, Rosner AJ. Validation of the binocular vision dysfunction Questionnaire (BVDQ). Otol Neurotol. 2021 Jan;42(1):e66-e74. doi: 10.1097/MAO.0000000000002874. PMID: 33105328.
- Wick BB. Prescribing vertical prism: How low can you go? J Optom Vision Dev 1997;28:77-85.
- Jackson DN, Bedell HE. Vertical heterophoria and susceptibility to visually induced motion sickness. Strabismus. 2012;20(1):17-23. doi:10.3109/09273972.2011.650813
- Schroeder TL, Rainey BB, Goss DA, Grosvenor TP. Reliability of and comparisons among methods of measuring dissociated phoria. Optom Vis Sci. 1996 Jun;73(6):389-97. doi: 10.1097/00006324-199606000-00006. PMID: 8807650.
- Scheiman, M., & Wick, B. (2002). Clinical management of binocular vision: Heterophoric, accommodative, and eye movement disorders. Philadelphia: Lippincott Williams & Wilkins.
- Rosner, M. S., Feinberg, D. L., Doble, J. E., & Rosner, A. J. (2016). Treatment of vertical heterophoria ameliorates persistent post-concussive symptoms: A retrospective analysis utilizing a multi-faceted assessment battery. Brain injury, 30(3), 311-317.
- Passamonti L, Toschi N. Lower Functional Connectivity in Vestibular-Limbic Networks in Individuals With Subclinical Agoraphobia. Front Neurol. 2019;10:874. Published 2019 Aug 13. doi:10.3389/fneur.2019.00874 (7)
- U.S. Department of Health, National Institutes of Health, Ménière's Disease. https://www.nidcd.nih.gov/health/menieres-disease. Published February, 2013. Accessed April 18, 2022.
